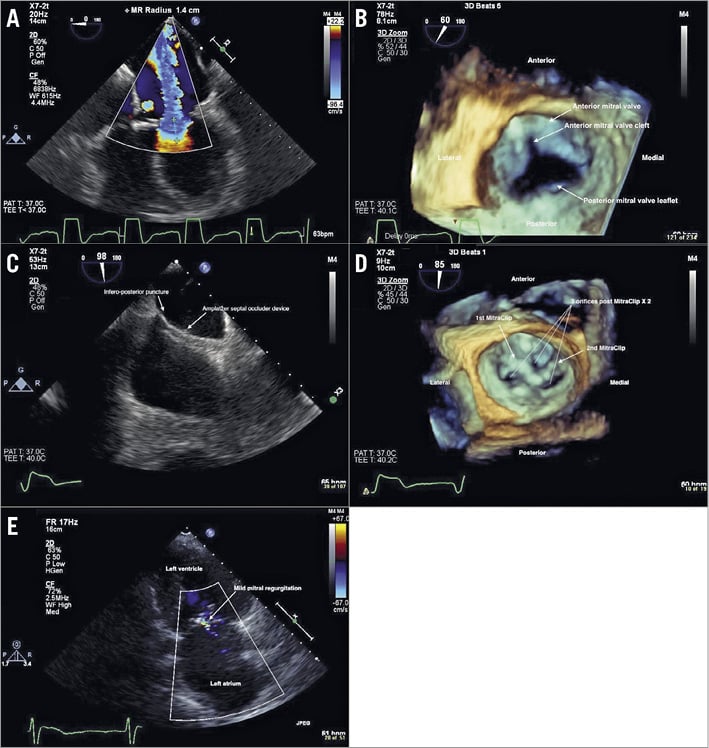
Figure 1. Illustration of the MitraClip procedure. A) Two-dimensional transoesophageal echocardiogram (2D TEE) four-chamber mid-oesophageal view showing large severe central mitral regurgitation (MR) jet. B) 3D TEE showing cleft in the mid anterior mitral valve leaflet (white arrow). C) 2D TEE mid-oesophageal bicaval view showing AMPLATZER Septal Occluder device and inferior-posterior puncture of the interatrial septum. D) 3D TEE showing two MitraClips post deployment in a “V” configuration. E) 2D transthoracic echocardiogram two-chamber view showing mild MR at one-month follow-up.
Mitral regurgitation (MR) is the second most common valvulopathy after aortic stenosis. Primary MR is a disorder of leaflet abnormality such as myxomatous degeneration, whereas secondary MR is a result of left ventricular remodelling causing abnormal leaflet coaptation. Cleft mitral valve leaflet is the most common cause of congenital MR, and surgical correction is the mainstay of treatment. Willemsen et al previously described the application of a MitraClip device in a 51-year-old male patient with severe MR and dilated cardiomyopathy who was discovered with posterior leaflet cleft during the procedure as a cause of the MR1. Here, we describe a challenging case of MitraClip intervention in a patient who was surgically repaired for the partial congenital atrioventricular (AV) canal defect and now presenting with symptomatic severe MR due to residual mitral valve cleft.
A 76-year-old female with a congenital AV septal defect and repair presented with NYHA Class III progressive dyspnoea on exertion and fatigue for six months. She had a history of congenital partial AV canal defect and mitral cleft for which she had received mitral valve (MV) repair and an atrial septal defect (ASD) repair with a pericardial patch in 1994. Due to the left to right shunt through the pericardial patch, she subsequently had an AMPLATZER™ Septal Occluder (ASO) device (St. Jude Medical, St. Paul, MN, USA) placed in 2007. A transthoracic echocardiogram showed an ejection fraction of 50-55% and severe mitral regurgitation (MR). A transoesophageal echocardiogram (TEE) showed severe MR (Figure 1A), and the ASO device. The three-dimensional TEE (3D TEE) showed a cleft in the MV A2 leaflet (Figure 1B, Moving image 1). Due to the prohibitive surgical risk and complex anatomy for the redo MV surgery, she was referred for MitraClip® (Abbott Vascular, Santa Clara, CA, USA) implantation.
The ideal approach for the transseptal puncture site in a MitraClip procedure is the superior and posterior aspect in the interatrial septum (IAS)2. However, due to the prior pericardial patch repair of the ASD and subsequent ASO device placement, the transseptal puncture was performed in the inferior and posterior aspect of the IAS (Figure 1C). This puncture location provided an appropriate height above the mitral annulus. Next, the MitraClip guide catheter was inserted into the left atrium and manoeuvred close to the MV. Initially, a MitraClip was deployed in a lateral position at the A1-P1 scallop, but there appeared to be moderate to severe MR still with a wide-open orifice (Moving image 2). The usual approach to implant a second MitraClip in cases of residual MR should be as parallel as possible to the first MitraClip2. However, due to the A2 cleft, we decided to place the second MitraClip at a slight angulation to the first MitraClip at the A3-P2 scallop in a “V” configuration with three corresponding openings (Figure 1D, Moving image 3). This resulted in a reduction in MR to 1+ (Moving image 4, Moving image 5) and the mean gradient across the mitral valve was 5 mmHg. There were no procedure-related complications. The patient was discharged on the following day. At the one-month follow-up visit the patient reported improvement in symptoms. The echocardiogram at one-month follow-up was consistent with mild MR (Figure 1E).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. 3D TEE left atrial view showing mitral valve A2 cleft.
Moving image 2. 3D TEE left atrial view showing mitral valve A2 cleft medial to the 1st MitraClip.
Moving image 3. 3D TEE left atrial view showing two MitraClips in a “V” configuration with three openings.
Moving image 4. 3D TEE colour left atrial view showing mild MR post procedure.
Moving image 5. 2D TEE mid-oesophageal two-chamber view showing mild MR post procedure.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. 3D TEE left atrial view showing mitral valve A2 cleft.
Moving image 2. 3D TEE left atrial view showing mitral valve A2 cleft medial to the 1st MitraClip.
Moving image 3. 3D TEE left atrial view showing two MitraClips in a “V” configuration with three openings.
Moving image 4. 3D TEE colour left atrial view showing mild MR post procedure.
Moving image 5. 2D TEE mid-oesophageal two-chamber view showing mild MR post procedure.