A 79-year-old male with severe primary MR, due to flail of the lateral (P1) scallop with a commissural jet (Figure 1A), underwent attempted transcatheter edge-to-edge repair (TEER) with the MitraClip system (Abbott). The transseptal puncture was performed in the mid-position in the bicaval view and in the mid-posterior position in the short-axis view (Figure 1B), with a transseptal puncture height of 4 cm (Figure 1C). The MitraClip system was noted to have an anterior-to-posterior trajectory (aorta hugger) (Figure 1D, Figure 1E). Correcting the aorta hugger trajectory − using the “+” knob on the steerable guide catheter to move the guide posteriorly (away from the aorta) and the “M” knob to move the MitraClip system medially − resulted in loss of height of the MitraClip system from the mitral valve. The loss of height from the mitral valve could not be adequately corrected with posterior steering of the guide catheter and addition of the “A” knob to move the MitraClip system anteriorly and laterally to the mitral plane. A repeat transseptal puncture was performed with a transseptal height of 5.8 cm (Figure 1F). While advancing the MitraClip steerable guide across the interatrial septum through the 2nd transseptal puncture, a septal tear was noted, extending to the 1st transseptal puncture, thereby again resulting in loss of height from the mitral valve. Despite advanced steering with the A knob and M knob, as well as posterior steering of the guide catheter, an adequate height of the MitraClip system from the mitral valve could not be achieved and the aorta hugger trajectory could not be corrected. The procedure was aborted.
Following the U.S. Food and Drug Administration (FDA) approval of the PASCAL Precision system (Edwards Lifesciences) 2 months after the aborted MitraClip procedure, the patient was brought back to the catheterisation laboratory for another attempt at TEER with the PASCAL device. The left atrium was accessed via the right femoral venous approach through the tear in the interatrial septum (Figure 1G), which occurred during the MitraClip procedure, with a transseptal height of 4 cm. An aorta hugger trajectory was again noted when the PASCAL implant system was steered towards the mitral valve (Figure 1H); this was corrected successfully (Figure 1I) by adding flexion to the guide sheath (Figure 1J). The optimal height of the PASCAL system from the mitral valve was achieved by turning the guide sheath clockwise while the PASCAL implant system was turned counterclockwise (Figure 1K-Figure 1M). Once optimal position, trajectory, height, and orientation (Figure 1N) of the PASCAL implant system were achieved, successful TEER of the lateral commissure was performed with the PASCAL Ace implant (Edwards Lifesciences) (Figure 1O), resulting in a reduction to trivial MR (Figure 1P, Figure 1Q).
This is the first report of a clinical scenario where the results with the PASCAL system may be more favourable when compared with the MitraClip system. TEER for lateral commissural P1 flail was unsuccessful with the MitraClip system due to the failure to correct the aorta hugger trajectory without losing height from the mitral valve. Successful TEER was performed with the PASCAL system in the same patient using vascular access from the same side, through the same transseptal puncture, by the same operator and imager. For patients in whom an aorta hugger trajectory cannot be corrected successfully with the MitraClip system, the PASCAL device may offer another treatment option. As clinical experience with the PASCAL device grows, there may also be clinical scenarios where the MitraClip device may be more suitable. The availability of two different TEER technologies will expand the patient population that are eligible for transcatheter mitral valve repair.
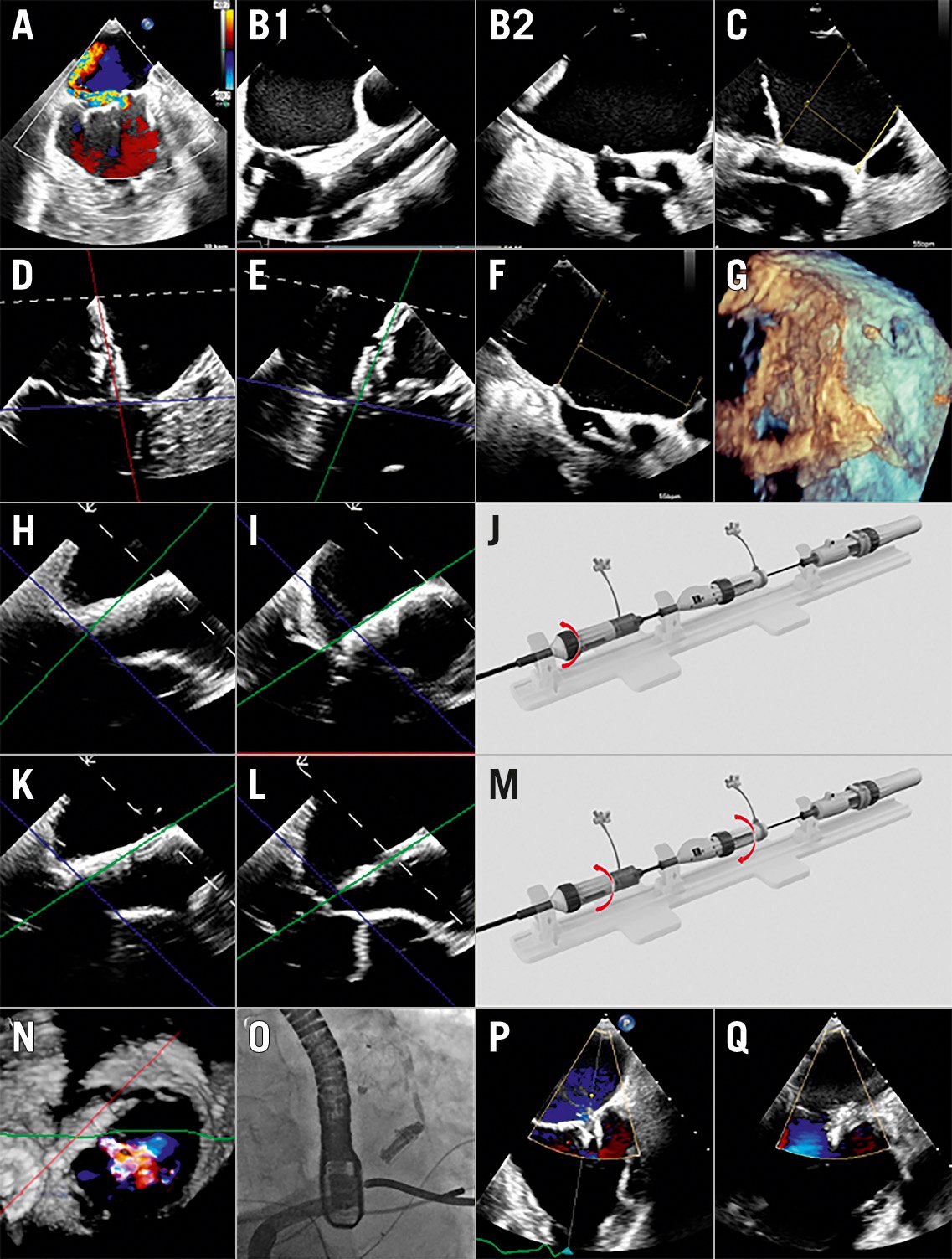
Figure 1. Transcatheter mitral valve edge-to-edge repair, unsuccessful with the MitraClip device, but successful with the PASCAL device. A) Severe primary mitral regurgitation due to flail of the lateral scallop. B) Transseptal puncture was performed in the mid-position in the bicaval view (B1) and in the mid-posterior position in the short-axis view (B2). C) Transseptal height of 4 cm from the mitral valve. D, E) Bicommissural view (D) and grasping view (E) demonstrating lack of adequate height of the MitraClip system to correct the anterior-to-posterior (aorta hugger) trajectory. F) Repeat transseptal puncture performed with a transseptal height of 5.8 cm. G) The septal tear which occurred during the MitraClip procedure was used for transseptal access for the PASCAL device. H-J) In the grasping view on transoesophageal echocardiogram (TOE), the aorta hugger trajectory (H) of the PASCAL implant system was successfully corrected (I) by adding flexion to the PASCAL guide sheath (J). K-M) In the grasping view on TOE, additional height of the PASCAL implant system was achieved (K, L) by clockwise rotation of the guide sheath followed by counterclockwise rotation of the PASCAL implant system (M). N) Optimal orientation of the PASCAL Ace implant. O-Q) Successful transcatheter mitral valve edge-to-edge repair performed with the PASCAL Ace implant O) with no significant residual mitral regurgitation (P, Q).
Conflict of interest statement
T. Chakravarty is aconsultant for Edwards Lifesciences, Medtronic, Abbott, and Boston Scientific. M. Makar is aconsultant for Abbott. R. Makkar is aconsultant for Edwards Lifesciences, Medtronic, Abbott, and Boston Scientific. The other authors have no conflicts of interest to declare.