Abstract
Transcatheter aortic valve implantation (TAVI) has become the preferred treatment for severe aortic stenosis. Nonetheless, interplay between aortic valve disease, transcatheter valve implantation, and the coronary arteries is frequent and clinically relevant. Coronary intervention in the context of TAVI encompasses distinct but interrelated scenarios, including the management of concomitant coronary artery disease and the prevention or treatment of coronary artery obstruction. These aspects introduce additional complexity to procedural planning and long-term management. This review provides a comprehensive and practical overview of coronary interventions related to TAVI, encompassing coronary evaluation and physiological assessment, the indications and timing of percutaneous coronary intervention before and after valve implantation, and strategies for managing coronary obstruction. Particular emphasis is placed on anatomical and device-related factors influencing coronary access, including transcatheter heart valve design, aortic root anatomy, and commissural alignment. By structuring coronary interventions according to distinct clinical scenarios, this article aims to support tailored decision-making and optimise procedural safety, feasibility, and long-term coronary management in patients undergoing TAVI.
1. Introduction
Transcatheter aortic valve implantation (TAVI) has established itself as a safe, effective, and successful strategy for treating severe aortic stenosis (AS) across all patient risk categories.123 TAVI is a less invasive alternative to surgical aortic valve replacement (SAVR) because of its minimally invasive nature, shorter recovery time, and reduced perioperative risks compared with conventional aortic valve surgery.4 Accordingly, in the most recent European Society of Cardiology (ESC) guidelines, TAVI is recommended as the preferred treatment modality for patients over 70 years of age with severe tricuspid AS.5
However, important aspects to consider in patients undergoing TAVI are the management of concomitant coronary artery disease (CAD) and the ability to access the coronary arteries, including the potential risk of coronary compromise during the procedure. These factors add significant complexity to patient management, as they influence procedural planning, the choice and timing of revascularisation, and the anticipated feasibility of future coronary reaccess.
Therefore, when considering the relationship between TAVI and the coronary arteries, patients can be broadly divided into two main groups: those with CAD present before or developing after valve implantation, and those in whom the coronary arteries may be compromised during the procedure (Central illustration).
The goal of this review is to integrate current evidence and procedural experience to guide clinical decision-making across the full spectrum of coronary interventions associated with TAVI, including the evaluation and management of CAD, the optimal timing of percutaneous coronary intervention (PCI), and strategies to ensure safe coronary access as well as the prevention and treatment of coronary artery obstruction (CAO) after valve implantation.
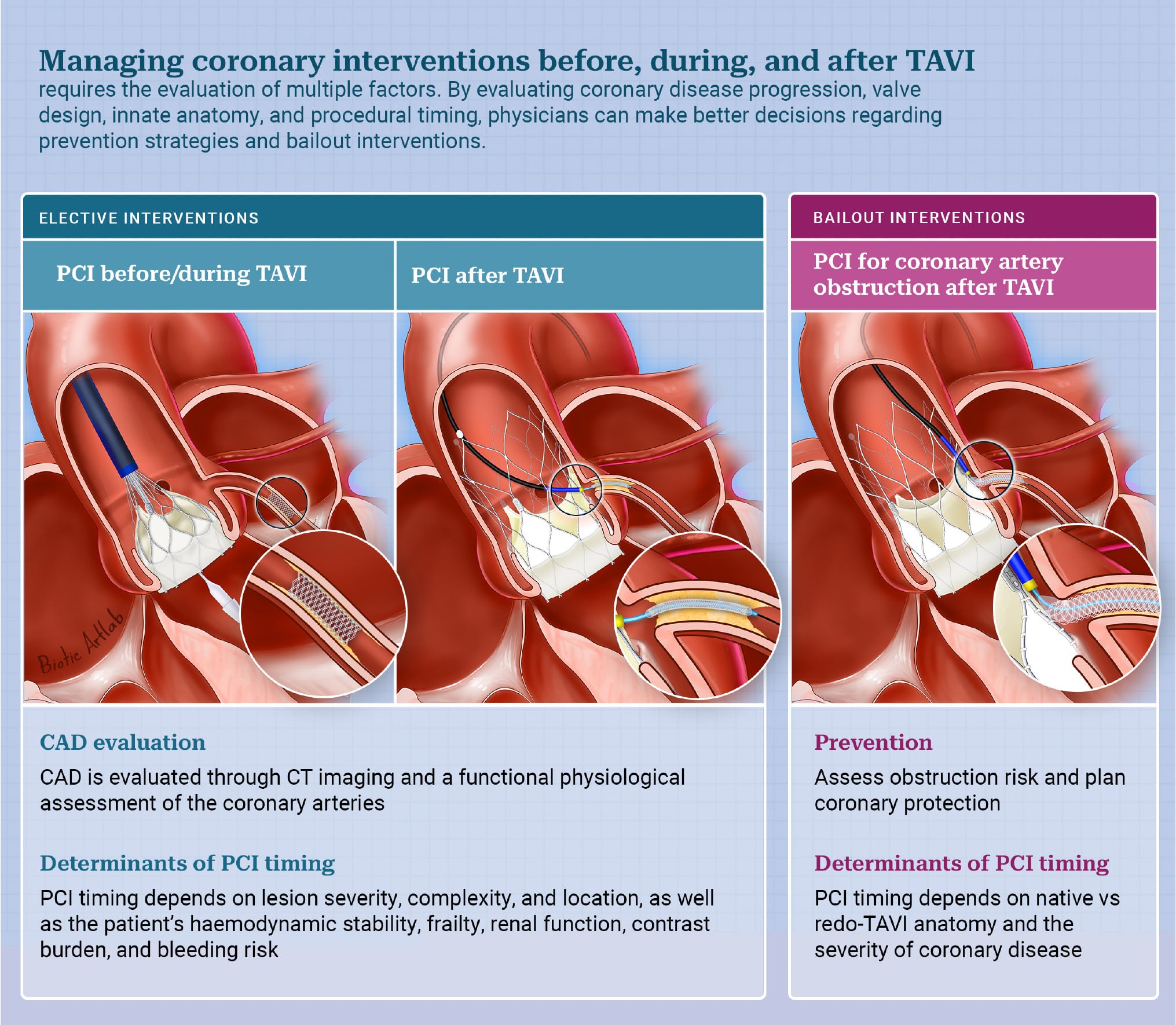
Central illustration. Coronary interventions in TAVI: clinical scenarios, timing, and preventive strategies. This illustration summarises the main clinical scenarios for PCI in patients undergoing TAVI: before, during, and after TAVI as well as in the setting of coronary artery obstruction. Procedural planning, including CT imaging and coronary assessment, is essential to guide timing, anticipate technical challenges, and optimise outcomes. Preventive strategies and procedural decisions should be tailored according to valve characteristics, coronary anatomy, and clinical context. CAD: coronary artery disease; CT: computed tomography; PCI: percutaneous coronary intervention; TAVI: transcatheter aortic valve implantation
2. CAD and TAVI
In the workup of patients with severe AS before TAVI, some form of CAD is observed in approximately 40-75% of cases, reflecting the high burden of atherosclerotic disease in this population.6 However, only a subset of these patients are considered to have significant CAD, as treatment with PCI occurs in only 10-20% of TAVI patients.7 As TAVI expands to younger patients with longer life expectancy, the development of new CAD during follow-up has become increasingly relevant.3 Moreover, residual or untreated coronary lesions prior to valve implantation may persist as potential sources of future ischaemia or adverse clinical events including acute myocardial infarction and the need for revascularisation.
Based on these considerations, two principal clinical scenarios can be delineated in the context of TAVI and CAD: (1) the evaluation and management of pre-existing CAD prior to the procedure and (2) the management of symptomatic or newly developed CAD after TAVI, presenting as either chronic coronary syndrome (CCS) or acute coronary syndrome (ACS) (Central illustration).
2.1 Evaluation of pre-existing CAD prior to TAVI and indications for PCI
In patients with coexisting AS and CAD, PCI may be required in addition to TAVI. A primary challenge in this setting is determining whether ischaemia is driven by valve stenosis, coronary stenosis, a combination of both, or unrelated mechanisms. The main objective is thus to identify coronary lesions that truly require intervention, ensuring that only those posing a meaningful clinical risk are treated. Consequently, the evaluation of CAD becomes a critical element of the preprocedural assessment, guiding procedural planning and optimising overall patient management (Figure 1).
In the earlier TAVI era, CAD screening was predominantly performed with invasive coronary angiography (ICA);2 however, undertaking ICA before TAVI adds to the complexity of the diagnostic workflow and is associated with additional in-hospital time, patient discomfort, risk of procedural complications, and increased costs. In contemporary real-world practice, fewer than 50% of patients undergoing TAVI are evaluated with ICA, as cardiac computed tomography (CT) is often sufficient for the anatomical assessment of the coronary arteries.89 In the latest guidelines, cardiac CT is recommended as the first-line modality for the evaluation of the CAD in patients undergoing TAVI.5 Therefore, ICA is now indicated only in cases where CT does not provide a reliable evaluation of the coronary anatomy, such as when image quality is limited by extensive calcification, inadequate opacification, or significant motion artefacts (Figure 1).
Once anatomical severity has been established, the next step is to assess the physiological relevance of the coronary lesions. If the diameter stenosis is ≥90%, the stenosis is considered significant,10 whereas for lesions with 50-90% stenosis, coronary physiology is essential to determine which lesions warrant revascularisation in patients undergoing TAVI, as it provides a more reliable assessment of functional significance than angiography alone.11 In general, hyperaemia-based fractional flow reserve (FFR) is preferred over resting indices such as the instantaneous wave-free ratio (iFR) (Table 1).121314 Patients with severe AS exhibit elevated baseline (resting) coronary flow, whereas hyperaemic flow is less affected.12 Resting flow-based indices are unreliable in severe AS because elevated baseline flow tends to overestimate lesion severity. In contrast, hyperaemia-based FFR is less influenced by these abnormalities in resting flow and thus provides a more reliable assessment before TAVI.1213 Therefore, a negative resting index (>0.89) can safely exclude significant CAD, whereas a positive value (<0.89) should be confirmed with FFR for definitive stratification.
Recent evidence further supports an FFR-guided strategy, showing that deferring lesions with an FFR>0.80 is safe and that FFR, interpreted as a continuum, refines risk stratification and clinical decision-making.12 Accordingly, PCI may be considered in left main disease, lesions with diameter stenosis ≥90%, or when the FFR is ≤0.80.
Another important factor that influences the decision to perform PCI in patients undergoing TAVI is the marked heterogeneity in comorbidity burden and expected lifespan across this population. A relatively young patient with low comorbidity (e.g., 72 years old with preserved functional status) has a substantially different projected risk of future coronary events and long-term exposure to valve-coronary interactions compared with a frail 85- to 90-year-old patient with chronic kidney disease or other major comorbidities. Younger TAVI candidates may derive greater long-term benefit from complete or physiology-guided revascularisation, given their longer anticipated survival. In contrast, in elderly patients or those with high comorbidity and frailty, the procedural risks and uncertain long-term benefit of PCI often favour a more conservative, symptom-driven strategy, and PCI should thus be deferred in very frail patients (Figure 1).
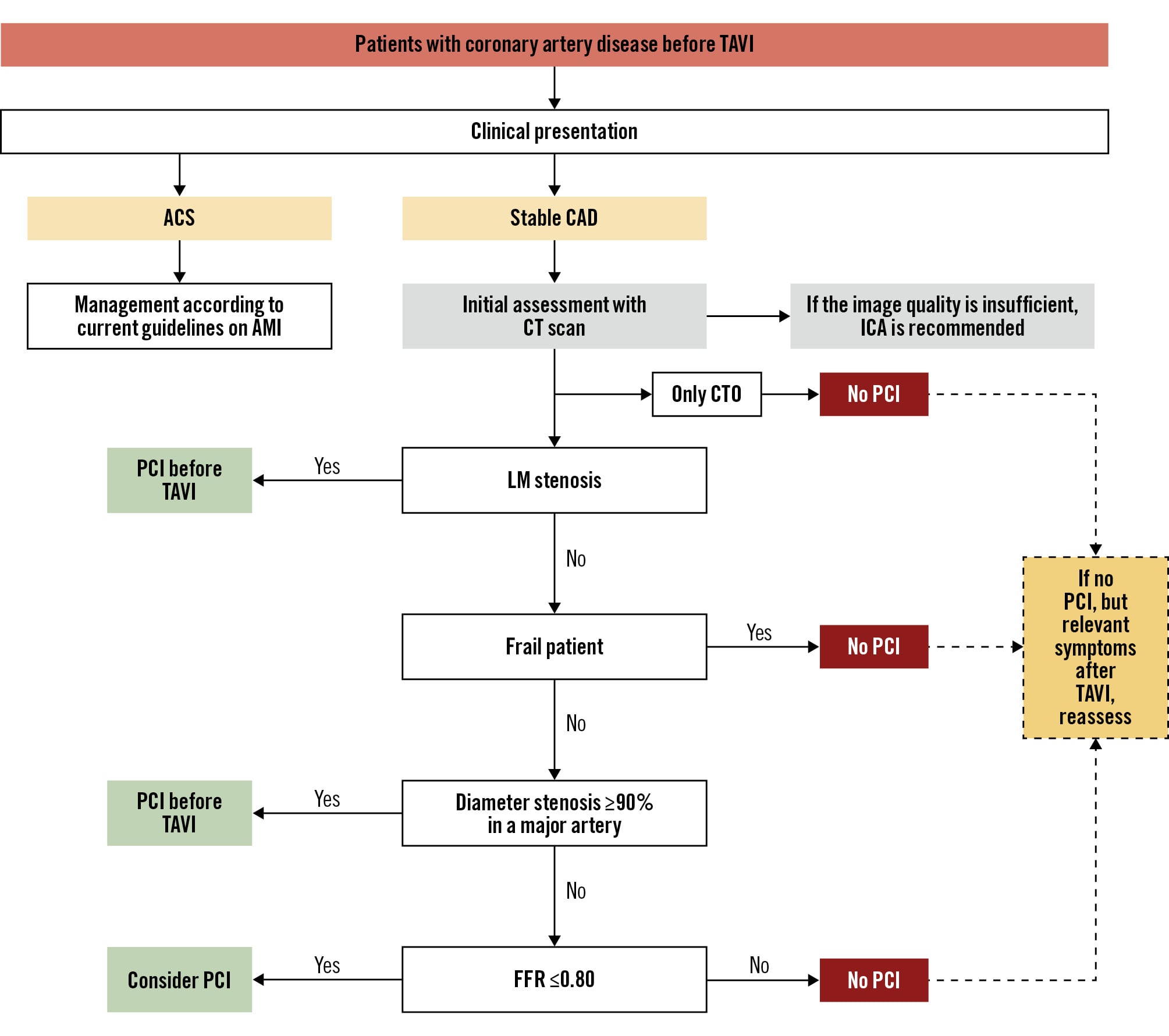
Figure 1. Algorithm for PCI before TAVI. ACS: acute coronary syndrome; AMI: acute myocardial infarction; CAD: coronary artery disease; CT: computed tomography; CTO: chronic total occlusion; FFR: fractional flow reserve; ICA: invasive coronary angiography; LM: left main; PCI: percutaneous coronary intervention; TAVI: transcatheter aortic valve implantation
Table 1. Coronary physiology evaluation: considerations before and after TAVI.
| Domain | Before TAVI | After TAVI |
|---|---|---|
| Haemodynamic environment | Severe AS is associated with increased resting flow, reduced CFR, and microvascular dysfunction | Afterload reduction, improved myocardial perfusion, and recovery of CFR and microvascular function |
| iFR/resting indices | Non-hyperaemic indices are feasible but more affected by high resting flow in AS, with frequent discordance versus FFR | As resting flow normalises post-TAVI, iFR becomes more reliable |
| FFR (preferred for pre-TAVI assessment) | FFR remains the reference standard before TAVI. FFR ≤0.80 accurately identifies significant lesions; deferral of non-ischaemic lesions is safe | FFR remains stable and reliable after TAVI |
| Pitfalls | Mild hyperaemia blunting and NHPR misclassification | Early microvascular stunning and potential coronary engagement difficulty |
| Optimal reassessment timing | FFR-guided assessment is best performed before TAVI to determine the need for PCI | If reassessment is required, waiting ≥30 days after TAVI is preferred, once haemodynamics stabilise |
| AS: aortic stenosis; CFR: coronary flow reserve; FFR: fractional flow reserve; iFR: instantaneous wave-free ratio; NHPR: non-hyperaemic pressure ratio; PCI: percutaneous coronary intervention; TAVI: transcatheter aortic valve implantation | ||
2.2 Timing of PCI in patients with pre-existing CAD prior to TAVI
After defining the anatomical and functional relevance of CAD, the next step is to determine the optimal timing of PCI in relation to TAVI, specifically whether it should be performed before, during, or after the procedure. Current guidelines do not specify the optimal chronological order for PCI and TAVI and recommend basing the decision on the angiographic pattern of CAD.5
Although clinical trials have not demonstrated a clear benefit for routinely treating coronary lesions before TAVI (Table 2), observational data have reported higher rates of acute kidney injury and early complications when PCI and TAVI are performed concomitantly.15161718192021 These associations are likely influenced by selection bias, as patients undergoing both procedures in a single session are often more unstable or present with more complex coronary anatomy. Recently, the PRO-TAVI trial demonstrated that deferring PCI for stable coronary lesions is non-inferior to routine preprocedural PCI at 1 year.22 This evidence suggests that postponing PCI does not compromise ischaemic safety and allows for a more tailored, staged strategy in the TAVI population (Table 2).
From an anatomical standpoint, guidelines and expert consensus documents suggest that PCI should be performed before TAVI in patients with severe CAD, defined as stenosis greater than 50% in the left main or greater than 70% in other major coronary arteries, particularly when these lesions have the potential to compromise haemodynamic stability during the procedure.523 Lesions located in the proximal or ostial segments of major epicardial vessels warrant special consideration, as they may precipitate periprocedural instability, especially in the presence of acute coronary syndrome, symptomatic angina, or severe stenosis of 90% (Figure 1). In addition, anomalous coronary artery origins may favour performing PCI before TAVI because of the anticipated difficulties in achieving selective coronary engagement after valve implantation.24
An important aspect of this strategy is the potential risk of bleeding complications when performing PCI before TAVI, particularly related to the need for dual antiplatelet therapy (DAPT) during the periprocedural period. This issue is especially relevant in elderly or frail patients, who are more susceptible to bleeding and other adverse events. In the NOTION-3 trial, no excess periprocedural bleeding was observed in patients undergoing TAVI while receiving DAPT, supporting the procedural safety of maintaining DAPT in patients with prior PCI.10 Another important finding was that PCI was performed before TAVI in most patients (74%), yet periprocedural complications were similar between those randomised to PCI and those assigned to a conservative strategy, suggesting that the timing of PCI may not be a major determinant of procedural risk.10
In carefully selected patients, same-session PCI and TAVI may be appropriate for non-complex lesions with clear indications for revascularisation, particularly when the coronary anatomy is straightforward, vascular access is favourable, and clinical stability is maintained. This strategy avoids a second procedure and reduces cumulative hospital exposure. However, this strategy should be avoided in patients with complex coronary anatomy, lesions of uncertain physiological significance, or impaired renal function. On the other hand, TAVI followed by PCI is preferable in patients with complex CAD or in patients with a low ejection fraction in whom PCI may risk causing haemodynamic instability.
Table 2. Comparative studies evaluating PCI performed before versus after TAVI.
| Study | Design (n) | Groups compared | HR (95% CI) | Main findings |
|---|---|---|---|---|
| Ochiai et al, 202019 | Retrospective cohort (n=258) | Pre- vs concomitant vs post-PCI | HR 0.45 (0.18-1.16) | No significant difference in 2-year MACCE among the timing strategies |
| Lunardi et al, 202220 | Single-centre cohort (n=144 PCI) | Pre-TAVI vs post-TAVI PCI | HR 0.68 (0.30-1.55) | No significant differences; a trend towards better outcomes with post-TAVI PCI |
| Rheude et al, 202315 | Multicentre registry (n=1,603) | Pre- vs post- vs concomitant PCI | HR 2.0 (1.16-3.45) | Post-TAVI PCI was associated with lower mortality; selection bias was present |
| Caminiti et al, 202421 | Systematic review/meta-analysis (n=1,531) | Pre-TAVI vs post-TAVI PCI | Adjusted HR 5.18 (1.97-8.40) | Higher mortality with pre-TAVI PCI; heterogeneous observational data |
| Wen et al, 202546 | Network meta-analysis (13 cohorts) | Pre- vs post- vs concomitant TAVI vs TAVI without PCI | - | TAVI without PCI was associated with the lowest mortality; mixed results for PCI timing |
| Delewi et al, PRO-TAVI 202622 | Multicentre RCT (n=466) | Pre-TAVI PCI vs deferred PCI | HR 0.78 (0.52-1.18) | Non-inferiority met for 1-year MACCE |
| CI: confidence interval; HR: hazard ratio; MACCE: major adverse cardiac and cerebrovascular events; PCI: percutaneous coronary intervention; RCT: randomised controlled trial; TAVI: transcatheter aortic valve implantation | ||||
2.3 PCI after TAVI
The longer life expectancy in patients undergoing TAVI today will likely result in more reinterventions in the future, whether for coronary procedures or bioprosthetic valve degeneration. [25 In general, the incidence of PCI post-TAVI is relatively low, with registry data suggesting that about 6% of patients undergoing TAVI require PCI within a period of 18 months post-TAVI. [26,27 In the context of post-TAVI management, delayed PCI can be categorised into two distinct scenarios: (1) planned, staged PCI for pre-existing coronary lesions that were not treated before valve implantation (discussed above); and (2) unplanned PCI for newly developed or symptomatic CAD, presenting either as CCS or ACS (Figure 2).
The most frequent indication for PCI after TAVI is stable angina, accounting for approximately 37.5% of cases.27 In general, post-PCI coronary assessment and indications follow the same principles as in non-TAVI patients but must be interpreted in the context of valve-coronary interactions.
After TAVI, the haemodynamic milieu changes substantially, restoring physiological aortic valve function and normalising coronary flow dynamics. Hyperaemia becomes more reliable and resting flow stabilises, improving the diagnostic performance of non-hyperaemic indices such as the iFR.13 FFR remains a stable and dependable measure both before and after TAVI, while the postprocedural restoration of microvascular reserve particularly enhances the accuracy of resting indices (Figure 2, Table 1).13
PCI is indicated in patients with persistent or recurrent angina, objective evidence of ischaemia, physiologically significant stenosis (iFR ≤0.89 or FFR ≤0.80), or in those presenting with ACS (Figure 2).111213 Deferred PCI of borderline lesions may also be re-evaluated once post-TAVI physiology has stabilised, especially those in proximal vessels or large myocardial territories (Figure 2).111213 In contrast, asymptomatic lesions without physiological significance generally do not require intervention, particularly when coronary access is expected to be challenging.
Regarding unplanned PCI after TAVI, the incidence varies depending on the patient’s risk factors for CAD. The lifetime risk of unplanned PCI after TAVI is low in patients with no CAD at the time of TAVI but accumulates over time in patients with known CAD, particularly multivessel disease. In a trial, the cumulative incidence rate of unplanned PCI at 1, 5, and 10 years was 0.1%, 0.4%, and 0.6% in patients with no CAD at the time of TAVI; 0.7%, 2.5%, and 3.4% in patients with single-vessel disease; and 1.5%, 5.4%, and 7.4% in patients with multivessel disease, respectively.7 In this scenario, the primary indication for unplanned PCI was ACS in more than half of the cases (56%).728
In a multivariate analysis, the number of diseased vessels, male sex, and younger age were independently associated with an increased risk of unplanned PCI.728 In patients who have undergone TAVI, the incidence of ACS after TAVI is approximately 4.7%. Non-ST-segment elevation myocardial infarction (NSTEMI) is the most prevalent indication (30%), followed by ST-segment elevation myocardial infarction (STEMI; 16%) and unstable angina (UA; 10%).29
Among patients undergoing PCI after TAVI in clinical trials, lesion distribution predominantly involved the left anterior descending artery (44.4%), followed by the left circumflex (28.6%), the left main (26.3%), and the right coronary artery (25.5%).7 Most lesions were de novo (73%), with restenosis accounting for 24% and stent thrombosis 1.5%.7 Although unplanned PCI is usually successful in most patients, the added structural complexity of PCI in the presence of TAVI, along with clinical conditions such as angina, cardiac arrhythmias, and haemodynamic instability, pose challenges in patients with acute coronary syndrome, further increasing the complexity.
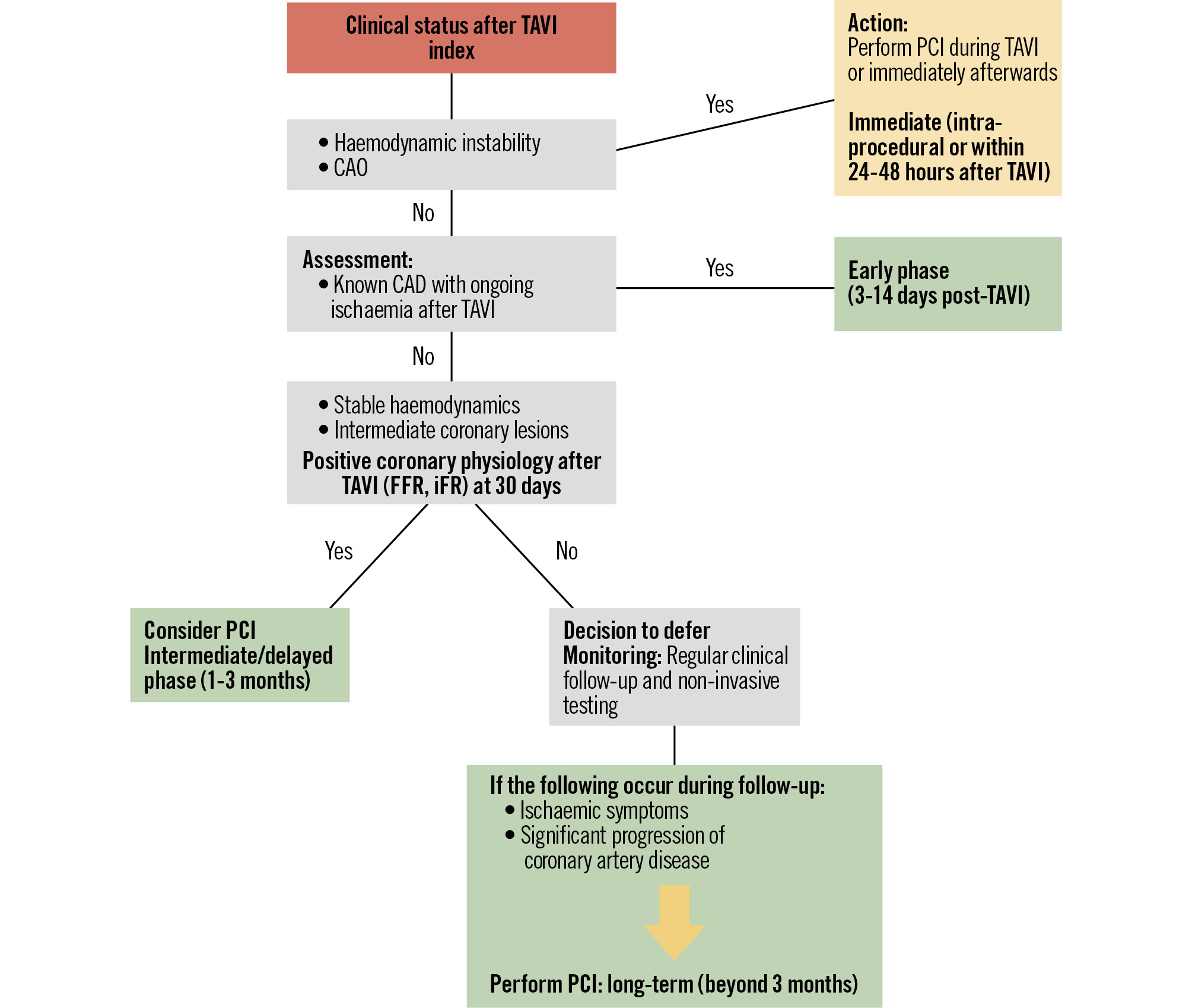
Figure 2. Algorithm for PCI after TAVI. CAD: coronary artery disease; CAO: coronary artery obstruction; FFR: fractional flow reserve; iFR: instantaneous wave-free ratio; PCI: percutaneous coronary intervention; TAVI: transcatheter aortic valve implantation
2.3.1 Complex PCI after TAVI
The presence of severe CAD is a significant factor that may influence the clinical decision-making process in AS patients. Patients with complex CAD have been excluded from randomised trials comparing TAVI and SAVR, thereby affecting the generalisability of the results to the general AS population.
Patients with multivessel coronary artery disease or reduced left ventricular ejection fraction represent an additional subgroup in whom PCI after TAVI can be particularly challenging. These patients often carry a higher ischaemic burden, impaired coronary flow reserve, and a greater risk of haemodynamic instability during the procedure. Decisions regarding staged versus more complete revascularisation must consider the feasibility of coronary engagement after valve implantation, the technical complexity of the lesions, and the expected long-term need for reliable coronary access.
In high-risk scenarios such as intervening in the left main coronary artery, a last remaining vessel, the presence of severe ventricular dysfunction, or situations in which prolonged balloon inflation or extensive lesion preparation is anticipated, temporary mechanical circulatory support may be required to maintain haemodynamic stability. The selective use of intravascular imaging or advanced calcium-modification techniques may further optimise procedural safety, although their application should be individualised to anatomical complexity and overall clinical risk.
2.4 Coronary reaccess and technical challenges of PCI after TAVI
Despite the advantages of TAVI, various difficulties have been identified in achieving coronary reaccess and performing PCI either during or after valve placement, particularly with self-expanding valves.30313233
The spatial relationship and distance between the transcatheter heart valve (THV) stent frame and coronary ostia, as well as commissural alignment, sinus of Valsalva diameter, sinus width and coronary height, must be appreciated because of the impact that these characteristics have on successful coronary artery access (Figure 3). The size of the valve, stent frame architecture, and leaflet attachment location are essential factors to consider during coronary reaccess (Figure 4, Table 3). Small valves and the use of catheters with long curves can make it more difficult to manoeuvre or rotate a catheter at the level of the annular plane, especially in catheters with preformed curves.
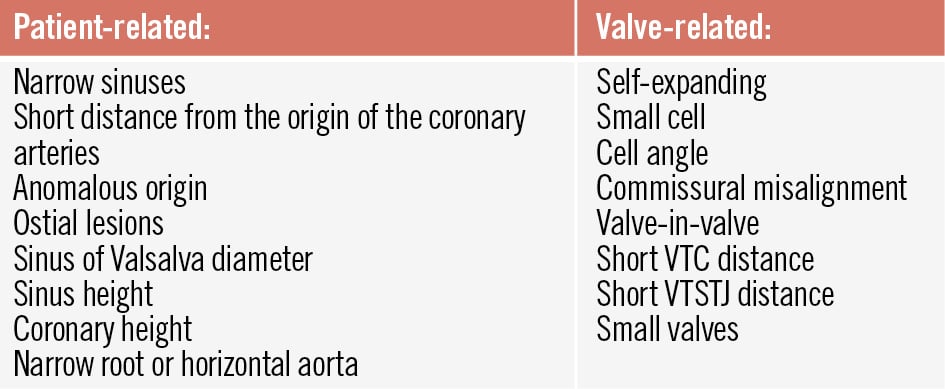
Figure 3. Factors related to the complexity of coronary reaccess. VTC: valve-to-coronary; VTSTJ: valve-to-sinotubular junction
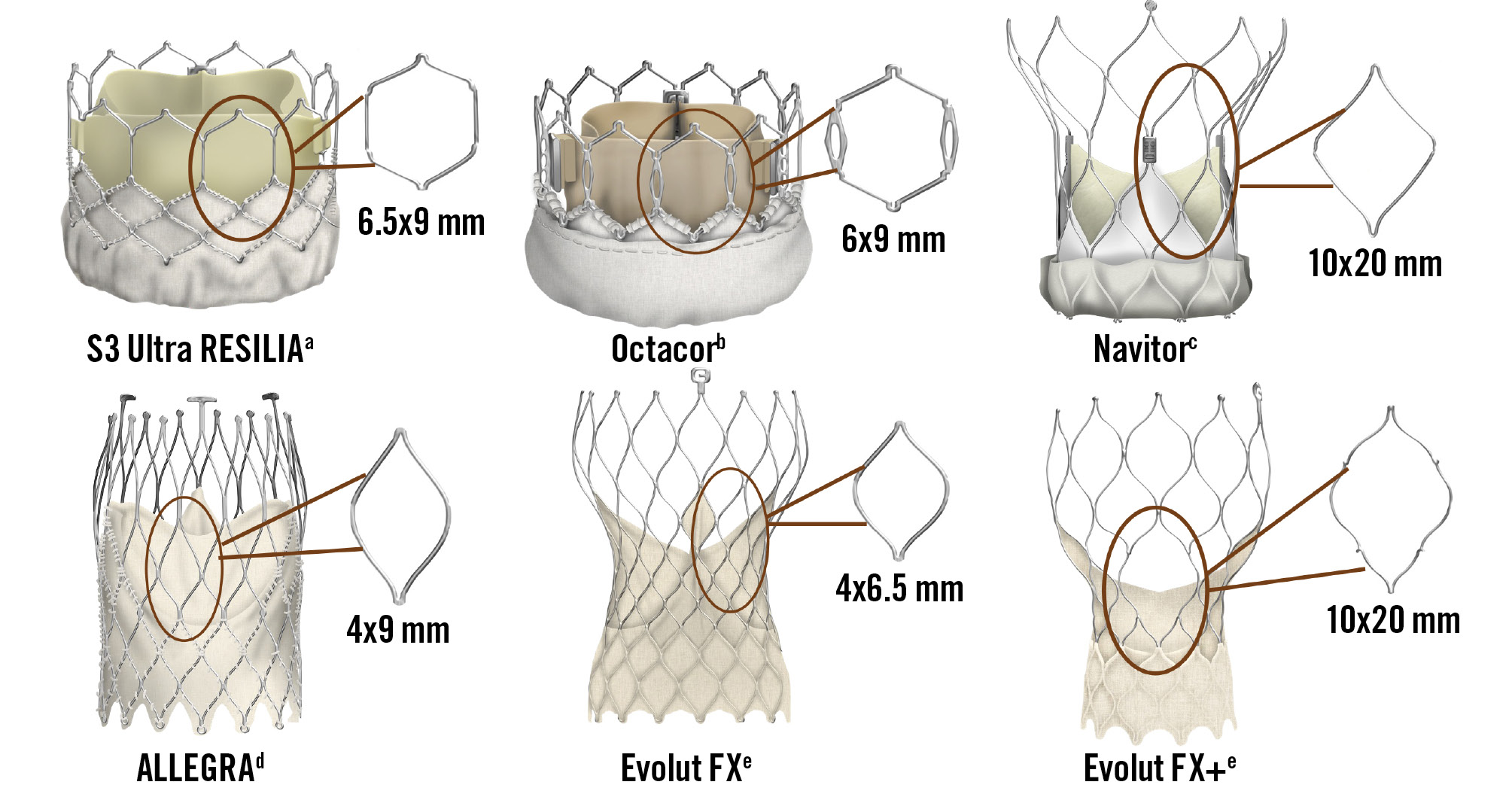
Figure 4. The most common types of valves around the world, with the shape and diameters of their cells. aBy Edwards Lifesciences; bby Meril Life Sciences; cby Abbott; dby New Valve Technology; eby Medtronic. S3: SAPIEN 3
Table 3. Structural characteristics of contemporary transcatheter aortic valves relevant to coronary reaccess.
| THV device | Type | Frame profile/height | Cell design | Frame cell diameters | Leaflet level | Coronary access implications |
|---|---|---|---|---|---|---|
| SAPIEN 3/Ultra (Edwards Lifesciences) | BEV | Short frame 15.5-22.5 mm | Large, open cells | 6.5x9 mm | Intra-annular | Highest coronary accessibility |
| Myval/Octacor (Meril Life Sciences) | BEV | Short frame 17-21 mm | Large, square BEV cells | 6x9 mm | Intra-annular | Good CA (similar to SAPIEN) |
| Portico/Navitor (Abbott) | SEV | Tall frame 47-48 mm | Very large cells | 10x20 mm | Intra-annular/low supra-annular | Favourable CA among SEVs |
| ALLEGRA (New Valve Technology) | SEV | Tall frame 37-43 mm | Small/narrow cells | 4x9 mm | Supra-annular | Potentially difficult CA |
| Evolut R/PRO/FX+ (Medtronic) | SEV | Tall frame ~43-45 mm | Small/narrow cells The FX+ incorporates two enlarged-frame cells | Evolut PRO: 4x6.5 mm Evolut FX+: 10x20 mm | Supra-annular | Most challenging CA; commissural alignment critical |
| BEV: balloon-expandable valve; CA: coronary access; SEV: self-expanding valve | ||||||
2.4.1 Practical strategies for successful coronary reaccess
Coronary reaccess after TAVI may be technically challenging and frequently requires subselective cannulation, which can increase fluoroscopy time, radiation exposure, and contrast utilisation. Despite these challenges, high procedural success rates have consistently been reported, reflecting advances in THV design, newer-generation devices, and improved procedural planning.30313233
Successful coronary engagement depends on the careful selection of catheter type and size, tailored to the valve design, aortic root anatomy, coronary ostial location, and the degree of commissural alignment or misalignment achieved during implantation. In this context, smaller catheter curves are often preferred after crossing the valve cells, whereas larger curves may be required in patients with wide sinuses of Valsalva.
Taken together, a thorough understanding of valve-specific characteristics − including frame design and cell geometry, combined with an appropriate choice of catheter shape and size, and vascular access − is essential to optimise procedural success, minimise complications, and preserve future options for coronary reintervention after TAVI (Figure 4, Table 3, Supplementary Table 1, Supplementary Figure 1). Key quantitative metrics of coronary reaccess from major prospective studies, including CAvEAT, ALIGN-ACCESS, RE-ACCESS, and RE-ACCESS 2, are summarised in Table 4.30313233
Table 4. Coronary reaccess feasibility by THV type and generation.
| Study | Sample size | Valve platforms | Selective CA (LCA/RCA) | Semiselective CA (LCA/RCA) | Unsuccessful CA |
|---|---|---|---|---|---|
| RE-ACCESS (2020)30 | n=300 | SAPIEN 3a | SAPIEN: 88%/90% | LCA: 36 patients (12.0%) | Overall: 7.7% |
| Evolut R/PROb | Evolut: 45%/48% | RCA: 95 patients (31.7%) | (22/23 Evolut) (4.7% in the LCA, 4.0% in the RCA) | ||
| ALIGN-ACCESS (2022)31 | n=206 | SAPIEN 3a (BEV) | BEV: 98%/98% | BEV: 2%/2% | BEV: 0%/0% |
| Evolut R/PROb (SEV) | Aligned SEV: 89%/79% | Aligned SEV: 10%/19% | Aligned SEV: 1%/2% | ||
| ACURATE neo2c (SEV) | Misaligned SEV: 68%/57% | Misaligned SEV: 28%/32% | Misaligned SEV: 4%/11% | ||
| RE-ACCESS 2 (2024)33 | n=127 | Evolut R/PRO/PRO+b | Evolut R/PRO/PRO+: 85%/70% | Evolut R/PRO/PRO+: 12.5%/23.7% | Evolut R/PRO/PRO+: 2.5%/6.3% |
| ACURATE neo2c | ACURATE neo2: 91.5%/83% | ACURATE neo2: 6.4%/17% | ACURATE neo2: 2.1%/0% | ||
| CAvEAT (2025)32 | n=632 | SAPIEN 3/Ultraa | SAPIEN: 89% | SAPIEN: 9% | SAPIEN: 2% |
| ACURATE neo/neo2c | ACURATE neo2: 63% | ACURATE neo2: 31% | ACURATE neo2: 6% | ||
| Portico/Navitord | Navitor: 62% | Navitor: 32% Evolut: 46% | Navitor: 6% | ||
| Evolut PRO+b | Evolut: 45% | Evolut: 9% | |||
| Selective cannulation: coaxial engagement of the coronary ostium with full contrast opacification. Semiselective: near-ostial engagement with partial opacification but usable for diagnostic angiography/PCI. aBy Edwards Lifesciences; bby Medtronic; cby Boston Scientific; dby Abbott. Failed or unfeasible cannulation was defined as the inability to achieve selective or non-selective engagement of the coronary ostium due to THV-coronary interactions, despite attempts with standard diagnostic catheters. BEV: balloon-expandable valve; CA: coronary access; LCA: left coronary artery; PCI: percutaneous coronary intervention; RCA: right coronary artery; SEV: self-expanding valve; THV: transcatheter heart valve | |||||
3. TAVI and coronary artery obstruction: risk, prevention, and treatment
Apart from planned PCI during TAVI, a primary reason for urgent PCI after valve deployment is coronary artery compromise. A feared complication during the procedure is CAO, which requires immediate PCI. CAO after TAVI carries high short-term mortality due to delayed treatment. [34 It should be emphasised that this issue is independent of the presence or absence of CAD prior to TAVI.
Acute CAO is defined as complete or partial obstruction of one or both coronary ostia during TAVI, typically manifesting as sudden haemodynamic instability and progressing rapidly to cardiogenic shock and arrhythmias.3435 The incidence in native valves is relatively low (<1%), with a 1-year mortality rate of about 45.5%.3435
Most cases of CAO occur at the time of the procedure; however, some patients may present later, mainly because of continued Nitinol expansion or valve thrombosis.3536
PCI performed immediately after TAVI for CAO can serve to prevent or treat occlusion of the coronary ostium during TAVI (e.g., the chimney/snorkel technique).36 CAO during the procedure may involve the coronary ostium, whether in patients with risk factors (where occlusion of the ostium can be provoked, either by mechanical obstruction or sinus sequestration) or in patients without risk factors (where it may be caused by mechanisms such as calcium embolism or thrombus) (Figure 5).
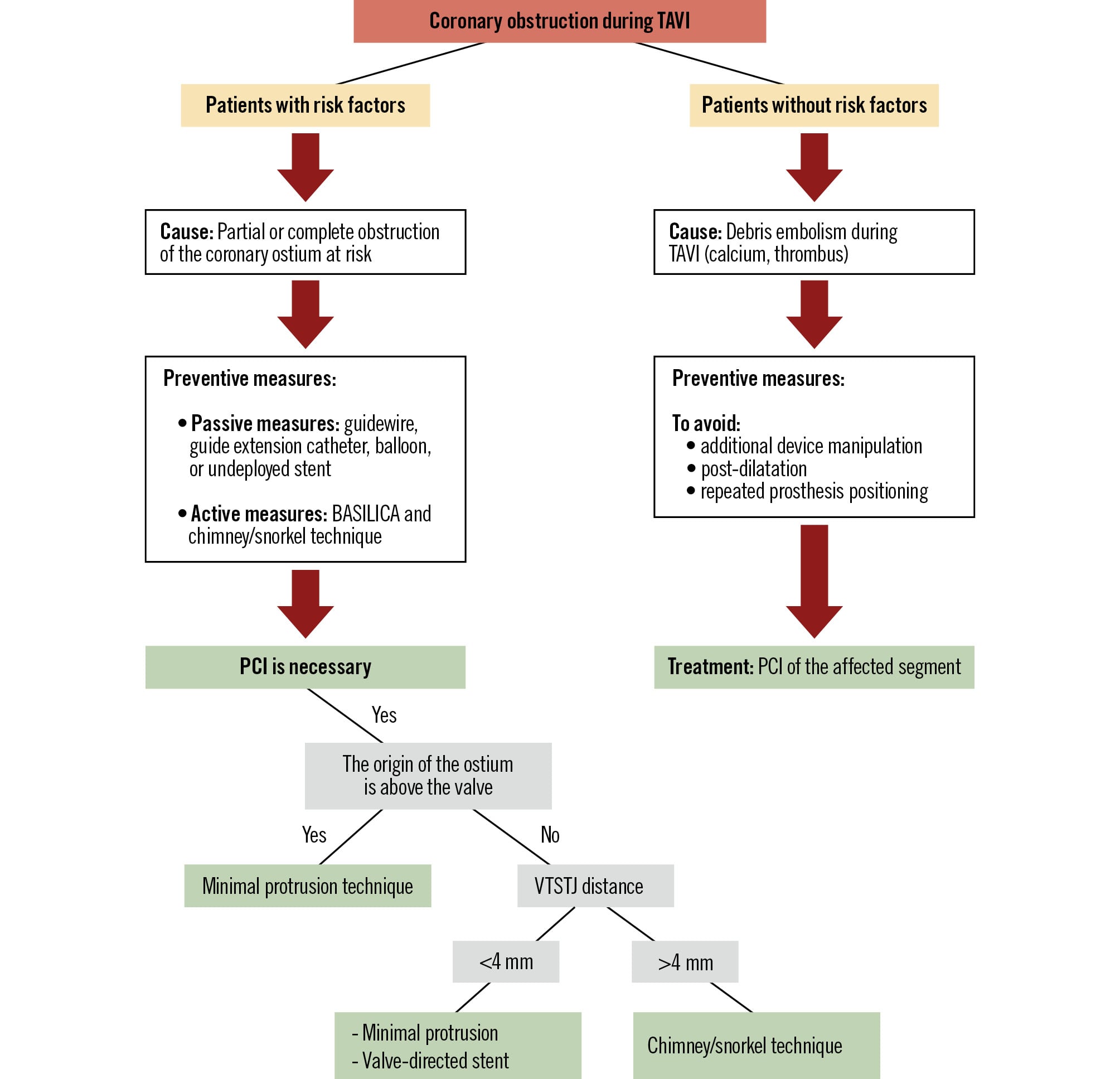
Figure 5. CAO prevention and treatment scheme. BASILICA: Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction; CAO: coronary artery obstruction; PCI: percutaneous coronary intervention; TAVI: transcatheter aortic valve implantation; VTSTJ: valve-to-sinotubular junction
3.1 Risk assessment for CAO
3.1.1 Native valves
There are various predictors of coronary obstruction prior to valve placement. In order to prevent CAO, some measurements must be performed before placing a bioprosthetic valve, for example: coronary height (from the annulus plane to the coronary artery take-off), distance from the coronary ostium to the valve, degree of calcification, distance from the aorta to the valve at the level of the sinus, diameter of the sinus of Valsalva, and length of the cusps (Figure 6).343536 In these scenarios, the main mechanism is generally the obstruction of the coronary ostia secondary to the interaction between the THV and the coronary ostia; therefore, PCI is aimed at preventing and/or treating the obstruction.
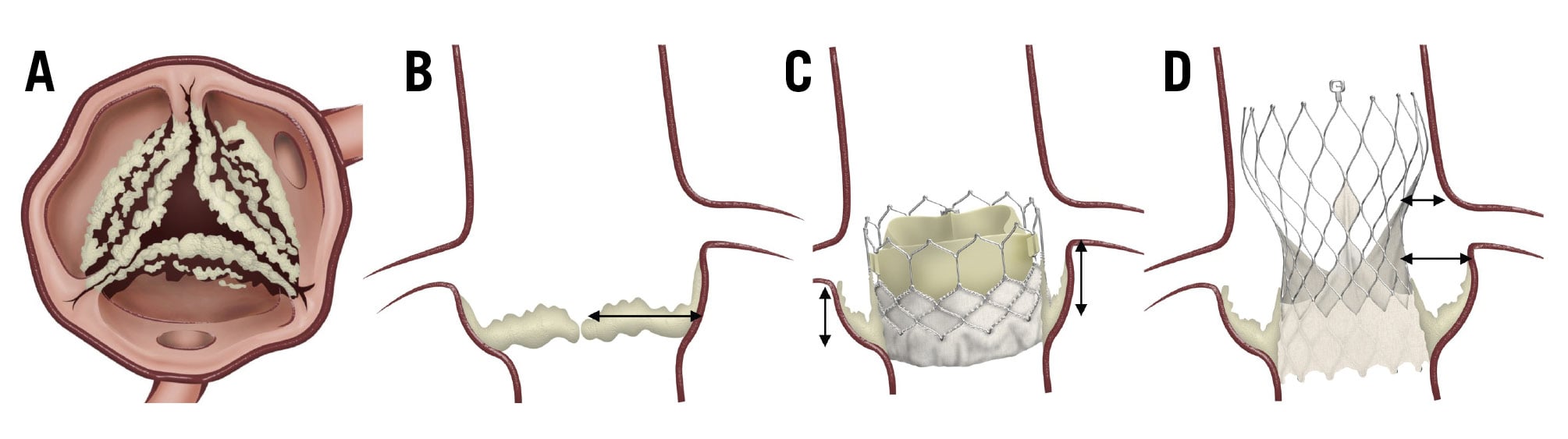
Figure 6. Risk factors for coronary artery obstruction. A) Leaflet calcification and the diameter of the sinus of Valsalva; (B) cusp length; (C) coronary height (measured from the annular plane to the coronary take-off); and (D) the horizontal distance from the coronary ostium to the transcatheter heart valve frame (neoskirt distance), as well as the distance from the aortic wall to the valve.
3.1.2 Redo-TAVI
CAO risk is known to be higher in TAVI-in-TAVI than in native TAVI.3738 This increased risk is due to the extension of the surgical aortic valve (SAV) leaflets beyond the aortic root above the sinotubular junction (STJ). After TAVI-in-TAVI, the displaced SAV leaflets create a cylinder effect, causing sinus sequestration and sealing off the flow to the coronaries.
To assess the risk of coronary obstruction in TAVI-in-TAVI, a multidetector CT scan is necessary to measure the valve-to coronary (VTC) and valve-to-STJ distances.93738 Because of the higher risk of CAO in TAVI-in-SAVR and TAVI-in-TAVI compared with TAVI in a native valve, careful planning and prevention strategies are very important, whether via passive measures or active ones, such as leaflet laceration or splitting, to prevent obstruction.3839 Table 5 and Supplementary Table 2 summarise the risk factors, prevention strategies, and treatment options depending on the type of procedure.
Table 5. Coronary artery obstruction risk/prevention.
| Risk factor | Description | Risk level | Protection strategies | Implications |
|---|---|---|---|---|
| VTC/VTSTJ | <2 mm | High | Active/passive | Critical factor; close proximity increases obstruction risk |
| VTC/VTSTJ | 2-4 mm | Intermediate | Passive | No immediate risk for coronary occlusion, but challenging coronary access can be anticipated |
| VTC/VTSTJ | >4 mm | Low | None | No need for coronary protection measurements |
| Heavy calcification | Calcification of the cusp or sinus, encroaching on the coronary ostia | Intermediate to high | Passive | The protected coronary artery will depend on the location of the calcification |
| STJ/aortic annulus mean ratio <1.2 | Limited space for valve expansion and flow | Intermediate to high | Active/passive: avoid long-frame THV | ↑ risk of sinus sequestration |
| Low coronary height (<10 mm) | Distance from the annulus to the coronary ostia | High | Passive/active | Both techniques can be used in the same procedure |
| Low and narrow STJ | Shallow sinuses; ↑ risk of sinus sequestration | High | Active: leaflet laceration Passive: avoid long-frame THV | Narrow sinuses increase CAO risk |
| Valve type: stentless or internally stented bioprosthesis | Leaflets can move outward and obstruct coronaries | High | Active/passive | Both techniques can be used in the same procedure |
| Passive techniques: (1) use of protective guidewire, balloon, prepositioned stents, or guide extension catheter in coronaries during TAVI; (2) commissural alignment, avoid long-frame THV. Active techniques: (1) chimney/snorkel stenting: simultaneous stenting to maintain ostial patency; (2) leaflet laceration techniques: lacerate the leaflet to prevent obstruction during valve deployment (BASILICA, UNICORN). BASILICA: Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction; CAO: coronary artery obstruction; TAVI: transcatheter aortic valve implantation; THV: transcatheter heart valve; UNICORN: Undermining Iatrogenic Coronary Obstruction with Radiofrequency Needle; VTC: valve-to-coronary; VTSTJ: valve-to-sinotubular junction | ||||
3.2 Preventive strategies
The main objective in a patient with a high probability of CAO during TAVI is to assess which strategy will be used (prevention and/or treatment strategy) (Figure 5, Table 5, Supplementary Table 2).
The application of passive coronary protection measures − such as using a guidewire, guide extension catheter, balloon, or undeployed stent in the distal artery (or arteries) at risk − has been suggested in patients considered at risk of CAO prior to THV deployment.40 If there is no coronary compromise after valve deployment, the protection device is removed. If flow is compromised during or after deployment, the stent should be retracted to free the ostium, extending from the proximal coronary artery cranially, laterally, and parallel to the THV (Figure 7).
Another way to prevent CAO is through active prevention measures, in which a procedure is performed as a protective technique (Figure 5, Table 5, Supplementary Table 2). Currently, leaflet modification and the chimney/snorkel technique are two consolidated strategies to prevent coronary obstruction during TAVI.404142 The chimney/snorkel technique is not only useful for treating a new complete or partial obstruction of a coronary ostium but has also been used as a prophylactic treatment in cases of impending CAO, where the stent is released immediately after valve deployment.42 For their part, leaflet laceration techniques have been designed to mitigate this risk. Among the most studied methods is Bioprosthetic or native Aortic Scallop Intentional Laceration to prevent Iatrogenic Coronary Artery obstruction (BASILICA), which uses transcatheter electrosurgery to lacerate the aortic valve leaflet and maintain coronary perfusion.42 Other promising techniques include ShortCut (Pi-Cardia), a mechanical leaflet splitting device, and Undermining Iatrogenic Coronary Obstruction with Radiofrequency Needle (UNICORN), which utilises radiofrequency energy to achieve leaflet laceration.43
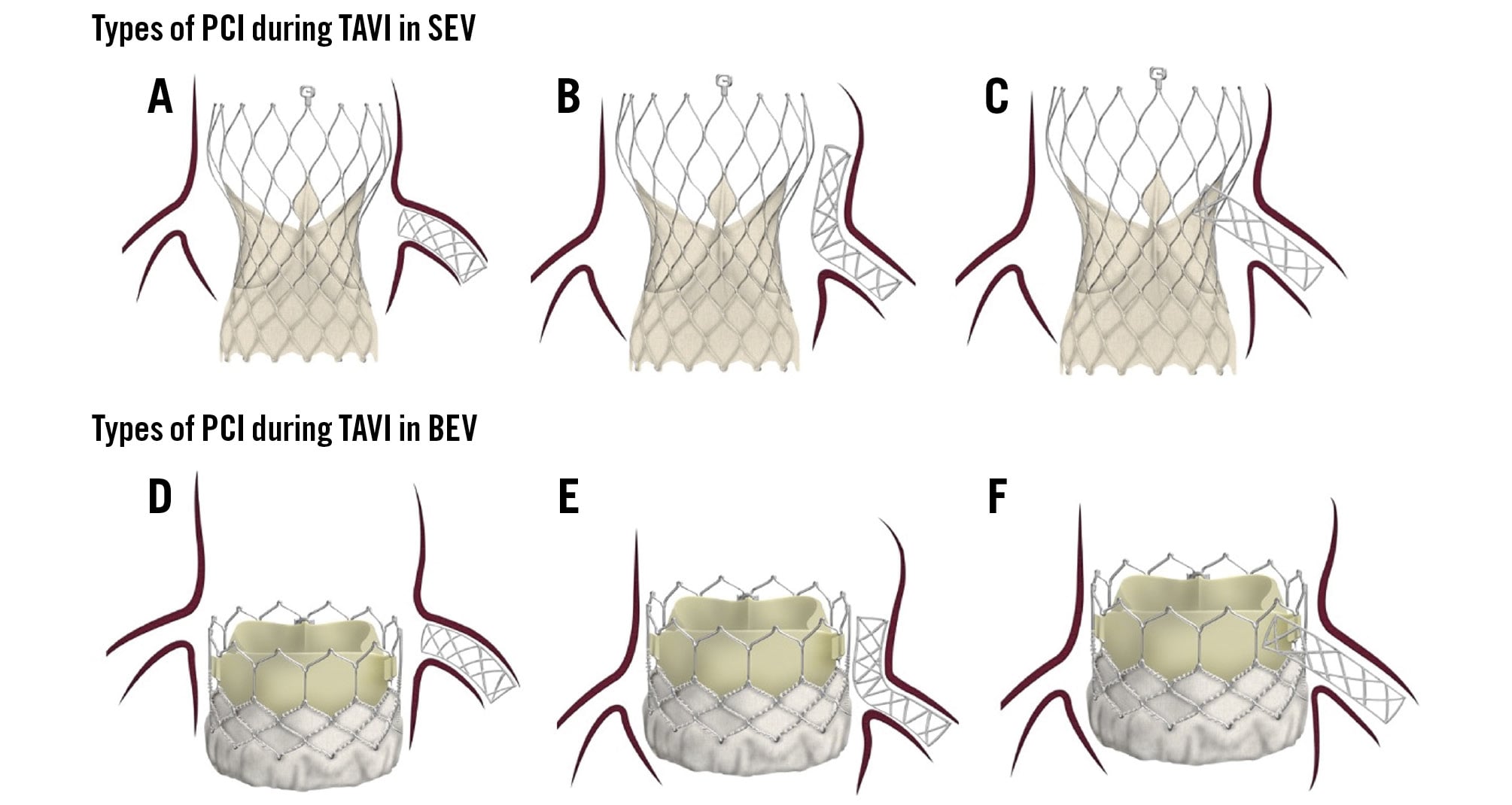
Figure 7. PCI types in different types of valves. A) PCI with minimal stent protrusion due to limited space between the valve and the STJ. B) Adequate space between the valve and the STJ, allowing for the chimney technique. C) Valve-directed stenting from the coronary ostium towards the valve frame. D) PCI with minimal protrusion, as the coronary ostium is located above the valve. E) Coronary ostium located below the valve frame, with sufficient space between the valve and the STJ to perform the chimney/snorkel technique. F) Coronary ostium located below the valve frame, with limited space between the valve and the STJ; therefore, stenting is directed from the ostium towards the valve. BEV: balloon-expandable valve; PCI: percutaneous coronary intervention; SEV: self-expanding valve; STJ: sinotubular junction; TAVI: transcatheter aortic valve implantation
3.3 Bailout PCI for coronary obstruction
3.3.1 With risk factors
When PCI is performed to treat complete or partial coronary ostial obstruction following valve deployment, the revascularisation strategy depends on the anatomical characteristics of the aortic root, including sinus dimensions, coronary height, and the interaction between the THV and the STJ.37 In this context, three main bailout strategies have been described: the chimney or snorkel stent technique, which involves coronary stent implantation with variable protrusion into the aorta through the frame of the implanted transcatheter valve; conventional ostial stenting with minimal protrusion; and valve-directed stenting, in which the stent is deployed from the coronary artery up to the prosthetic frame (Figure 5, Figure 7).4142 The choice of bailout technique is strongly influenced by the type of THV, particularly balloon-expandable versus self-expanding designs. Careful assessment of the aortic root anatomy is essential, as coronary engagement may be relatively straightforward when the coronary ostia or the STJ are located above the valve frame, allowing stent deployment above the frame and making both chimney and conventional ostial stenting feasible (Figure 5, Figure 7). In contrast, when the coronary ostium originates below the upper border of the valve frame, bailout PCI becomes technically challenging. In these cases, precise evaluation of the valve-to-STJ and VTC distances is critical to guide the choice of revascularisation strategy. A valve-to-STJ distance greater than 4 mm generally favours the chimney or snorkel technique, whereas shorter distances increase the risk of stent interaction with the valve frame and may favour minimal ostial protrusion or valve-directed stenting.343541
Redo-TAVI represents a particularly complex scenario for bailout PCI, as coronary reaccess is affected by the interaction between two THV frames with different geometry and cell morphology. Overlap between valve cells is more likely when the second valve has smaller cells, especially when the coronary ostia originate below the upper frame of the first valve. Commissural misalignment may further exacerbate this phenomenon by leading to the superposition of neocommissures, increasing cell overlap and impairing coronary engagement. Valve-in-valve procedures involving self-expanding valves, either within another self-expanding valve or a balloon-expandable valve, may further complicate coronary access because of asymmetric and non-uniform frame structures, whereas balloon-expandable valves provide a more uniform architecture that may facilitate valve-in-valve procedures. Additional anatomical constraints, including a valve-to-STJ distance below 3.5 mm and a VTC distance below 2 mm, have been associated with increased difficulty or failure of coronary reaccess and bailout PCI after redo-TAVI.37
3.3.2 Without risk factors
Despite the absence of risk factors for CAO after TAVI, events such as calcium embolism or thromboembolism can lead to coronary obstruction (Figure 5). In these cases, mobilisation of calcified nodules towards the ostium may result in embolisation of debris or thrombi within the coronary arteries.44
Coronary embolism after TAVI remains less investigated and potentially overlooked. The reported incidence is less than 1%.44 Overall, TAVI-associated coronary embolism often presents with proximal vessel occlusion causing STEMI and haemodynamic instability. However, it can also present with distal vessel occlusion and minor symptoms that may be missed during the periprocedural period. Due to the increasing number of procedures and the presence of complex (calcified) anatomies, the prevalence of TAVI-related coronary embolism is now higher than previously documented.
Similarly to early ischaemic cerebrovascular events, the clinical presentation of coronary thromboembolism often occurs periprocedurally. Debris captured by embolic protection devices, used as a preventive measure during TAVI, can contain fresh or organised thrombus, valve and arterial wall fragments, cardiomyocytes, endothelial strands, collagenous tissue, calcification, and foreign material. The primary mechanisms involve additional device manipulations, postdilatation, and valve redeployments, which increase the risk of valvular debris, captured in devices like SENTINEL (Boston Scientific).45 These mechanisms may also be involved in the primary aetiology of coronary embolism.
Distal or proximal coronary embolisation typically occurs within minutes after valve deployment. Its clinical impact depends on the vessel and segment affected. Larger arteries tend to lodge emboli distally, often without symptoms; in smaller arteries such as the non-dominant right coronary artery, proximal segments may be affected, leading to symptoms. Therefore, treatment is directed at the affected segment (Figure 5). While coronary height is an essential consideration, it is equally important to consider calcium distribution and the length of calcified leaflets to anticipate any potential occlusion of the coronary ostium.
Conclusions
PCI related to TAVI can be divided into two overarching groups with distinct clinical implications. The first comprises PCI performed to address CAD, whether pre-existing or newly symptomatic following TAVI. The second includes PCI related to TAVI-specific complications, particularly preventative or emergent interventions for CAO. This classification helps standardise decision-making and highlights the different anatomical, temporal, mechanistic, and technical considerations associated with coronary intervention in TAVI patients.
Conflict of interest statement
O. De Backer has received institutional research grants and consulting fees from Abbott, Boston Scientific, Medtronic, and Microport. G.H.L. Tang has received speaker honoraria and served as a physician proctor, consultant, advisory board member, TAVR publications committee member, RESTORE study steering and screening committee member, APOLLO trial screening committee member and IMPACT MR steering committee member for Medtronic; has received speaker honoraria and served as a physician proctor, consultant, advisory board member, ENVISION trial screening committee member, and TRILUMINATE trial anatomic eligibility and publications committee member for Abbott; and has served as an advisory board member for Boston Scientific, Anteris, Philips, Edwards Lifesciences, Peija Medical, and Shenqi Medical Technology. I.J. Amat-Santos is a physician proctor and consultant for Medtronic, Boston Scientific, and Meril Life. D. Tchétché has received honoraria or consultation fees from Abbott, Boston Scientific, Edwards Lifesciences, and Medtronic. M. Barbanti is a consultant for Edwards Lifesciences, Boston Scientific, and Medtronic. A. Regueiro has been a proctor for Abbott. N. Piazza is a consultant/proctor for Peijia, HighLife, and Medtronic. G. Tarantini has received lecture fees from Medtronic, Edwards Lifesciences, Abbott, and Boston Scientific. The other authors have no conflicts of interest to declare relevant to the contents of this paper.
Supplementary data
To read the full content of this article, please download the PDF.