Abstract
Background: Catheter-based renal denervation (RDN) is a guideline-recommended therapy for uncontrolled hypertension. Late-term follow-up among RDN trials is essential to characterise the durability of its efficacy, and further study is needed to ascertain the proportion of patients experiencing a clinical benefit.
Aims: We aimed to evaluate 36-month blood pressure (BP) changes after radiofrequency (RF)-RDN across four clinical studies from the SPYRAL programme and to determine the proportion of patients who experienced a clinical benefit.
Methods: Data were pooled from the Global SYMPLICITY Registry DEFINE, SPYRAL First-In-Human, and SPYRAL HTN-OFF MED and -ON MED trials. All patients were treated with RF-RDN (Symplicity Spyral). Medications, BP changes, and adverse events were evaluated through 36 months.
Results: A total of 2,137 patients treated with RF-RDN using the Spyral device were included in the analysis. Baseline office systolic (OS)BP was 163±23 mmHg, baseline 24-hour ambulatory systolic (AS)BP was 152±17 mmHg, and the baseline number of antihypertensive medications was 3.8±2.1. At 36 months, the number of medications was 3.5±1.9, and reductions in OSBP and ASBP were significant (–18.1±23.4 mmHg and –13.3±17.6 mmHg, respectively; p<0.0001). Overall, adverse event rates were low. The proportion of patients who experienced a reduction in OSBP ≥10 mmHg, ASBP ≥5 mmHg, and/or ≥1 medication was 88% at 36 months.
Conclusions: In this large, pooled cohort of Spyral RF-RDN patients, there were significant BP reductions through 36 months with few adverse events. Additionally, nearly 9 out of 10 patients experienced a clinical benefit. These findings suggest the long-term efficacy and safety of RF-RDN across a broad spectrum of patients with uncontrolled hypertension.
Hypertension is the leading modifiable risk factor for cardiovascular disease and remains a major global health challenge, affecting more than 1 billion adults worldwide.123 Despite the established efficacy of lifestyle interventions and antihypertensive (AH) medications, adherence remains poor, and a significant proportion of hypertensive patients have persistent uncontrolled blood pressure (BP), underscoring the need for alternative therapeutic options to achieve and maintain BP control.4 Catheter-based renal denervation (RDN) is a minimally invasive, guideline-recommended procedure that targets sympathetic nerves in the renal arteries, offering a novel approach to treat hypertension.5678 Multiple randomised, sham-controlled trials and global registries have demonstrated the safety and efficacy of RDN, both in the presence and absence of AH medications.91011121314 Although the results of recent pooled studies and meta-analyses across numerous different populations and device types suggest a consistent, durable BP-lowering effect with RDN,15161718 a systematic assessment of the long-term efficacy and safety of RDN using the latest-generation, U.S. Food and Drug Administration-approved, Symplicity Spyral multielectrode radiofrequency (RF) catheter (Medtronic) remains warranted. Moreover, while multiple studies have investigated which patients are most likely to experience a clinical benefit after the procedure, only higher preprocedure baseline BP has been consistently associated with future BP response.1516 However, a broader question remains unaddressed that is essential to informing practice: what proportion of patients experience a meaningful clinical benefit after RDN?
We leveraged comprehensive follow-up data from over 2,000 patients in the SPYRAL clinical trial programme, including the Global SYMPLICITY Registry (GSR) DEFINE, SPYRAL First-In-Human (FIH), and the SPYRAL HTN-OFF MED and -ON MED trials to evaluate long-term changes in BP, prescribed AH medications, and safety outcomes among RDN patients treated with the Spyral device through 3 years.9101219 Additionally, we evaluated the proportion of hypertensive patients who experienced a clinical benefit after undergoing RDN with the Spyral device.
Methods
Study designs and patient population
This post hoc analysis included patients from GSR DEFINE who were treated with the latest-generation Spyral catheter, those included in SPYRAL FIH, and those randomised to the RDN cohorts from the randomised controlled SPYRAL HTN-OFF MED and -ON MED trials.9101112 Details of the study designs have been previously published.122021 Follow-up through 3 years was prespecified for all 4 studies. GSR DEFINE is an all-comers, real-world, international registry evaluating the safety and efficacy of RF-RDN. SPYRAL FIH was a feasibility study of the Symplicity Spyral RF-RDN catheter in patients with an office systolic BP ≥160 mmHg, or ≥150 mmHg for those with type 2 diabetes, despite prescription of ≥3 AH medication classes. The SPYRAL HTN-OFF MED and SPYRAL HTN-ON MED studies were global, randomised, blinded, sham-controlled trials evaluating the safety and efficacy of RF-RDN using the Spyral device in the absence or presence of AH medications, respectively. Eligible patients had an office systolic BP ≥150 and <180 mmHg, an office diastolic BP ≥90 mmHg, and a 24 h ambulatory systolic BP ≥140 and <170 mmHg. In the OFF MED trial, enrolled patients remained off medications for the first 3 months, whereas in the ON MED trial, patients were prescribed a stable regimen of 1-3 AH medications through 6 months.
Procedure
The procedure was performed using the Symplicity Spyral multielectrode RDN catheter and the Symplicity G3 RDN RF generator (Medtronic) to deliver circumferential RF ablation to the renal arteries and all accessible branch vessels with diameters of 3-8 mm.12 All cases were performed by an experienced operator and, in the case of the OFF and ON MED trials, were also case-supported according to predetermined treatment plans.
Follow-up
Patients had planned follow-up at 3, 6, 12, 24, and 36 months. Office and 24 h ambulatory BP, medication information, and adverse events − including renal artery stenosis, stroke, death, cardiovascular death, myocardial infarction (MI), and hospitalisation for a hypertensive emergency or crisis − were recorded at each follow-up.
Statistical analysis
Categorical variables are shown as percentages and counts (N), whereas continuous variables are reported as mean±standard deviation. Changes in continuous variables from baseline to follow-up were evaluated using paired t-tests. Patients with complete follow-up at 36 months versus those without were compared using Fisher’s exact test for categorical variables and t-tests for continuous variables. The cumulative proportions of subjects who experienced adverse events across all studies were summarised based on available follow-up. Mixed models for repeated measures were fitted with office and ambulatory systolic BP as outcome variables. The models included the study, baseline BP, and the number of AH medications over time as fixed effects; subject was included as a random effect using a first-order autoregressive covariance structure. As a separate analysis, we calculated the proportion of patients that experienced either a ≥10 mmHg office systolic BP reduction, a ≥5 mmHg 24 h ambulatory systolic BP reduction, a reduction of ≥1 AH medication, or a combination thereof. For this analysis, we considered all Spyral-treated patients who completed 36-month follow-up and had uncontrolled BP (office systolic BP ≥140 mmHg) at baseline.
Role of the funding source
All studies were funded by Medtronic. The executive committees, in collaboration with the funder, designed the protocols and identified suitable clinical sites for the studies. The funder was responsible for transparent data collection, monitoring, and analysis. The lead author wrote the manuscript with contributions from the co-authors and copyediting assistance from the funder. Medtronic aided in figure preparation, table generation, and manuscript formatting. All authors had full access to the data and were solely responsible for the submission for publication. The data are proprietary; however, they may be available upon reasonable request to the first author.
Results
Patient characteristics
As of September 2025, data were pooled from 2,137 patients treated with the Symplicity Spyral device across the 4 studies of the SPYRAL clinical programme (Central illustration). Patient demographics at baseline are provided in Table 1. At baseline, patients were 58±13 years old, and 38.8% were female. Baseline office and 24 h ambulatory systolic BPs were 163±23 mmHg and 152±17 mmHg, respectively. The mean number of AH medications at baseline was 3.8±2.1. Among pooled patients, 3.6% had a history of MI, 29.9% had type 2 diabetes, 3.3% had prior stroke, 18.2% had sleep apnoea, 7.9% had atrial fibrillation, and 34.2% had a history of smoking. The mean estimated glomerular filtration rate (eGFR) was 78.1±25.4 mL/min/1.73 m2, with 22.0% having chronic kidney disease (eGFR <60 mL/min/1.73 m2). Procedural characteristics are provided in Supplementary Table 1.
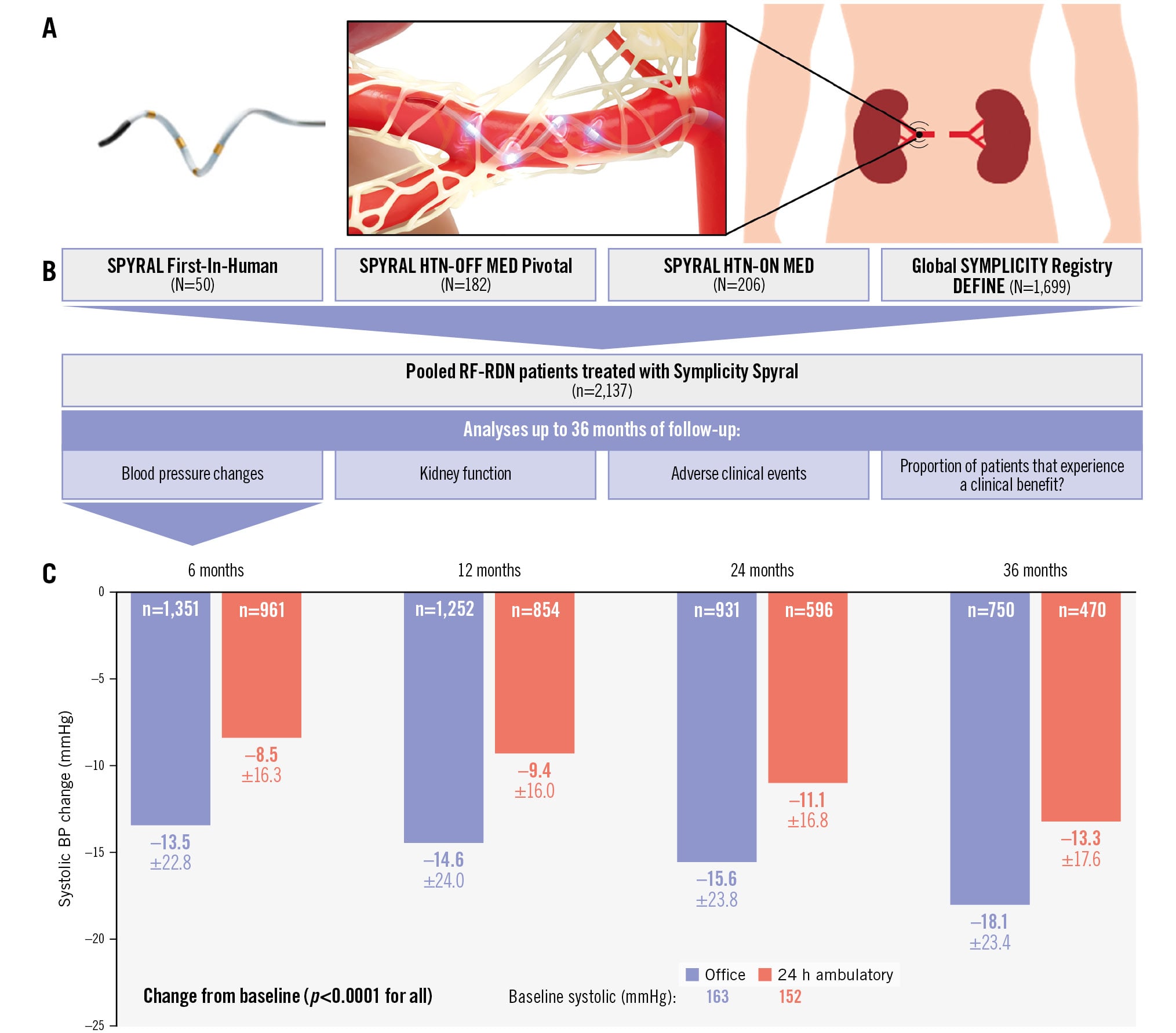
Central illustration. Flowchart and blood pressure changes among pooled patients treated with the Spyralradiofrequency RDN device. Data from 2,137 patients treated with the Spyral radiofrequency renal denervation device (A) were pooled from 4 studies: SPYRAL First-In-Human, SPYRAL HTN-OFF MED, SPYRAL HTN-ON MED, and the Global SYMPLICITY Registry DEFINE (B). Among pooled Spyralpatients, the office (blue) and 24 h ambulatory (red) systolic BP changes from baseline to 36 months were statistically significant (C). BP: blood pressure; RF-RDN: radiofrequency renal denervation
Table 1. Patient baseline characteristics.
| Pooled Spyral (n=2,137) | |
|---|---|
| Office systolic BP, mmHg | 163±23 |
| Office diastolic BP, mmHg | 93±16 |
| 24 h ambulatory systolic BP, mmHg | 152±17 |
| 24 h ambulatory diastolic BP, mmHg | 90±14 |
| Age, years | 58±13 |
| Male | 61.2 (1,308) |
| BMI, kg/m2 | 30.6±6.4 |
| eGFR, mL/min/1.73 m2 | 78.1±25.4 |
| CKD (eGFR <60 mL/min/1.73 m2) | 22.0 (454) |
| Previous myocardial infarction | 3.6 (76) |
| Type 2 diabetes mellitus | 29.9 (630) |
| Prior stroke | 3.3 (68) |
| Heart failure | 3.3 (70) |
| Sleep apnoea | 18.2 (354) |
| Atrial fibrillation | 7.9 (166) |
| Number of antihypertensive medications | 3.8±2.1 |
| Data are presented as mean±SD or % (n). BMI: body mass index; BP: blood pressure; CKD: chronic kidney disease; eGFR: estimated glomerular filtration rate; SD: standard deviation | |
Blood pressure changes and medications THROUGH 36 months
In GSR, follow-up through 36 months is still ongoing for many patients, with 24% (401/1,699) and 12% (208/1,699) having completed 36-month office BP and 24 h ambulatory BP measures, respectively, as of March 2025. Importantly, it was not mandated that 24 h ambulatory BP measures be collected in GSR. In the SPYRAL First-In-Human, OFF MED, and ON MED studies, 82% (41/50), 85% (154/182), and 85% (175/206) of patients, respectively, completed their 36-month office BP measures, and 70% (35/50), 71% (129/182), and 75% (155/206), respectively, completed their 36-month 24 h ambulatory BP measures. At 36 months after RF-RDN, the pooled patient cohort had statistically significant reductions in office systolic BP (–18.1±23.4 mmHg), 24 h ambulatory systolic BP (–13.3±17.6 mmHg), office diastolic BP (–8.1±13.9 mmHg), and 24 h ambulatory diastolic BP (–8.7±10.6 mmHg; p<0.0001 for all) (Central illustration, Supplementary Figure 1). Among a matched patient cohort with available follow-up through 36 months, BP reductions increased over time (Supplementary Figure 2). A mixed model − accounting for missing data, baseline BP, differing studies, and changing medications throughout long-term follow-up − yielded similar results (Supplementary Figure 3). The benefit of RDN was observed throughout the 24-hour period, with significant systolic and diastolic BP reductions at 36 months during both daytime and nighttime (Figure 1). The pooled patient population had greatly improved BP control after RF-RDN through 36 months (Figure 2). The number of AH medications among the pooled cohort from baseline to 36 months is plotted in Figure 3. At 36 months, the mean eGFR among pooled Spyral patients was 75.6±23.2 mL/min/1.73 m2.
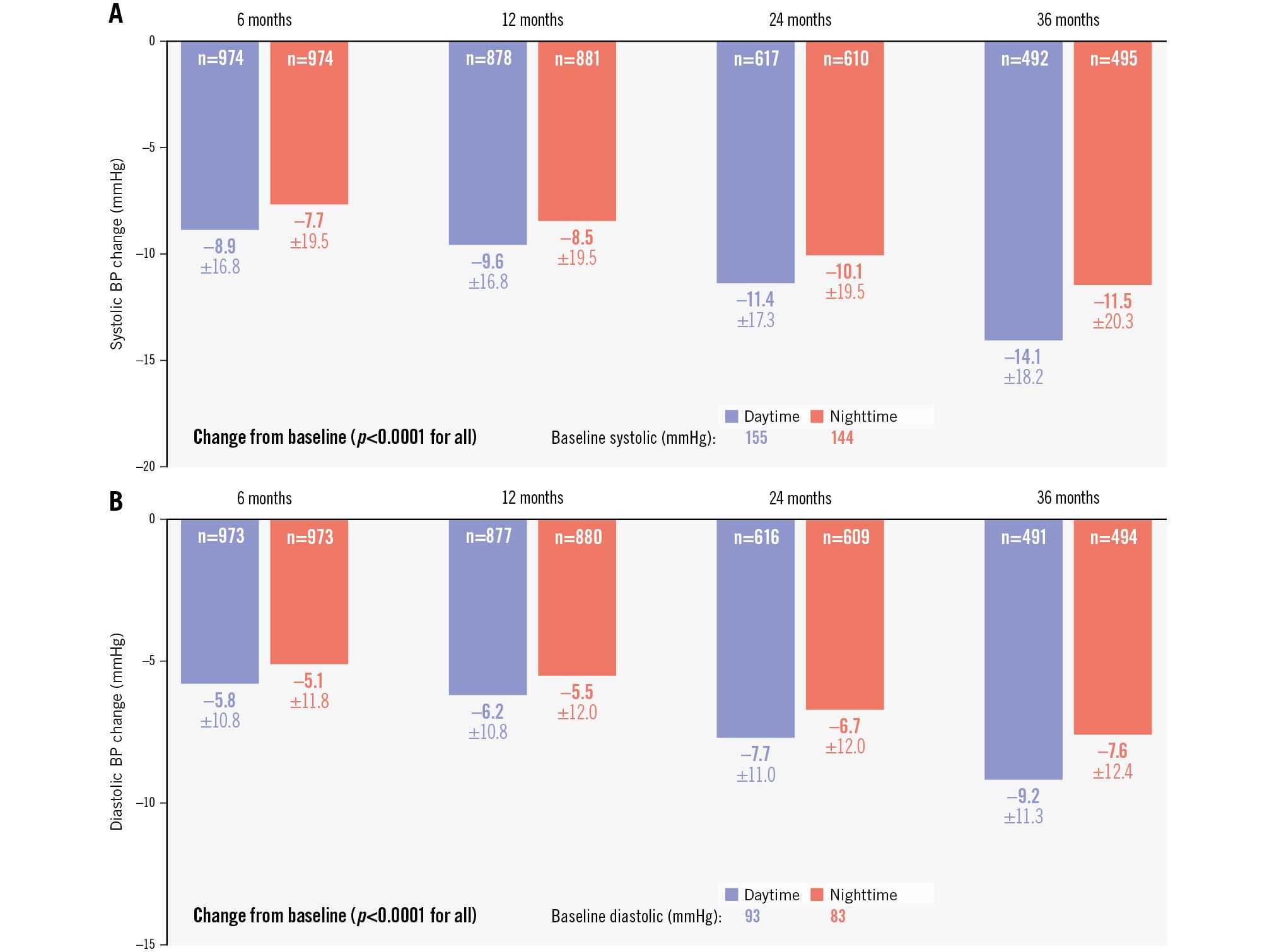
Figure 1. Daytime and nighttime systolic and diastolic ambulatory BP changes through 36 months. The daytime (blue) and nighttime (red) systolic (A) and diastolic (B) BP changes of the pooled Spyral cohort from baseline through 36 months are plotted. BP: blood pressure
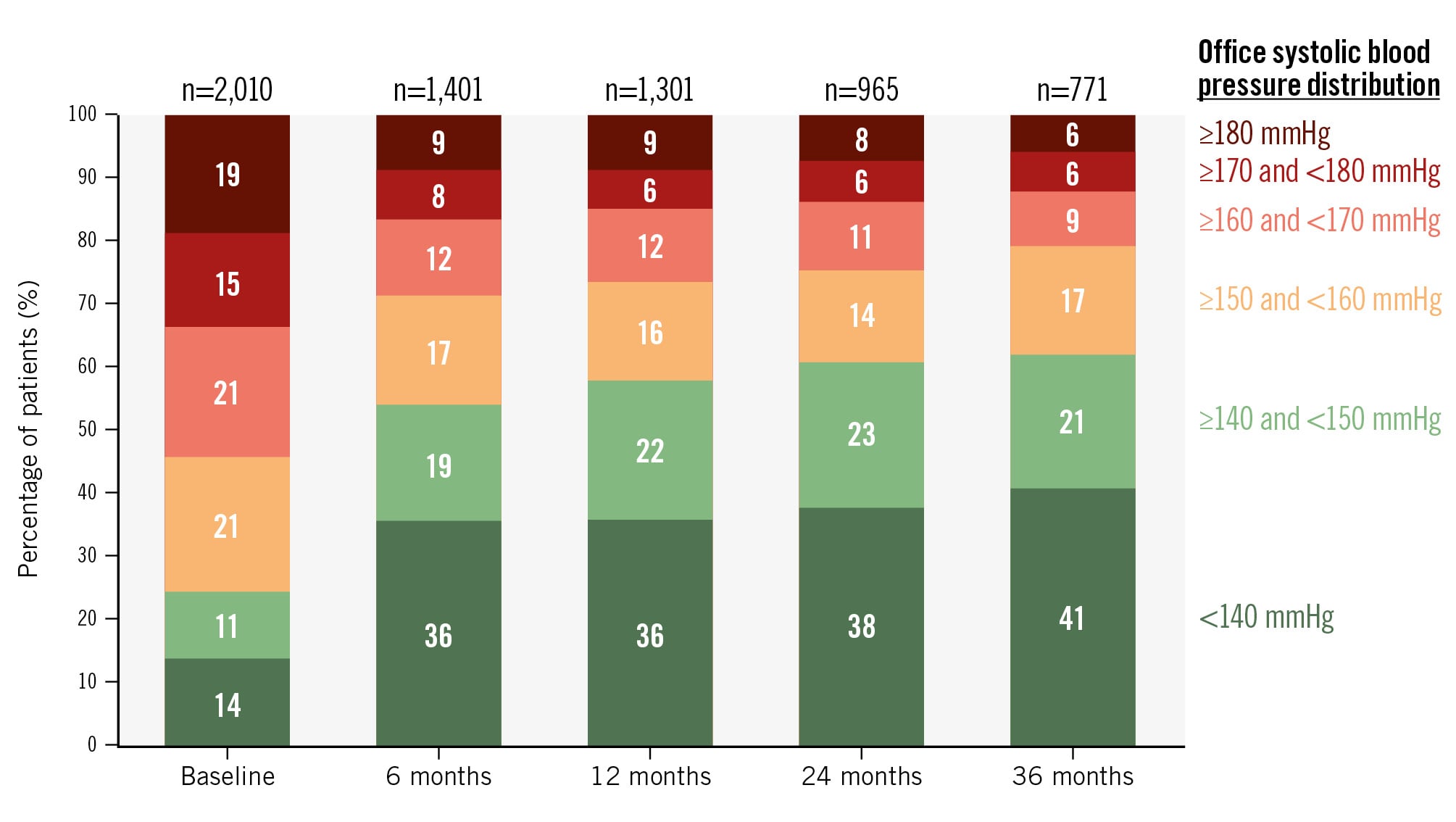
Figure 2. Distribution of office systolic BP reductions after RDN at 36 months. The proportion of patients in the indicated office systolic BP ranges from baseline to 36 months are plotted. BP: blood pressure; RDN: renal denervation
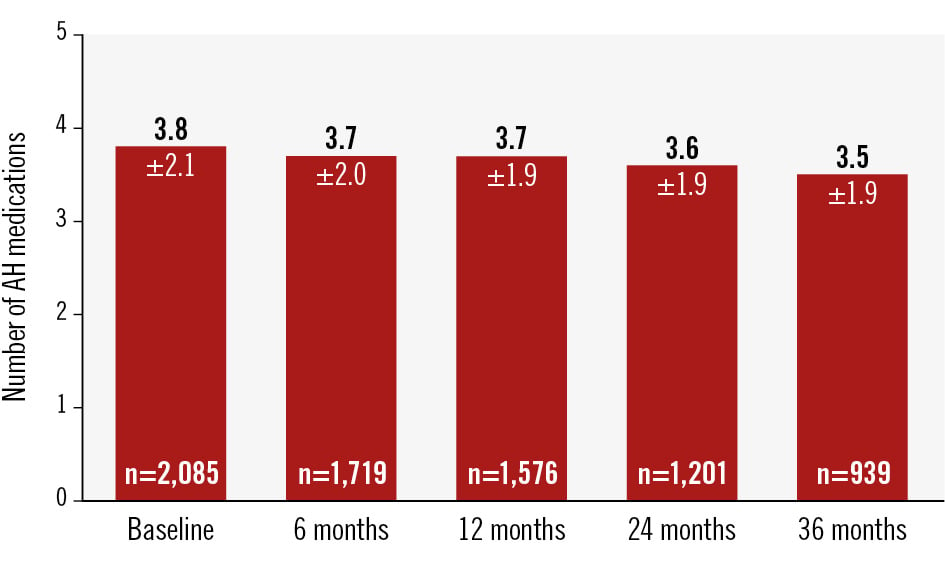
Figure 3. Antihypertensive medications among pooled Spyral patients through 36 months. The number of prescribed antihypertensive (AH) medications from baseline up to 36 months are plotted.
Proportion of patients experiencing a clinical benefit after RDN
Among the evaluable patients at 36 months (n=428) (Supplementary Table 2), 87.6% experienced either a 10 mmHg or greater reduction in office systolic BP, a 5 mmHg or greater reduction in 24 h ambulatory systolic BP, and/or the reduction of at least 1 AH medication (Figure 4). As a sensitivity analysis, we also calculated the proportion of patients who experienced a clinical benefit without any increase in either office or 24 h ambulatory BP (Supplementary Figure 4). The proportion of patients experiencing a clinical benefit by study is provided in Supplementary Table 3. The mean office and 24 h ambulatory systolic BP changes at 36 months in this cohort were –22.6±18.1 mmHg and –16.3±16.0 mmHg, respectively. The number of medications in this subgroup was 2.3±2.2 at baseline and 2.9±1.8 at 36 months.
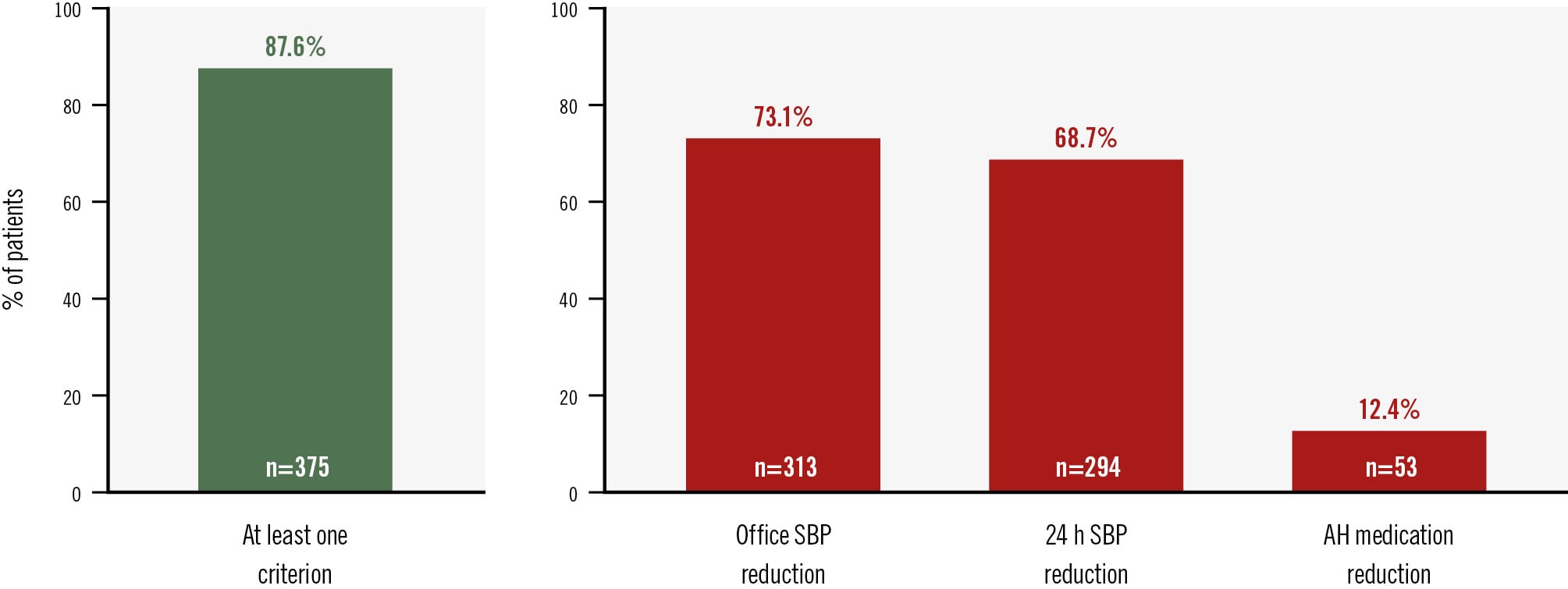
Figure 4. The proportion of patients experiencing a clinical benefit 36 months after RDN. The proportion of patients experiencing a clinical benefit (green) is broken down into its non-mutually exclusive components (red). AH: antihypertensive; RDN: renal denervation; SBP: systolic blood pressure
Clinical outcomes THROUGH 36 months
Safety events were uncommon through 36 months after RF-RDN (Supplementary Table 4). The rate of renal artery stenosis was 0.1% (1/1,000), with 1 patient identified as having renal artery stenosis greater than 70%. However, this patient declined confirmatory imaging of renal artery stenosis by angiography. No patient required renal artery reintervention or stent implantation through 36 months after treatment with the Spyral device. The rates of death, cardiovascular death, myocardial infarction, and stroke were 5.2%, 2.5%, 1.8%, and 4.5%, respectively. The rate of hospitalisation for hypertensive crisis was 2.2%. Among the patients who experienced a 10 mmHg or greater reduction in office systolic BP, a 5 mmHg or greater reduction in 24 h ambulatory systolic BP, or the reduction of at least 1 AH medication, the rates of death, cardiovascular death, myocardial infarction, stroke, and hospitalisation for hypertensive crisis were 0.0%, 0.0%, 1.1%, 1.1%, and 1.1%, respectively.
Discussion
This study pooled data from 2,137 patients treated with the Spyral device in the SPYRAL clinical programme. Through 36 months after RF-RDN, patients experienced statistically significant and clinically meaningful reductions in office and 24-hour ambulatory systolic and diastolic blood pressure. Overall, the rates of office and ambulatory BP control improved over time, highlighting the sustained efficacy of RDN. Adverse events were rare through long-term follow-up with few procedure-related complications.
Numerous single-arm and randomised controlled studies have demonstrated the sustained efficacy of RDN through 3 years of follow-up.1722 In the present study, the persistent BP reductions considerably exceeded the treatment effect of a single AH medication.23 The observation of continual BP lowering through long-term follow-up and in the absence of escalating medications is a consistent finding following RF-RDN.15 Although the biological mechanisms for this finding remain uncertain, attenuation of the neurohormonal system, vascular remodelling with reduced peripheral vascular resistance, and resetting baroreflex physiology have been hypothesised.
Measurement of BP is an established surrogate endpoint,24252627 with a 5 mmHg reduction in office systolic BP being associated with a 10% reduction in the risk of major adverse cardiovascular events.23 Among patients with all evaluable measures through 36 months, nearly 9 out of 10 experienced a clinical benefit after RDN, indicated by an office systolic BP reduction of at least 10 mmHg, a 24 h ambulatory systolic BP reduction of at least 5 mmHg, a reduction of at least 1 AH medication, or a combination thereof. In real terms, these results provide practical guidance for treating clinicians to inform late-term expectations as part of clinical decision-making with patients. Two recent linear regression models investigating the BP response in patients from the SPYRAL clinical programme, both of which included a subcohort of Spyral-treated patients, found that baseline BP was the only consistent patient characteristic associated with expected BP changes after RDN.1516 Similarly, BP response to pharmacotherapy is also dependent on the baseline or starting blood pressure.2829 Even in the absence of other identified variables predictive of a BP-lowering effect after RDN, it is reassuring that nearly 90% of patients experience some meaningful benefit.
It remains to be seen whether other patient or procedural characteristics might also be associated with BP response. However, individuals who remain hypertensive despite adherence to lifestyle modifications and prescribed AH medications should be prioritised for consideration for RDN. This is consistent with multiple recent hypertension guidelines.83031 Patients that should be especially considered for RDN are those taking multiple AH medications and those who wish to reduce their medication burden. Polypharmacy risks increased incidence of side effects, non-adherence, and medication intolerance.3233 By reducing the number of prescribed AH medications, patients may also have considerable improvements in their quality of life.34 The results herein, coupled with increased patient awareness of interventional treatment options, should serve to inform the shared decision-making process between physicians and their patients in shaping a personalised hypertension management plan.3536
Limitations
This study has several limitations. Patients’ data were pooled across 4 different studies with varying study designs, inclusion criteria (or lack thereof), and prescribed AH medication regimens (or lack of AH medications, in the instance of the OFF MED trial). Due to the heterogeneity of the pooled studies, results should be regarded as descriptive rather than confirmatory. In the two randomised controlled trials, after the primary endpoint was ascertained, treating clinicians were encouraged to lower patients’ BP if it remained uncontrolled, which necessarily increased patients’ medication burden. Due to the inclusion of patients from the GSR and FIH study, and because the majority of sham-control patients crossed over to undergo RDN after the primary endpoint, blood pressure reductions are not sham adjusted. Thus, the results presented for the long-term durability of the procedure do not include comparative data. Not all patients had continuous follow-up through 36 months, as some have not reached 36 months since the procedure. Patients from the GSR did not undergo systematic imaging of the renal arteries or adjudication at later timepoints. Therefore, late renal function complications may have been underreported.
Conclusions
In this large, pooled dataset of patients treated with the Symplicity Spyral RF-RDN catheter, there were statistically significant and clinically meaningful BP reductions through 36 months with few adverse events. Sensitivity analyses including a matched analysis and mixed model showed similar efficacy results. Additionally, rates of systolic blood pressure control improved over time. Moreover, nearly 9 out of 10 patients experienced a clinical benefit. These findings are consistent with the durable efficacy and safety of RF-RDN in hypertensive patients with a wide range of demographics.
Impact on daily practice
Renal denervation (RDN) is a guideline-recommended therapy for uncontrolled hypertension. In this study, 3-year blood pressure (BP) changes and the proportion of patients who experienced a clinical benefit after RDN using the Symplicity Spyral device were evaluated. BP reductions after RDN were significant and were sustained over the long term, with nearly 9 out of 10 patients experiencing a clinical benefit.
Acknowledgements
Benjamin Woods, PhD, of Medtronic provided editorial support under the direction of the first author, including the preparation of figures and tables, and editing of text. The executive committee designed the protocol and identified suitable clinical sites to conduct the study in collaboration with Medtronic. Medtronic was responsible for data collection, monitoring, and analysis. The article was written by the lead author with contributions from the co-authors. All authors have access to all data and were responsible for the decision to submit the manuscript for publication.
Conflict of interest statement
D.E. Kandzari receives institutional research/grant support from Biotronik, Boston Scientific, OrbusNeich, Teleflex, Medtronic, and Abbott; he also receives personal consulting honoraria from Boston Scientific, Medtronic, HyperQure, Cordis Corporation, and Brattea Medical. M. Böhm is supported by the Deutsche Forschungsgemeinshaft (SFB TTR219); and receives personal fees from Abbott, Amgen, AstraZeneca, Bayer, Boehringer Ingelheim, Cytokinetics, Edwards Lifesciences, Medtronic, Novartis, Recor Medical, Servier, and Vifor. R.E. Schmieder has received speaker and consulting honoraria from Medtronic, Recor Medical, Boston Scientific, and Ablative Solutions; and research grants have been given to his institution from Medtronic, Recor Medical, SoniVie/Boston Scientific, and Ablative Solutions. M.P. Schlaich has received support from the National Health and Medical Research Council Senior Research Fellowship; and has received consulting fees or travel and research support from Medtronic, Abbott, Novartis, Servier, Pfizer, and Boehringer Ingelheim. R.R. Townsend is a consultant for Medtronic, Axio, Regeneron, Bard, OBIO, Corcept, and AstraZeneca; and receives royalties from UpToDate. K. Kario receives research grants from A&D Company and Omron Healthcare; and receives honoraria from Medtronic, Otsuka Pharmaceutical, and Omron Healthcare. M. Gilbertson is an employee of Medtronic. F. Mahfoud has been supported by Deutsche Forschungsgemeinschaft (SFB TRR219, Project-ID 322900939), and Deutsche Herzstiftung; Saarland University has received scientific support from Ablative Solutions, Medtronic, and Recor Medical; until May 2024, he received speaker honoraria/consulting fees from Ablative Solutions, AstraZeneca, Inari, Medtronic, Merck, Novartis, Philips, and Recor Medical, all outside the submitted work. R. Whitbourn has no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.