Abstract
Primary percutaneous coronary intervention is currently the standard of care for the treatment of acute ST-segment elevation myocardial infarction (STEMI). While it can restore flow in the infarcted artery in the majority of cases, some patients experience the so-called “no-reflow” phenomenon, which consists of abnormal myocardial reperfusion occurring after the occluded coronary artery has been opened. It is caused by microvascular obstruction (MVO), and its pathogenesis is multifactorial, including myocardial ischaemia, distal embolisation, and ischaemia-reperfusion injury, combined with individual susceptibility. Currently, there is no consensus on pharmacological or interventional strategies which can prevent or treat it. We herein discuss in detail the pathophysiology of the “no-reflow” phenomenon in STEMI patients, which is closely related to MVO, as well as potential pharmacological and interventional treatments tested in clinical studies.
No reflow and slow flow after percutaneous coronary intervention (PCI) are highly dynamic processes characterised by failure to adequately obtain microvascular reperfusion despite successful stent implantation in the epicardial coronary artery.1 Microvascular obstruction (MVO) – the pathological basis of these phenomena – was first described in 1948 by Harman and colleagues in albino male rabbits, and its impact on adverse clinical outcomes was highlighted more than two decades ago.234 It may occur in approximately 40-50% of patients undergoing PCI, with a higher incidence among patients with ST-segment elevation myocardial infarction (STEMI).4
MVO after successful stent implantation in epicardial coronary vessel reperfusion can be the result of an interplay of various factors: myocardial ischaemia, spontaneous or iatrogenic distal embolisation, reperfusion-related injury, and individual susceptibility. These factors contribute either to intravascular obstruction (e.g., endothelial cell swelling, platelet-neutrophil plugging, fibrin-thrombus generation, etc.) or to extravascular compression (e.g., myocardial oedema, cardiomyocyte swelling/hypercontracture, intramyocardial haemorrhage, pericyte contracture, etc.).
Over the last three decades, extensive efforts have been made to identify pharmacological and interventional approaches capable of preventing or treating this no-reflow/slow-flow phenomenon, as well as targeting MVO; however, to date, no therapy has been shown to consistently improve clinical outcomes.5
Against this background, this state-of-the-art review provides a comprehensive overview of the pathophysiological mechanisms underlying this phenomenon, as well as invasive and non-invasive diagnostic tools, and finally, pharmacological and interventional treatments, highlighting the clinical gaps in the field (Central illustration).
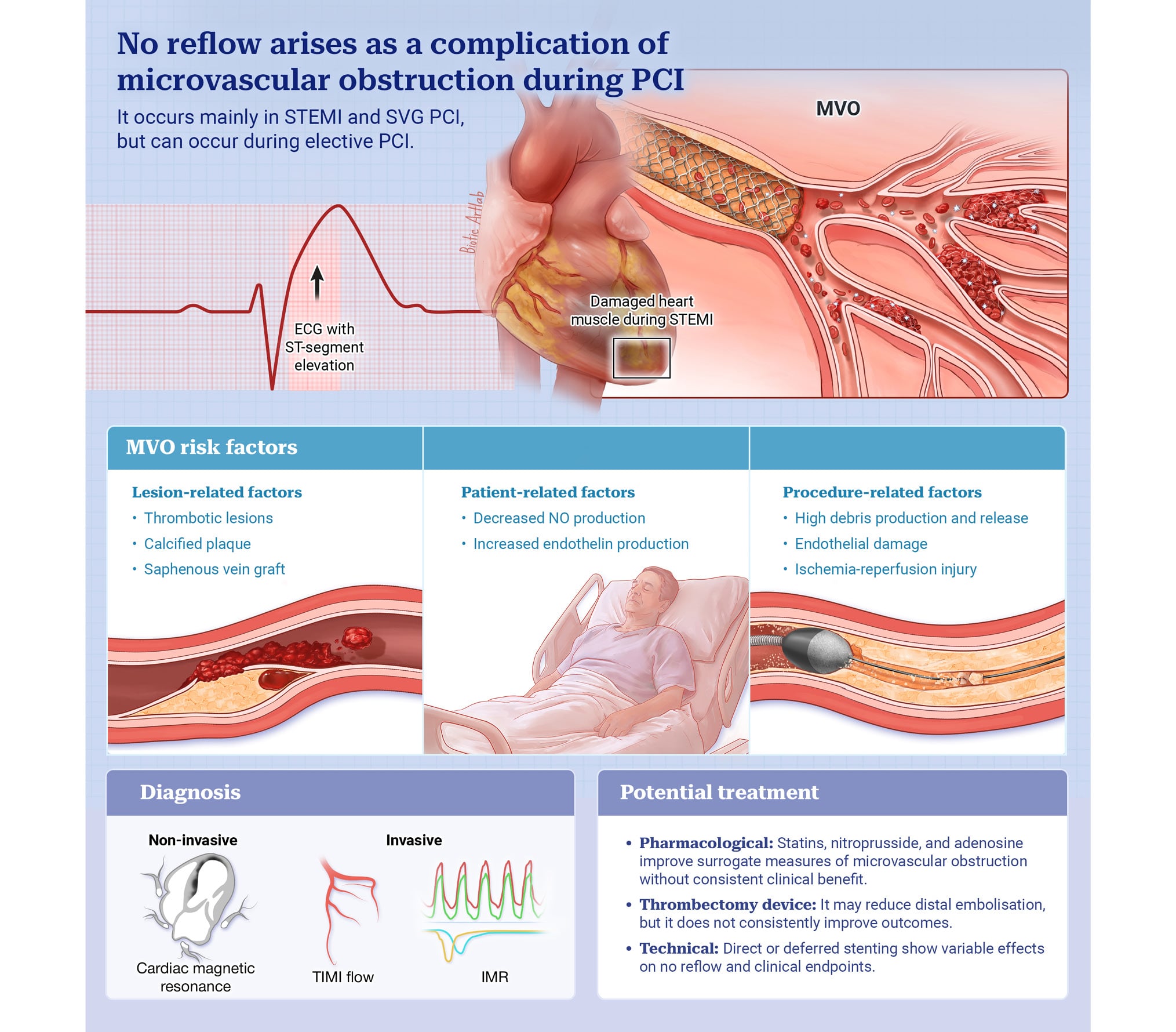
Central illustration. Risk factors, diagnosis and treatment of slow flow/no-reflow. The current understanding of microvascular obstruction allows clinicians to identify several risk factors related to specific patient, plaque, and procedural characteristics, primarily associated with endothelial damage with reduced NO production and increased endothelin release. In addition, several tools have been developed for diagnosing microvascular obstruction, including both non-invasive and invasive tools. Among non-invasive tools, cardiac magnetic resonance imaging is increasingly utilised, while invasive tools mostly rely on TIMI flow assessment and pressure wire-based indices of microcirculatory resistance. Finally, several strategies have been proposed to prevent and treat microvascular obstruction, extending broadly beyond the mechanical procedures. Additional treatments include pharmacological options, such as preprocedural statins or intravascular adenosine, and technical aspects, such as direct stenting or staged stenting after an initial balloon-based lesion expansion. NO: nitric oxide; TIMI: Thrombolysis in Myocardial Infarction
Pathophysiology of slow flow and no reflow
Mechanistically, both slow flow and no reflow arise when the coronary microcirculation becomes the rate-limiting step for myocardial perfusion, despite epicardial patency.678 Risk factors for slow flow and no reflow cluster into patient, lesion, and procedural domains, with these factors being more prominent and of longer duration in no reflow (Figure 1, Supplementary Table 1).
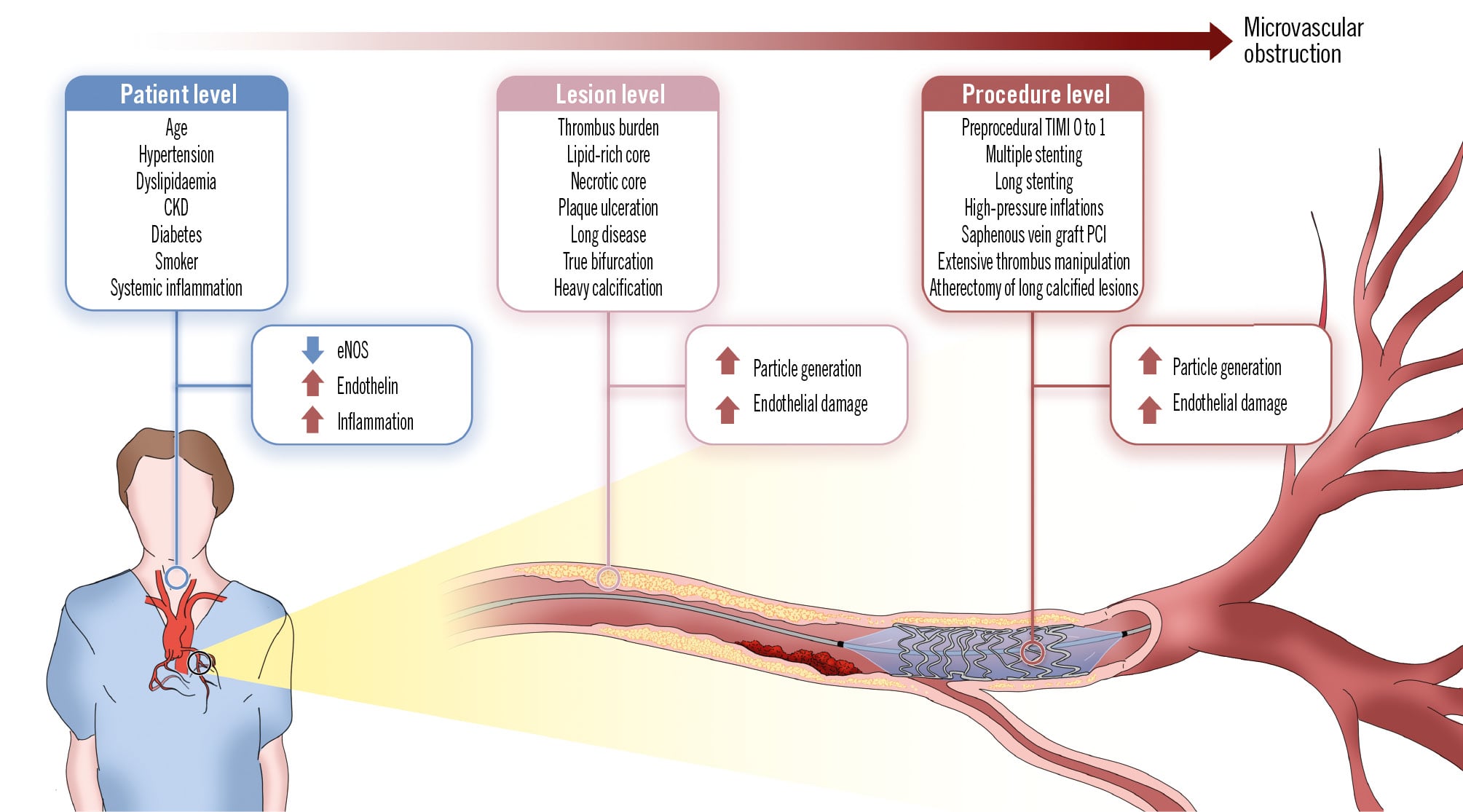
Figure 1. Risk factors for slow flow and no reflow. Several risk factors have been associated with slow flow and no reflow after PCI, which can be schematically clustered into patient-level, lesion-level, and procedure-level characteristics. Patient-level factors, such as age and CKD, reduce the activity of eNOS, while lesion- and procedure-level factors are those associated with increased particle generation, ultimately leading to slow flow and endothelial damage. All these factors play a key role in generating the imbalance between nitric oxide and endothelin in favour of endothelin, further inducing endothelial damage and peripheral capillary ischaemia. CKD: chronic kidney disease; eNOS: endothelial nitric oxide synthetase; PCI: percutaneous coronary intervention; TIMI: Thrombolysis in Myocardial Infarction
Mechanisms of no reflow
The mechanisms underlying no reflow are illustrated in Figure 2.
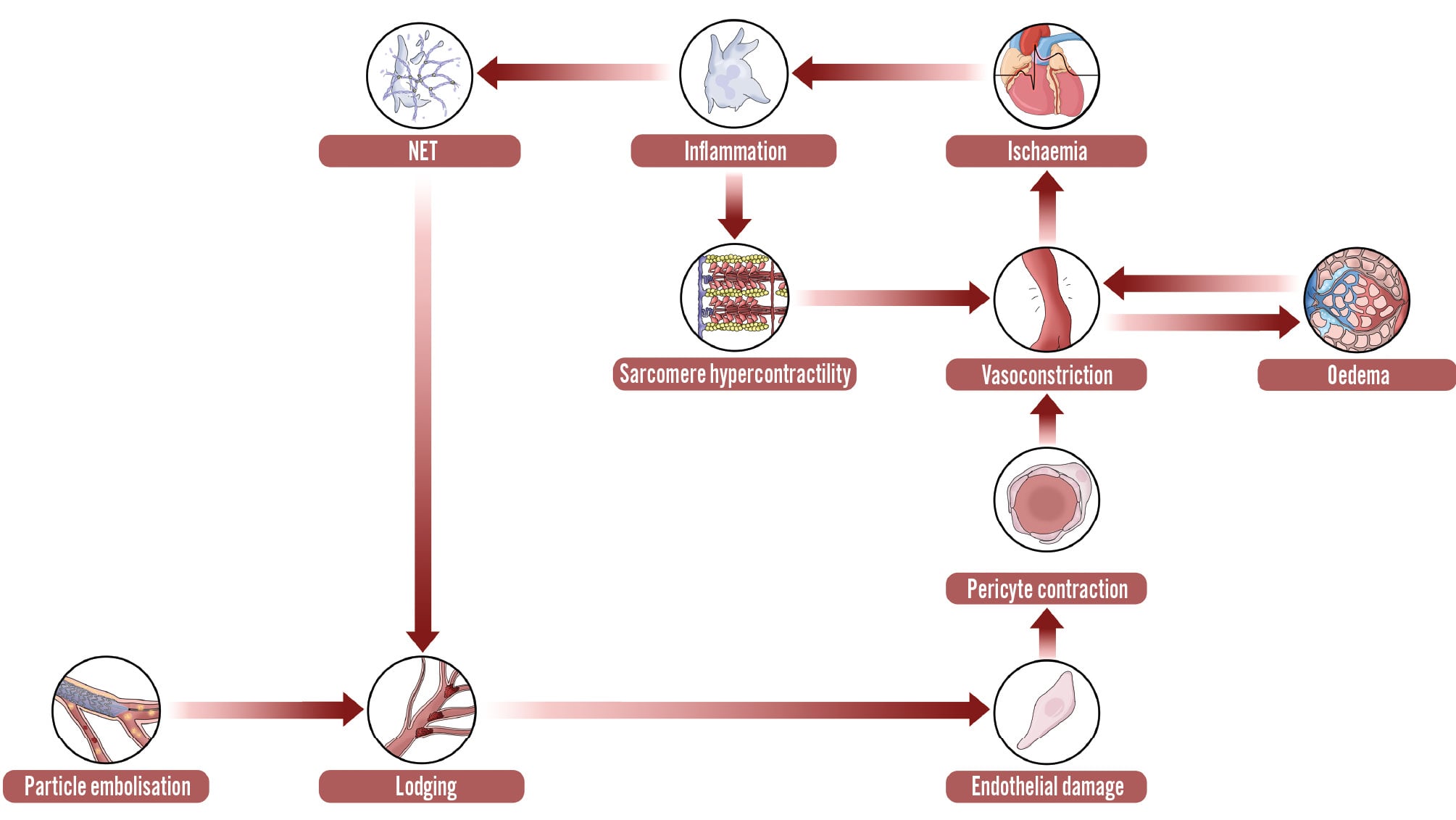
Figure 2. Pathophysiology of slow flow and no reflow. Endothelial damage and dysfunction play a central role in the complex pathophysiology of microvascular obstruction. Indeed, both the ongoing ischaemia and periprocedural particle embolisation lead to lodging of debris in the capillary bed, damaging the endothelium and leading to an imbalance between nitric oxide and endothelin production, and pericyte hyperreactivity, resulting in capillary vasoconstriction. Such vasoconstriction also leads to oedema and worsens ongoing ischaemia, worsening endothelial damage in a continuous ischaemic loop. In addition, ongoing ischaemia also induces local inflammation, which increases both peripheral lodging and vasoconstriction by NET production and sarcomere hypercontractility associated with calcium mobilisation, respectively. NET: neutrophil extracellular trap
Thrombus embolisation
A first mechanism is distal microembolisation secondary to wire, balloon, or stent manipulation, which dislodges platelet-fibrin aggregates, cholesterol crystals, and cellular debris that become lodged in arterioles and capillaries, creating patchy luminal loss and heterogeneous areas of non-perfused microvasculature.678 When the embolic particulate burden is modest, angiography may show delayed contrast transit, indicating slow flow. In contrast, when the embolic burden is high or recurrent, the obstruction becomes durable and tissue-level: the hallmark of no reflow and MVO.678
In parallel, the embolic burden damages the coronary endothelial surface layer. Glycocalyx shedding exposes intercellular adhesion molecule-1 (ICAM-1), vascular cell adhesion molecule-1 (VCAM-1), and von Willebrand factor, thereby enhancing leukocyte rolling and platelet tethering through leukocyte integrins. Moreover, endothelial nitric oxide synthase (eNOS) operates in a state that is deficient in cofactors or substrate, generating superoxide rather than nitric oxide (NO) and reducing NO bioavailability, while oxidation of soluble guanylate cyclase further reduces cyclic guanosine monophosphate (cGMP) output. Reactive oxygen species (ROS), hypoxia, thrombin, and cytokines upregulate endothelin-1 and endothelin-converting enzyme-1, while the loss of NO removes tonic suppression and augments endothelin-1 production and release. Overall, these changes promote coronary vasomotor constriction.6910 Because signalling from NO to soluble guanylate cyclase, and then to cGMP, is reduced as endothelin-1 levels rise, the coronary microcirculation cannot dilate fully during hyperaemia and its minimal resistance increases.610
Vasoconstriction
At the capillary wall, pericytes are active effectors of persistent narrowing. These contractile mural cells encircle capillaries and regulate their diameter; small calibre reductions disproportionately raise resistance. With endothelin-1 dominance, the activation of endothelin A and endothelin B receptors increases intracellular calcium and enhances calcium sensitivity via Rho kinase, sustaining pericyte and arteriolar constriction and raising minimal microvascular resistance.611 Ischaemia and early reperfusion trigger contraction at these sites, and relaxation is supported by the nitric oxide to cGMP to protein kinase G and the adenosine to cyclic adenosine monophosphate (AMP) pathways. Experimental inhibition of pericyte pathways, for example, G protein-coupled receptor 39 signalling, relaxes the capillary bed and reduces no reflow, linking transient slow flow with persistent tissue-level hypoperfusion when pericyte constriction persists.61112 Concomitantly, oedema accumulates within the reperfused territory, and extravascular compression raises interstitial hydrostatic pressure, further increasing microvascular resistance. Within the slow-flow and no-reflow continuum, this effect is load dependent, meaning that greater oedema volume produces larger increases in resistance.1314
Reperfusion injury
During ischaemia, succinate accumulates. Upon reperfusion, its rapid oxidation at the mitochondrial level drives a burst of ROS, while myocytes accumulate calcium.121516 Mitochondrial permeability transition pore opening follows, leading to myocardial sarcomere hypercontracture − defined as calcium-driven sarcomere shortening with myofibrillar rigor − and regulated cell death. This cascade worsens endothelial dysfunction, promotes sustained pericyte contraction, and releases damage-associated molecular patterns that promote microthrombus formation and capillary occlusion. Consequently, more extensive and sustained ischaemia-reperfusion signalling pushes the phenotype towards no reflow.121516
Ultimately, inflammation and thrombosis pathways consolidate, causing failure in both slow flow and no reflow. Platelet-leukocyte aggregates and neutrophil extracellular traps (NETs) scaffold microthrombi; integrin-mediated binding with exposure of phosphatidylserine and tissue factor, as well as modulation by sphingosine-1-phosphate and ceramide, injures the endothelium and interfaces with coagulation to stabilise capillary occlusion. Greater activation of these mechanisms aligns with the transition from slow-flow physiology to no-reflow tissue injury.61718
Role of proteomics, metabolomics, microRNAs, and neutrophil extracellular traps
Metabolomics identifies ischaemic succinate as a central node linking these entities. During ischaemia, mitochondria accumulate succinate; when reperfusion begins, rapid succinate oxidation triggers a burst of reactive oxygen species. Thus, higher succinate flux and downstream lipid peroxidation correlate with the larger, more durable microvascular obstruction typical of no reflow.19
Proteomic studies in acute myocardial infarction (MI) demonstrate enrichment of complement and coagulation proteins in patients with greater MVO. This aligns with human myocardial data showing complement upregulation and deposition of the C5b-9 membrane attack complex following infarction. These signals are present in slow flow, but they are more intense and involve a larger myocardial territory in no reflow.20
In parallel, microribonucleic acids (miRs) are small non-coding ribonucleic acids (RNAs) − about 22 nucleotides in length − that repress messenger RNA and modulate endothelial stability, inflammatory signalling, and thrombosis across the slow-flow to no-reflow spectrum.2122 Clinical cohorts link circulating miR-208a with angiographic no reflow and adverse remodelling, and associate miR-660-5p with the no-reflow phenotype in STEMI.232425 Consistent with these clinical findings, no reflow after primary PCI shows higher levels of the long non-coding RNA metastasis-associated lung adenocarcinoma transcript-1 and lower levels of miR-30e, miR-126, and miR-155, together with increased endothelin-1 and heparanase.232425 Complementary reports further link reduced levels of miR-126 and miR-155 following intervention to impaired endothelial integrity; meanwhile, miR-98, miR-145, and miR-34 are described as modulators of endothelial survival and tone in ischaemia-reperfusion models, aligning with the clinical gradation from slow flow to no reflow.19
Ultimately, NETs are deoxyribonucleic acid (DNA) and protein webs released by activated neutrophils. In primary PCI, NETs scaffold platelet and fibrin microthrombi, bind von Willebrand factor and tissue factor, and obstruct capillaries, driving the transition from slow flow to no reflow. While deoxyribonuclease (DNase) reduces NET-mediated no reflow in ischaemia-reperfusion models, a higher NET burden is associated with poorer ST-segment resolution and a larger MI size.172627
Role of pericytes
A clear conceptual distinction has been made between reperfusion injury, which primarily affects cardiomyocytes, and no reflow, which is predominantly a microvascular phenomenon.6 Several experimental studies have demonstrated that a reduction in infarct size does not necessarily translate into attenuation of the no-reflow area or improvement in myocardial blood flow, suggesting a dissociation between myocyte salvage and microvascular perfusion.6 Kaul et al proposed the hypothesis that when the mean coronary perfusion pressure falls below 45 mmHg and arterioles – fully dilated – cannot maintain a constant capillary hydrostatic pressure, pericyte contraction induces capillary constriction. This mechanism aims to stabilise capillary hydrostatic pressure at approximately 30 mmHg, as required by Starling’s laws governing tissue fluid homeostasis. This pericyte-mediated capillary constriction, demonstrated during myocardial ischaemia and low perfusion pressure states, results in a capillary volume decrease with reduced myocardial blood flow, particularly in the endocardium.628 This phenomenon, called ischaemic capillary derecruitment, has been described not only in the heart but also in skeletal muscle and the central nervous system.2829 Importantly, this mechanism, initially reversible, may become irreversible with prolonged ischaemia or ineffective reperfusion because of pericyte death or phenotype transformation, leading to permanent capillary rarefaction, sustained microvascular dysfunction, and eventually, myocardial necrosis and heart failure.6 Pericyte contraction may therefore represent a unifying and pathophysiologically plausible mechanism underlying the no-reflow phenomenon. This could open new opportunities for pharmacological or mechanical interventions aimed at preserving or restoring microvascular perfusion – beyond epicardial recanalisation – with pericyte relaxation and subsequent reductions in no reflow, infarct size and degree of ischaemia.
Non-invasive and invasive diagnostic tools
Microcirculatory vessels (<500 μm), whose obstruction is the cause of the slow-flow/no-reflow phenomenon, cannot be visualised by non-invasive or invasive imaging techniques. Therefore, diagnosing this condition requires the use of specific angiographic/electrocardiogram (ECG) indices and functional tests.30
ECG
ST-segment resolution in patients with STEMI is widely used as a marker of myocardial reperfusion in patients treated with thrombolysis or following primary PCI. An ST-segment resolution <50% has been associated with severe microcirculatory injury and worse outcomes compared with an ST-segment resolution ≥50%.3132
Coronary angiography
The angiographic definition of slow flow/no reflow has traditionally been based on visual estimation. The slow-flow/no-reflow phenomenon is defined as a delay in the progression of the contrast dye into the coronary arteries after successful culprit (epicardial) vessel revascularisation.3033
The Thrombolysis in Myocardial Infarction (TIMI) flow grade (from 0 to 3) is a visually estimated semiquantitative method to assess the severity of slow flow/no reflow after PCI.34 In patients with STEMI, normal TIMI flow (grade 3) has been associated with a low risk of in-hospital death.35 However, a notable percentage of patients with normal TIMI flow also show inadequate myocardial perfusion, leading to pathological cardiac remodelling, heart failure and cardiac death at follow-up.36 In fact, only 24% (day 1), 31% (day 2), 35% (day 4), and 43% (day 8) of STEMI patients treated with primary PCI and with normal angiographic TIMI flow post-PCI exhibit a normal perfusion on cardiac magnetic resonance imaging (MRI).37
The myocardial blush grade (MBG) is another visually estimated classification aimed at characterising myocardial reperfusion (from 0 to 3) in patients with normal TIMI flow.36 Assessment of the MBG requires generous contrast injection (to properly fill the entire coronary artery) and long cinefluoroscopic recordings up to the venous phase of the contrast passage. The MBG is based on the contrast filling and washout of the distal (prearteriolar) vessels of a selected artery. The best projection is usually chosen for each coronary artery, preferably the left lateral view for the left anterior descending artery (LAD) and the right oblique view for the left circumflex and right coronary arteries. Table 1 shows the TIMI coronary flow and MBG classifications. Although TIMI flow and the MBG are intuitive and easy markers of coronary flow and myocardial perfusion, they have significant variability and very low accuracy for assessing microcirculatory obstruction.38
The TIMI frame count and the corrected TIMI frame count (CTFC) are more useful to objectively evaluate the coronary flow and are frequently used in the setting of clinical trials. The TIMI frame count is defined as the number of cine frames needed for the contrast dye to reach standardised distal landmarks.39 For the TIMI frame count assessment, it is advisable to perform high-definition cinefluoroscopic recordings of the investigated vessel at 25 or 30 frames/second. The first frame is counted when the contrast dye fully enters the artery. For the LAD, the standardised distal landmark is the distal bifurcation (moustache), for the left circumflex artery, it is the distal bifurcation with the longest distance to the culprit lesion, and for the right coronary artery, it is the first branch of the posterolateral artery.39 The CTFC is based on the TIMI frame count, adjusted for the differences in the cine frame rate between laboratory systems and the different lengths of the coronary arteries. TIMI frame count estimation in catheterisation laboratories with cine acquisitions at 25 frames/second requires multiplying by a factor of 1.2 to homogenise with acquisitions at 30 frames/second; and TIMI frame count of the LAD requires dividing by a factor of 1.7 to homogenise with the other arteries.39 Although several studies indicate a relationship between (high) CTFC and adverse clinical outcomes, the correlation between CTFC and microvascular obstruction is weak.40
Table 1. Angiographic grades of coronary reperfusion.
| Grade | TIMI flow | Myocardial blush grade |
|---|---|---|
| 0 | No reflow: there is no antegrade flow beyond the revascularised lesion | No myocardial blush or contrast density; or in extreme cases, myocardial blush persists and stains the myocardium, indicating leakage of contrast medium into the extravascular space |
| 1 | Slow flow: the contrast material passes beyond the revascularised lesion but does not fill the entire distal coronary artery (for the entire cinefluoroscopy sequence) | Minimal myocardial blush or contrast density |
| 2 | Slow flow: the contrast material passes beyond the revascularised lesion and opacifies the entire distal coronary artery but slower than other arteries not supplied by the target lesion | Moderate myocardial blush or contrast density, but less than that seen during angiography of a contralateral or ipsilateral non-infarct-related artery |
| 3 | Normal flow: antegrade flow fills the distal bed of the revascularised vessel at a similar velocity as other coronary vessels | Normal myocardial blush or contrast density, comparable with that seen during angiography of a contralateral or ipsilateral non-infarct-related artery |
| TIMI: Thrombolysis in Myocardial Infarction | ||
Cardiac magnetic resonance imaging
Cardiac MRI is the gold-standard technique to assess MVO, equivalent to the slow-flow/no-reflow phenomenon, in STEMI patients.4 In a pooled data analysis of 1,688 STEMI patients imaged with cardiac MRI within 7 days of the index procedure, MVO was observed in 57% and was associated with a significantly higher risk of death or rehospitalisation for heart failure at 1 year.4
MVO assessment by cardiac MRI requires specific perfusion protocols with intravenous (IV) gadolinium. MVO is generally measured on early (1-3 minutes) and late (8-10 minutes) gadolinium administration sequences. In both sequences, MVO is typically visualised as central dark focus areas within the hyperenhanced infarcted area.41 Due to the slow diffusion of gadolinium into the surrounding areas of the no-reflow site, early sequences identify a higher proportion of patients and larger areas of MVO than late sequences. It is commonly accepted that late sequences reflect a more reliable segmentation of the no-reflow segment.41
The main limitations of cardiac MRI are the low accessibility in many institutions and the variability of MVO over time. The amount of MVO increases threefold during the first 48 hours after STEMI, and then it gradually decreases between the first and second month until it disappears.
Functional angiography-derived indices of microvascular resistance
Novel angiographic-based software assisted with automatic lumen contour detection, along with surrogate TIMI frame count and myocardial blush grading, is being investigated to assess the microcirculatory resistance.42 So far, it has shown poor accuracy to assess the microcirculatory resistance compared with intracoronary (IC) pressure wire-based assessment.42 However, this is an emergent field with potential improvement using artificial intelligence to redefine current algorithms.
There is limited evidence supporting the use of these software platforms in STEMI patients. However, most of the studies conclude that angiography-derived indices have better accuracy to diagnose MVO (defined by cardiac MRI) than TIMI flow or MBG based on plain angiography and visual assessment.4344
Functional invasive methods based on intracoronary wires
Invasive functional assessment with Doppler and pressure-thermistor intracoronary wires allows an immediate diagnosis of slow flow/no reflow and monitoring of the response to dedicated therapies. All invasive functional methods require maximal (achievable) hyperaemia. The coronary flow reserve (CFR) is the ratio between the estimated coronary flow at rest and at maximal hyperaemia. Although a CFR <2 is considered a parameter of microcirculatory dysfunction and has been associated with poor clinical outcomes, it represents the capacity of the whole coronary system (including the epicardial vessel and the microcirculation) to increase the coronary flow. For this reason, other invasive indices focused solely on the microcirculation are preferred in this context. So far, three different techniques have been described.
Doppler wire
Intracoronary Doppler wires assess the coronary blood velocity (cm/sec). Together with the lumen area (cm2) measured at the location of the Doppler sensor (by angiography or intravascular imaging techniques) and the distal pressure at maximal hyperaemia, they are capable of estimating the coronary blood flow (cm3/sec) and the hyperaemic microcirculatory resistance velocity. Most notably, IC Doppler assessment has described unique characteristics of the slow-flow/no-reflow phenomenon, such as early systolic retrograde flow and rapid deceleration of diastolic blood velocity.45 Currently, IC Doppler wires are not available worldwide.
Thermodilution with bolus saline injection
Intracoronary bolus saline injection requires a dedicated pressure-thermistor wire (PressureWire X [Abbott]), software (CoroFlow [Coroventis]) and any hyperaemic agent. Three consecutive 3 mL bolus saline injections at rest and at maximal hyperaemia are needed to assess the resting and hyperaemic mean transit times (Tmn).46 Tmn is an equivalent of the coronary flow, and therefore, CFR is estimated as the ratio between resting Tmn and hyperaemic Tmn values.46 The index of microcirculatory resistance (IMR) is assessed simultaneously with the CFR and represents the minimal resistance to coronary flow at maximal hyperaemia. The IMR is an abstract value obtained by the formula: Tmn x distal pressure at maximal hyperaemia. In patients without acute coronary syndrome, an IMR ≥25 is considered coronary microvascular dysfunction.46 In STEMI patients with an IMR assessment of the culprit vessel after revascularisation, around 50% of patients have an IMR >25.47 However, only an IMR >40 has been associated with MVO, as assessed by cardiac MRI, and with poor clinical outcomes.474849
Thermodilution with continuous saline infusion
Intracoronary continuous saline infusion requires the same pressure-thermistor wire (PressureWire X) and software (CoroFlow) as bolus saline infusion, together with a dedicated microcatheter (RayFlow [HEXACATH]) and infusion pump. Maximal hyperaemia is obtained by IC saline infusion at 15-30 mL/min via a microcatheter without the need for any hyperaemic agent. In patients without acute coronary syndrome, continuous saline infusion causes steady hyperaemia to a similar or superior degree as IC or IV adenosine. Continuous saline infusion thermodilution technique provides the absolute coronary flow (ACF) and minimal microcirculatory resistance (MMR) of a selected segment of any artery. This technique is operator independent and has shown excellent reproducibility.50 However, human variability in coronary artery tree distribution and differences in the ventricular mass between arteries hamper the standardisation of ACF and MMR reference values.
In STEMI patients, MMR measurement after primary PCI has good diagnostic accuracy to predict an IMR >40.51 However, in patients with severe slow flow/no reflow after primary PCI, continuous saline infusion causes a continuous cooling of the distal temperature and may confer erratic measures.52
Prevention and treatment of no reflow
Various pharmacological agents, mechanical devices, and technical strategies have been tested for preventing and treating no reflow in STEMI. They target the pathophysiological factors involved in the occurrence of no reflow, including thrombus embolisation, vasoconstriction, and reperfusion injury.
Pharmacological strategies
Adenosine
Adenosine is a purine nucleoside that binds adenosine receptors in cardiac myocytes and blood vessels. The main effects include smooth muscle cell relaxation in the coronary circulation, negative dromotropic and chronotropic effects, and antiplatelet properties. In initial studies in patients with STEMI receiving thrombolytic therapy (Acute Myocardial Infarction STudy of ADenosine [AMISTAD] I and II trials), adenosine showed a reduction in infarct size, although it did not improve clinical events.5354
The Intracoronary Nitroprusside Versus Adenosine in Acute Myocardial Infarction (REOPEN-AMI) multicentre trial evaluated the effects of intracoronary adenosine or nitroprusside on MVO in patients undergoing primary or rescue PCI after thrombus aspiration and glycoprotein (GP) IIb/IIIa antagonist administration. Selective infusion of adenosine, but not that of nitroprusside, was demonstrated to improve MVO, as assessed by an ST-segment resolution >70% at 90 minutes after primary PCI.55 The REperfusion Facilitated by LOcal Adjunctive Therapy in ST-elevation Myocardial Infarction (REFLO-STEMI) trial tested whether intracoronary high-dose adenosine or sodium nitroprusside reduced infarct size and/or MVO, determined by cardiac MRI. MVO was similar across groups. However, on per-protocol analysis, infarct size and major adverse cardiac events at 30 days and 6 months were increased and ejection fraction was reduced in adenosine-treated patients compared with controls.56
Nitroprusside
Nitroprusside is a direct donor of nitric oxide, which is a potent vasodilator of the resistance arteriolar circulation and has antiplatelet and anti-inflammatory effects. Intracoronary nitroprusside at doses of 50-300 μg is effective in the treatment of no reflow. When injected distally in the coronary artery, it has a negligible systemic effect on blood pressure. As seen above, it has been used as a comparator against adenosine with inconclusive results.5557 Recently, the Treatment of Slow-flow After Primary Percutaneous Coronary Intervention With Flow-mediated Hyperemia (RAIN FLOW) study, randomised patients with ST-segment elevation myocardial infarction and no reflow to receive either pharmacological-mediated hyperaemia with IC adenosine or nitroprusside, or a combination of both (n=30), versus flow-mediated hyperaemia (n=37). Both the TIMI frame count and MMR were similar between groups.52
Calcium channel blockers: nicorandil, verapamil, and diltiazem
Nicorandil is a potassiumâchannel activator with nitrate properties that improves microvascular flow by dilating coronary microvessels resistant to standard nitrates and reduces neutrophil infiltration and platelet aggregation. This drug has been demonstrated to reduce the occurrence of no reflow after rotational atherectomy and during PCI of vein grafts.5258 In the Effects of Nicorandil on Cardiac Infarct Size in Patients With ST-segment-Elevation Acute Myocardial Infarction Undergoing Primary Percutaneous Coronary Intervention (CHANGE) trial, IV nicorandil was demonstrated to reduce the incidence of no reflow and the infarct size while improving the rate of complete ST-segment resolution and left ventricular (LV) ejection fraction.59 A recent randomised trial reported that the oral administration of nicorandil significantly reduced the rate of no reflow, improved the myocardial blush grade, showed higher rates of complete ST-segment resolution, and improved clinical outcomes compared to placebo.60 In a meta-analysis involving 18 randomised controlled trials (RCTs), nicorandil significantly reduced the incidence of the no-reflow phenomenon and major adverse cardiac events, with a combination of IC and IV administration representing the optimal usage of nicorandil.61
Verapamil and diltiazem were compared against nitroglycerine in patients with no reflow after primary PCI in the REstoration of COronary flow in patients with no-reflow after primary coronary interVEntion of acute myocaRdial infarction (RECOVER) trial. Compared with the nitroglycerine group, the diltiazem and verapamil groups showed improvements in corrected TIMI frame counts, had more complete ST-segment resolution at 3 hours after PCI, and demonstrated lower peak troponin T levels, and lower N-terminal pro-B-type natriuretic peptide levels at 1 and 30 days after PCI.62
Statins
Beyond cholesterol reduction, statins exhibit anti-inflammatory, antithrombotic, and endothelial-protective properties that may be particularly beneficial in the acute setting of STEMI. A systematic review and meta-analysis involving 11 studies (n=4,294 patients) demonstrated that the use of high-dose statins before PCI significantly reduced postprocedural no reflow.63
Glycoprotein IIb/IIIa inhibitor
According to the 2023 European Society of Cardiology (ESC) guidelines for the management of acute coronary syndromes, GP IIb/IIIa inhibitors should be considered (Class IIa, Level of Evidence C) if there is evidence of no reflow or a thrombotic complication during PCI.64 In the INFUSE-AMI trial, patients presenting with anterior STEMI were randomised in a 2x2 factorial design to receive abciximab or not, and manual thrombectomy or not. The primary endpoint (infarct size at 30 days as assessed by MRI) was reduced in the abciximab group (vs placebo) but not in the manual aspiration therapy group. However, indices of myocardial reperfusion, ST-segment resolution, and 30-day clinical event rates were not significantly different between the randomised groups.65 Recently, the randomised REVERSE-FLOW trial investigated the effect of GP IIb/IIIa inhibitors on cardiac MRI-derived reperfusion success in patients with angiographic MVO after primary PCI. The primary endpoint of infarct size was similar between patients assigned to GP IIb/IIIa inhibitors and controls. However, an exploratory analysis of patients with TIMI flow grade 0 or 1 revealed a significantly reduced infarct size after administration of GP IIb/IIIa inhibitors, while patients with TIMI flow grade 2 did not benefit. The risk of developing and the extent of cardiac MRI-derived MVO was significantly lower in patients who received GP IIb/IIIa inhibitors. Finally, bleeding events were significantly higher in the GP IIb/IIIa arm.66
Epinephrine
An observational proof-of-concept study randomised STEMI patients with refractory coronary no reflow during PCI to IC epinephrine versus conventional treatment. IC epinephrine improved TIMI 3 flow, left ventricular ejection fraction, and ST-segment resolution, and reduced 30-day death or heart failure compared with conventional agents.67 An open-label randomised clinical trial included 201 patients with no reflow who were randomised 1:1 to IC epinephrine and IC adenosine. The primary endpoints were improvement in coronary flow, as assessed by TIMI flow, corrected TIMI frame counts, and myocardial blush grade. No reflow was more effectively improved with epinephrine, as evidenced by improved final TIMI 3 flow and final corrected TIMI frame counts. However, no significant differences were observed in the rates of final grade 3 myocardial blush or in the mean reduction of corrected TIMI frame counts.68
Beta blockers
The use of beta blockers before reperfusion to reduce infarct size has been tested with conflicting results. The Effect of METOprolol in CARDioproteCtioN During an Acute Myocardial Infarction (METOCARD-CNIC) Trial (n=220) showed that IV metoprolol administered before primary PCI reduced infarct size and preserved LV function. This study only included anterior STEMI and was neither blinded nor placebo controlled.69 The Early Beta blocker Administration before reperfusion in patients with ST-Elevation Myocardial Infarction who are planned to undergo primary PCI (EARLY-BAMI) trial was the first double-blinded, placebo-controlled, multicentre international study assessing the effect of early IV beta blocker therapy before primary PCI in a less restricted STEMI population. The primary endpoint − mean infarct size − was similar between the metoprolol group and the placebo group. Prereperfusion administration of IV metoprolol did not improve left ventricular ejection fraction on cardiac MRI.70
Glucagon-like peptide-1 receptor agonist
Glucagon-like peptide-1 receptor agonist (GLP-1 RA) is an incretin hormone that regulates plasma glucose, has antioxidant and anti-inflammatory properties, and may protect endothelial function. Experimental studies have also revealed that GLP-1 RAs, or their analogues, protect against reperfusion injury in pigs. In a randomised trial that compared liraglutide versus placebo in STEMI patients before primary PCI, the prevalence of no reflow (primary endpoint) was significantly lower in the liraglutide group than in the control group. In addition, there was a significant decrease in serum high-sensitivity C-reactive protein levels at 6 hours post-reperfusion in the liraglutide group compared with the control group.71
The SALINE technique
The SALINE technique consists of 3 rapid (≈3 s) sequential intracoronary injections of 10 mL saline delivered through a thrombus aspiration catheter positioned distally to the stented segment in patients with no reflow after primary PCI. In a propensity score-matched analysis, this technique was shown to be safe and effective in improving surrogate markers of MVO, such as TIMI flow grade 3 and ST-segment resolution >70% at 90 minutes, compared with optimal standard therapy.72 At three years, major adverse cardiac events – though limited by the very small sample size – were reduced in the saline versus standard-of-care group. Each saline bolus aims to rapidly increase distal coronary pressure and volume, promoting microvascular recruitment and displacement of microemboli and vasoconstrictive agents.73 This hypothesis on its mechanism of action is supported by a reduction of the postprocedural IMR in most cases. These findings should be considered as hypothesis-generating and require confirmation in larger and randomised trials.
Mechanical strategies
The mechanical strategies for preventing and treating no reflow in STEMI are depicted in Figure 3.
The single-centre Thrombus Aspiration during Percutaneous coronary intervention in Acute myocardial infarction Study (TAPAS) was the first randomised trial analysing the effect of manual thrombectomy on myocardial blush grade: it showed that aspiration thrombectomy reduced the incidence of no reflow, improved angiographic outcomes, and even improved cardiac death at 1 year.7475 Nevertheless, the large-scale Thrombus Aspiration in ST-Elevation Myocardial Infarction in Scandinavia (TASTE) trial and A Randomized Trial of Routine Aspiration ThrOmbecTomy With PCI Versus PCI Alone in Patients With STEMI Undergoing Primary PCI (TOTAL) demonstrated that routine thrombus aspiration did not reduce mortality among patients with STEMI up to 1 year, but it was associated with an increase in the rate of stroke.767778 Therefore, routine aspiration thrombectomy has gained a Class III, Level of Evidence A, recommendation in the setting of primary PCI in the recent ESC guidelines.64 Selective use in patients with significant thrombus burden may be considered.
Rheolytic thrombectomy also failed to improve infarct size, TIMI myocardial blush grade, microvascular obstruction, and LV remodelling.7980 Few data are available about mechanical thrombectomy, though findings are especially positive regarding continuous mechanical aspiration thrombectomy, which has an established role in thrombus removal within the neurovasculature and pulmonary bed.81 Distal protection (with filters or balloons) has also not shown any benefit in preventing no reflow in STEMI,828384 whereas it has shown to be beneficial in preventing no reflow in elective saphenous vein graft PCI.85
Other device-based strategies aimed at reducing the incidence of no reflow in acute STEMI treatment are the use of mesh-covered stents and lasers. The MGuard (InspireMD) − a bare metal stent covered with a polymeric mesh − was designed to reduce distal embolisation during percutaneous coronary intervention in STEMI. The MASTER trial showed complete ST-segment resolution with the MGuard stent compared with control, with a trend towards reduced 1-year mortality, despite late lumen loss typical of bare metal stents. However, the improved safety and efficacy of drug-eluting stents, together with stent dislodgment issues related to the MGuard stent, have led to its discontinuation.86
Excimer laser coronary angioplasty has been proposed to reduce distal embolisation and no reflow by plaque debulking and thrombus vaporisation before stent implantation.87 However, there are no randomised studies supporting this hypothesis.
Another device-based therapy aimed at limiting infarct size, which is the result of no reflow and subsequent MVO, is the Pressure-controlled intermittent coronary sinus occlusion device (PiCSO [Miracor Medical]). It consists of a dedicated balloon placed in the coronary sinus that inflates and deflates cyclically providing a transient increase in coronary sinus pressure that redistributes blood flow from the remote to the ischaemic myocardium. Preliminary non-randomised studies showed that this therapy was safe and feasible, and was potentially associated with improved coronary microvascular resistance. The PiCSO-AMI-I trial was the first randomised study evaluating the ability of PiCSO to reduce infarct size in STEMI patients undergoing primary PCI. It included 145 patients randomised 1:1 to PiCSO-assisted PCI versus conventional PCI. The trial failed to show any difference in infarct size between the 2 groups either at 5 days or at 6 months, with no difference in terms of MVO occurrence. PiCSO use was associated with increased procedural time and contrast use but not with an increase in adverse events up to 6 months.88
Among novel technologies, supersaturated oxygen (SSO2) infusion represents another potential treatment of no reflow and MVO. Preclinical studies showed that SSO2 may reduce infarct size by decreasing microvascular damage. The Acute Myocardial Infarction with Hyperoxemic Therapy (AMIHOT) study tested SSO2 in 269 STEMI patients in a randomised manner: infarct size did not differ between the 2 groups, but there was some evidence towards a positive effect in anterior STEMI.89 This was confirmed in AMIHOT II, which included only anterior STEMI, with a statistically significant reduction in infarct size in the SSO2 group.90 SSO2 therapy has received U.S. Food and Drug Administration (FDA) approval and a European Conformity (CE) mark and is indicated for non-shock anterior (LAD) STEMI treated successfully with PCI within 6 hours of symptom onset. SSO2 is usually infused through a 5 Fr guiding catheter for 60 minutes following stent implantation in anterior STEMI.91
Finally, hypothermia was studied in the EUROpean Intracoronary Cooling Evaluation in Patients With ST-elevation Myocardial Infarction (EURO-ICE) trial, in which 200 patients with anterior STEMI were randomised 1:1 to selective IC hypothermia (30-33°C for 7-10 minutes before and 10 minutes after reperfusion) or primary PCI alone. The study showed a favourable safety profile for the technique but failed to reduce microvascular injury or infarct size – evaluated by cardiac MRI – at 3-month follow-up.92
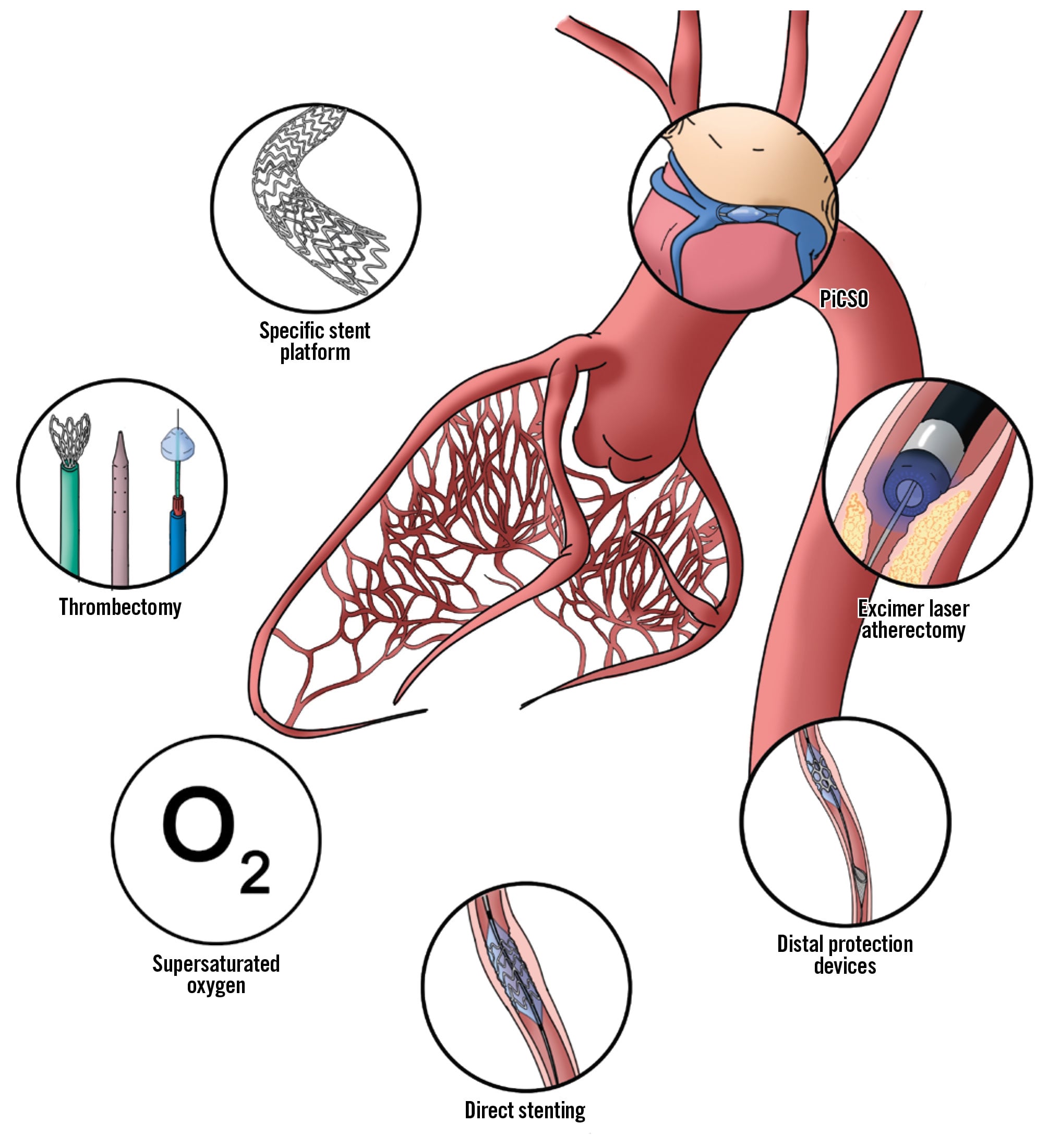
Figure 3. Interventional treatments for microvascular obstruction. Among the available treatments for microvascular obstruction, 6 interventional treatments have been tested in pivotal trials, including the use of specific stent platforms, such as balloon-expandable bare-metal stents with polyethylene terephthalate micronet mesh and self-expanding stents, mechanical thrombectomy, intracoronary supersaturated oxygen, PiCSO, excimer laser atherectomy, use of direct stenting to avoid particle generation during lesion preparation, and use of distal protection devices in cases of high-risk plaques. PiCSO: pressure-controlled intermittent coronary sinus occlusion
Technical strategies
Besides device-related strategies, there are also some technical strategies aimed at reducing the incidence of no reflow, such as direct stenting or deferred stenting. The idea of direct stenting (rather than predilation followed by stent implantation) in preventing no reflow is related to minimising thrombotic lesion preparation, avoiding thrombus embolisation. In elective cases, direct stenting has shown no benefit,93 whereas in primary PCI, evidence from small studies exists showing a reduced incidence of no reflow.8794 Evidence from a systematic review and meta-analysis – including only 3 small randomised clinical trials – suggests that direct stenting in STEMI might be associated with improved clinical and procedural outcomes; however, the fact that RCTs account for the minority of available data and that most of the available studies poorly reflect current clinical practice, as well as the existence of publication bias, preclude drawing definitive conclusions.95 Of interest, a subanalysis from the TOTAL Trial showed that although thrombectomy alone did not reduce no reflow in all patients, it may be synergistic with direct stenting.96
A two-step strategy of initial reperfusion by balloon angioplasty, followed by later stent implantation, has been also evaluated for the prevention of no reflow. The third DANish Study of Optimal Acute Treatment of Patients with ST-elevation Myocardial Infarction − Deferred Stent Implantation Versus Conventional Treatment (DANAMI-3-DEFER) showed that deferred stenting did not reduce infarct size, MVO, or the 10-year occurrence of all-cause mortality, but it did reduce hospitalisation for heart failure.9798 A meta-analysis of 8 studies (3 randomised and 5 non-randomised) also showed no differences in hard clinical endpoints, but it did show improved surrogate angiographic endpoints in deferred stenting versus the conventional approach.99
Another technical strategy explored in this field is ischaemic post-conditioning. This technique consists of reopening the infarct artery, followed by repetitive, brief interruptions of blood flow prior to establishment of final reperfusion through balloon inflation. Whereas in animal models, post-conditioning has resulted in an increase in myocardial salvage, in humans, there are conflicting results.100 The third DANish Study of Optimal Acute Treatment of Patients with ST-elevation Myocardial Infarction – Ischemic postconditioning (DANAMI-3-iPOST) tested the effect of post-conditioning in addition to primary PCI on survival and hospitalisation for heart failure. A total of 1,234 patients were randomised 1:1 to post-conditioning versus conventional treatment. No differences were found between groups in terms of TIMI flow after PCI nor in the other specified endpoints.101 However, a post hoc analysis of the same trial showed that post-conditioning reduced the risk of all-cause mortality and hospitalisation for heart failure in those patients not treated with thrombectomy up to 5-year follow-up, with no difference in the immediate post-PCI TIMI flow.102
Gaps in the evidence
Although the considerable data on the pathophysiology, diagnostic tools, and therapeutic procedures of the slow-flow/no-reflow phenomenon do not delineate a clear flowchart for its prevention and treatment, we have tried to suggest a flowchart based on standard clinical practice (Figure 4, Figure 5).
Looking ahead, a precision-medicine approach for treatment of no reflow/slow flow is essential. Standardising diagnostic methods, tailoring therapies to the underlying mechanisms of MVO, and stratifying patients based on risk profiles and individual susceptibilities are critical steps to optimise outcomes.
Various pharmacological and interventional strategies have been investigated to mitigate MVO in STEMI patients undergoing primary PCI. While several promising findings have emerged, these have not been translated into improved clinical outcomes in large RCTs. This discrepancy may be attributed to the multifactorial nature of MVO pathophysiology, variability in therapeutic responses influenced by drug dosages and the effects of background antithrombotic therapies, and the fact that the studies are quite old with the included patients often receiving thrombolytics or experiencing a delay to primary PCI.
Lack of standardisation in diagnostic methods has further contributed to inconsistencies in the reported incidence of MVO. While angiographic indices are widely used because of their accessibility, they offer limited sensitivity, especially given the dynamic nature of MVO, which can evolve hours or days after reperfusion. Advanced diagnostic tools, such as MRI, provide greater sensitivity and valuable prognostic information yet remain underutilised both in clinical practice and RCTs – due to limited availability and high costs.
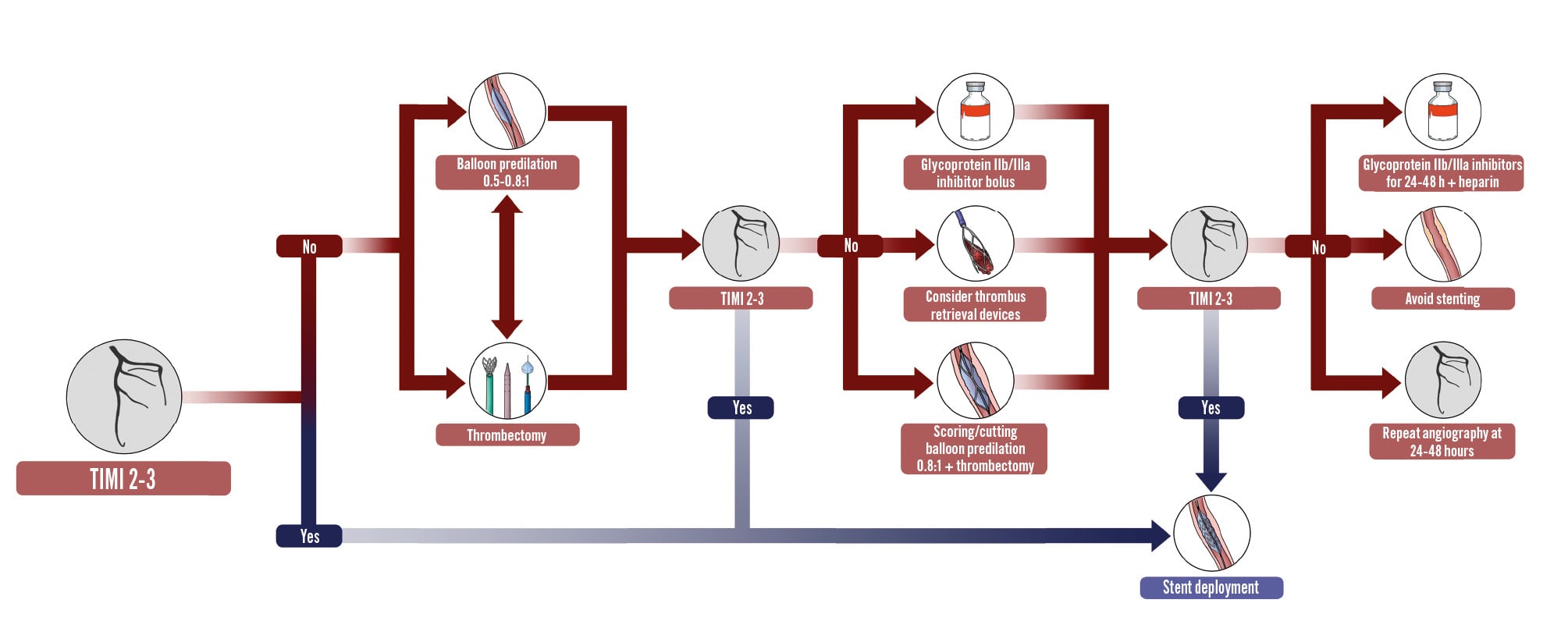
Figure 4. Algorithm for the prevention of slow flow/no reflow in patients undergoing percutaneous coronary intervention. The figure illustrates the algorithm for the prevention of slow flow and no reflow in patients undergoing percutaneous coronary intervention. If a TIMI flow of 0-1 is detected, several strategies may be attempted to restore flow before stent deployment, such as balloon predilation and thrombectomy. In case these strategies do not suffice, periprocedural glycoprotein IIb/IIIa inhibitors may allow dissolution of peripheral plugs and restore optimal flow. In case TIMI flow 2-3 is not achieved with these strategies, it may be appropriate to consider deferring stent implantation, with perfusion of glycoprotein IIb-IIIa inhibitors and heparin for 24-48 h. In case of significant thrombus burden, thrombus aspiration is also an option. TIMI: Thrombolysis in Myocardial Infarction
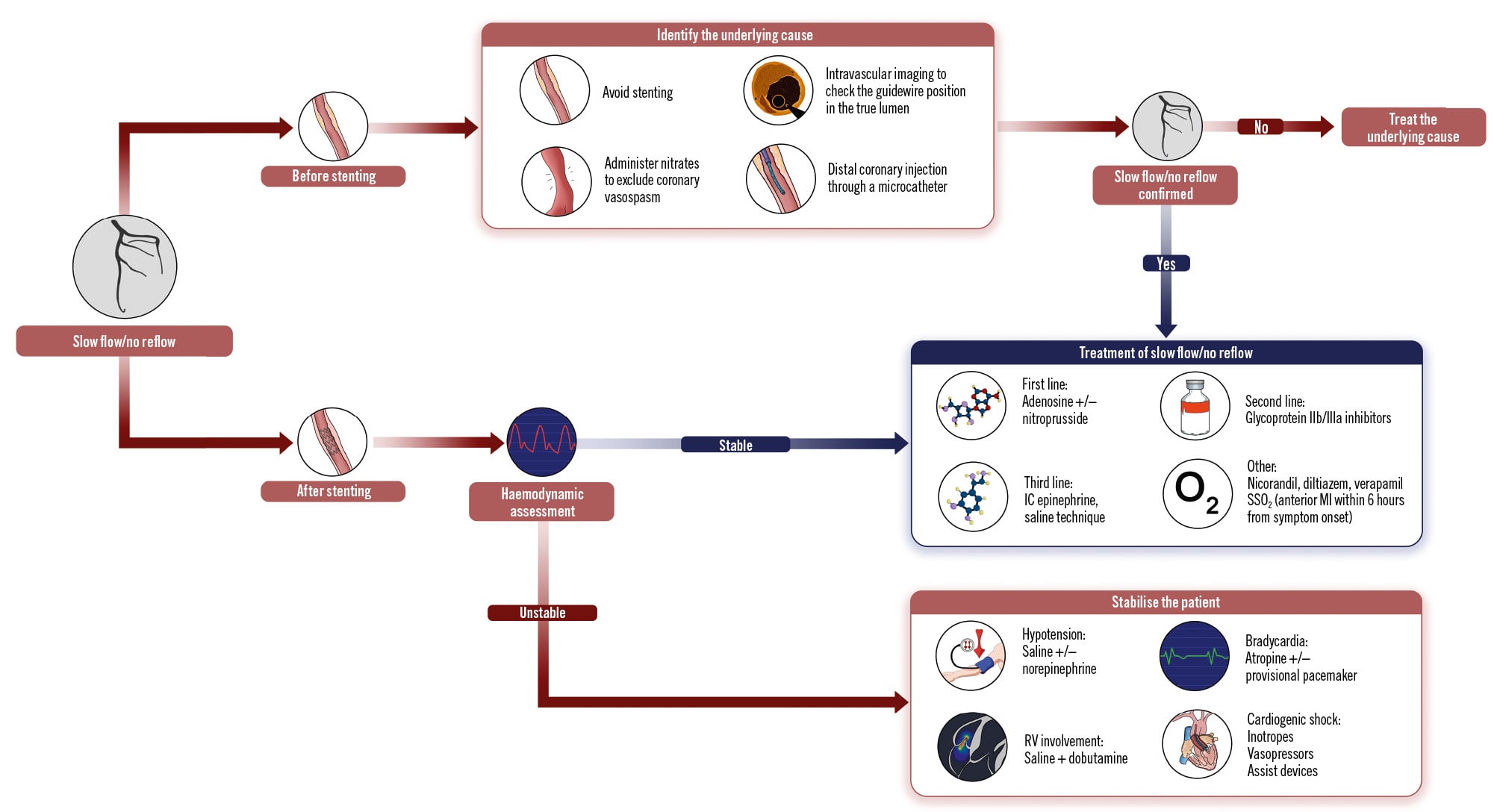
Figure 5. Algorithm for the treatment of slow flow/no-reflow in patients undergoing percutaneous coronary intervention. The figure illustrates the algorithm for the treatment of slow flow/no reflow in patients undergoing percutaneous coronary intervention. In case the slow flow/no reflow is detected before coronary stenting, identifying the underlying cause through intravascular imaging, distal injection, or nitrates is the cornerstone of downstream management. Similarly, if the diagnosis is made after stent deployment, it is critical to determine if the cause is true slow flow/no reflow or is due to haemodynamic instability. In the latter case, it is essential to stabilise the patient, as this could be misdiagnosed as slow flow/no reflow and lead to unnecessary downstream treatment, potentially worsening the patient’s clinical state and outcomes. IC: intracoronary; MI: myocardial infarction; RV: right ventricle; SSO2: supersaturated oxygen; TIMI: Thrombolysis in Myocardial Infarction
Conclusions
Intracoronary therapies and emerging approaches, such as SSO2, have shown encouraging results in specific patient subgroups and in improving surrogate outcomes. However, these findings require validation through large-scale, methodologically robust trials that address current evidence gaps. A new generation of clinical trials is focused on reperfusion therapy by testing adjunctive device-based and pharmacological strategies aimed at further reducing infarct size and MVO beyond the benefit achieved with primary PCI alone (Table 2). Future RCTs should explore new therapeutic targets, such as pericyte contraction, and should also prioritise comprehensive evaluations of therapeutic efficacy, encompassing not only surrogate endpoints but also hard clinical outcomes, to build stronger evidence.
Table 2. Future trials.
| Study name | Device/drug tested | Study description | Identifier number |
|---|---|---|---|
| STEMI-DTU | Impella CP systema | LV unloading with the Impella CP system in patients with anterior STEMI prior to reperfusion vs current standard of care aiming to reduce infarct size on cardiac MRI | NCT03947619 |
| RIC-AFRICA | RIC | Upper arm RIC in STEMI patients before and after reperfusion (mainly with thrombolysis). Primary composite endpoint: all-cause death and HF at 30 days | NCT04813159 |
| RIP-HIGH | RIC+post-conditioning | Brief cycle of RIC and post-conditioning after reperfusion vs standard of care in STEMI patients with Killip class ≥2 to evaluate the impact on all-cause mortality and HF | NCT04844931 |
| HOT-AAMI | IC SSO2 | SSO2 therapy administered immediately after pPCI in anterior STEMI vs pPCI alone in order to reduce the composite outcome of all-cause mortality or HF | NCT06742684 |
| REDUCE | Sono-thrombolysis | Sono-thrombolysis vs placebo delivered before and after pPCI, aiming to reduce infarct size on cardiac MRI | ACTRN12620000807954 |
| UPFRONT-STEMI | GP IIb/IIIa inhibitors+ nitroglycerine+verapamil | GP IIb/IIIa inhibitors, nitroglycerine, and verapamil administered before reperfusion, followed by staged restoration of flow using repeated balloon inflations to reduce no reflow and MVO on cardiac MRI | NCT05393557 |
| IOCYTE AMI-3 | FDY-5301 (sodium-iodide-based agent) | Evaluates the impact on all-cause mortality and HF of a single IV bolus injection FDY-5301 vs placebo in anterior STEMI patients | NCT04837001 |
| COOPERATION | IV dexmedetomidine | Dexmedetomidine infusion during pPCI vs placebo in patients with anterior STEMI in order to reduce infarct size on cardiac MRI | NCT04912518 |
| NORMAL | IC nicorandil | IC nicorandil administered after initial flow restoration and before stent implantation vs placebo. Endpoints: post-PCI AMR evaluation and slow flow/no reflow reduction | NCT06787430 |
| aby Abiomed. ACTRN: Australian Clinical Trials registration number; AMR: angiography-derived index of microcirculatory resistance; CP: cardiac power; GP IIb/IIIa: glycoprotein IIb/IIIa; HF: heart failure; IC: intracoronary; IV: intravenous; LV: left ventricular; MRI: magnetic resonance imaging; MVO: microvascular obstruction; NCT: National Clinical Trial; PCI: percutaneous coronary intervention; pPCI: primary PCI; RIC: remote ischaemic conditioning; SSO2: supersaturated oxygen; STEMI: ST-segment elevation myocardial infarction | |||
Conflict of interest statement
S. Brugaletta has received speaker fees from Zoll. M. Sabaté is a consultant for iVascular and Abbott. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.