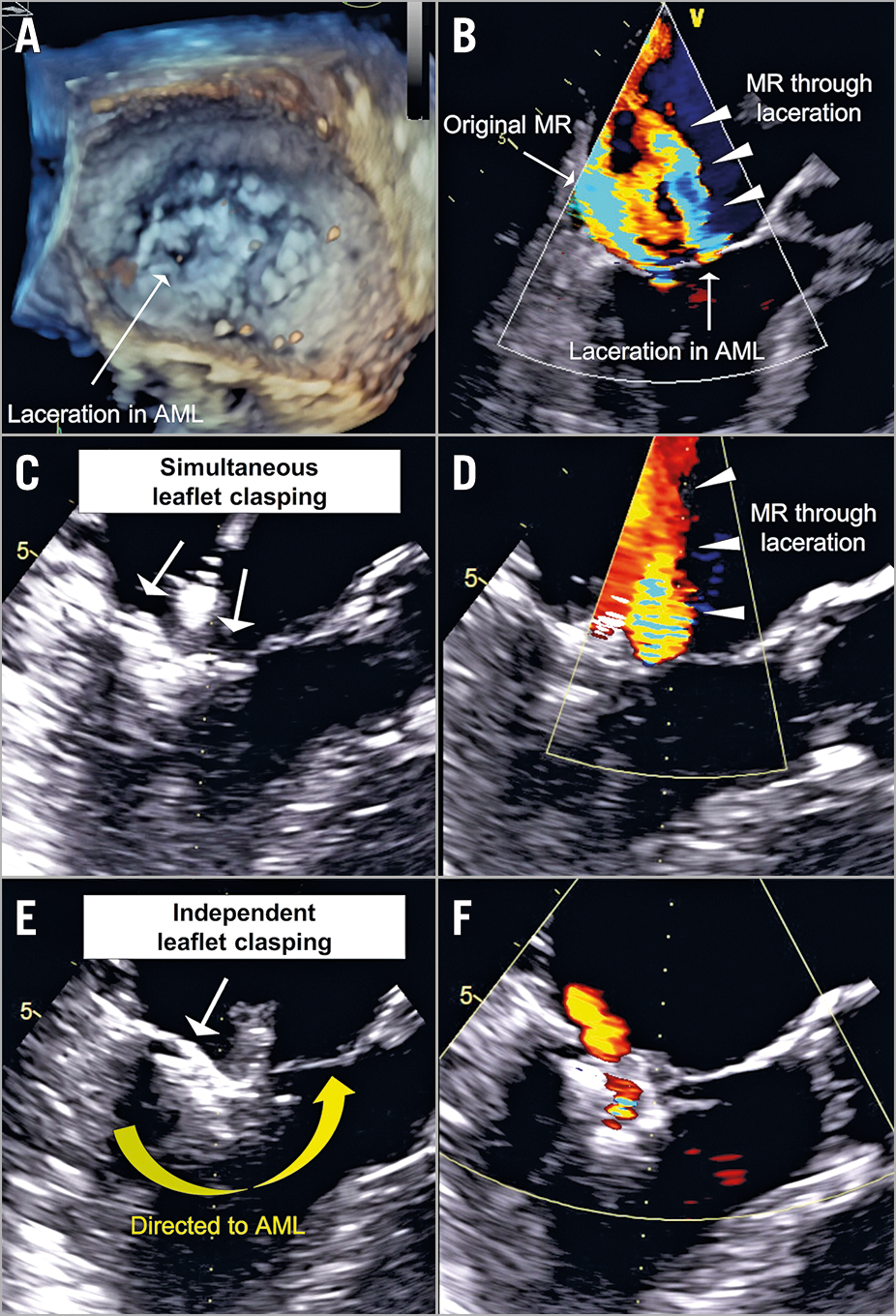
Figure 1. Independent clasping to capture a leaflet defect. A) Laceration in the medial half of the anterior mitral leaflet (arrow), caused by grasping with the MitraClip XTR device. B) Two jets of mitral regurgitation: one is due to leaflet tethering, the other (arrowheads) is through the iatrogenic laceration (arrow). C) Simultaneous clasping of the leaflets (arrows). D) Residual regurgitation (arrowheads) through the mitral leaflet laceration. E) The posterior leaflet was independently attached (arrow). Then, the PASCAL system was directed to the anterior leaflet to maximise leaflet insertion and cover the laceration (yellow arrow). F) No residual regurgitation through the iatrogenic laceration on the anterior leaflet.
An 84-year-old woman, presenting with dyspnoea (New York Heart Association Class III) and oedema, underwent an edge-to-edge mitral valve repair with the MitraClip® XTR system (Abbott Vascular, Santa Clara, CA, USA) for the treatment of severe functional mitral regurgitation (MR) (Moving image 1). After grasping the leaflets and closing the MitraClip, intraprocedural transoesophageal echocardiography detected a new substantial regurgitation through an iatrogenic laceration in the anterior leaflet that was believed to be caused by tension stress on the XTR device (Figure 1A, Figure 1B, Moving image 2, Moving image 3). Because the device’s arms could not reach far enough to cover the laceration in the several attempts that were made, the MitraClip was not implanted and the system was extracted.
Owing to the patient having a high surgical risk (STS-PROM score: 6.40%, EuroSCORE II: 7.82%), frailty, and unsuitable anatomy (small left ventricular outflow tract) for open heart or transcatheter mitral valve replacement, the Heart Team decided next to attempt edge-to-edge mitral valve repair with the PASCAL system (Edwards Lifesciences, Irvine, CA, USA). The PASCAL device was first placed in the original MR jet area, but the MR through the laceration remained (Figure 1C, Figure 1D, Moving image 4). Hence, to maximise leaflet insertion and cover the laceration, first, the posterior leaflet was independently attached and then the device was directed to the anterior leaflet, which was extensively captured including the leaflet defect (Figure 1E, Moving image 5). This led to good coverage of the laceration and a significant reduction in MR (Figure 1F, Moving image 6). At one-month follow-up, transthoracic echocardiography showed only trivial residual MR with a transmitral pressure gradient of 2.3 mmHg.
Edge-to-edge mitral valve repair is currently the most prevalent transcatheter technique for patients with severe MR. The PASCAL system offers an optional independent leaflet clasping, thereby allowing it to overcome challenging anatomies that might be inaccessible with the MitraClip system1. Furthermore, the unique design of the system (i.e., wide paddles, spacer, nitinol frame) enables preventing excess tension stress on leaflets. A multicentre study reported the procedural safety and efficacy of the PASCAL system, regardless of the anatomical complexity2. Therefore, staged independent clasping using the PASCAL device may be an efficient therapeutic option to overcome challenging MR pathologies, such as a leaflet laceration.
Acknowledgements
We wish to thank Dr Marcel Weber for supervising the manuscript and Figure, and Dr Meghan Campbell for proofreading the manuscript.
Conflict of interest statement
J.M. Sinning and G. Nickenig have received speaker honoraria and research grants from Medtronic, Boston Scientific, Edwards Lifesciences, and Abbott Vascular. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Baseline transoesophageal echocardiography showing severe functional mitral regurgitation (proximal isovelocity surface area, 0.8 cm; effective regurgitation orifice area, 0.32 cm²; regurgitant volume, 45 ml; anterior-posterior annulus diameter, 36 mm).
Moving image 2. During the initial procedure with MitraClip, intraprocedural transoesophageal echocardiography detected a new substantial regurgitation through an iatrogenic laceration in the anterior leaflet, approximately 5 minutes after grasping the leaflets.
Moving image 3. Three-dimensional transoesophageal echocardiography showing a laceration in the medial half of the anterior mitral leaflet.
Moving image 4. The PASCAL device was first placed in the original mitral regurgitation jet area; however, the regurgitation through the laceration remained.
Moving image 5. The posterior leaflet was independently attached, then the PASCAL system was directed to the anterior leaflet to maximise leaflet insertion and cover the laceration.
Moving image 6. No residual regurgitation through the iatrogenic laceration on the anterior leaflet.