A 41-year-old woman developed acute myocardial infarction after salbuterol abuse. Coronary angiography showed narrowing of the left main (LM) and of the proximal left anterior descending artery (LAD), and a hazy subocclusion of the mid LAD. Manual and rheolytic thrombectomy were performed without retrieving thrombus and improving flow. Due to haemodynamic instability, we deployed a drug-eluting stent (DES) and performed a first optical coherence tomography (OCT) scan, demonstrating severe spasm of the distal LM, and an extensive intramural haematoma of the proximal LAD, possibly squeezed proximally and distally by stent implantation (Figure 1, top row). We hypothesised intramural haematoma since no clear intimal tear was visualised. We deployed another DES distally overlapping the first, to prevent extension of the dissection. A second OCT showed worsening of the distal LM spasm (with a focal dissection) and of the proximal LAD luminal narrowing, and partial malapposition of the distal DES (Figure 1, middle row). We stopped as the patient was stable and we feared potential complications of further interventions. Ten days later, OCT showed resolution of spasm and dissection in the LM, partial resorption of the haematoma in the proximal LAD, and 360° malapposition of the distal stent (Figure 1, bottom row). We successfully post-dilated the DES, but OCT showed recurrence of severe spasm in the proximal LAD, with “blebbing” of the intima and/or adherent microthrombi. Coronary angiography after nine months showed normal LM and LAD appearance (Appendix).
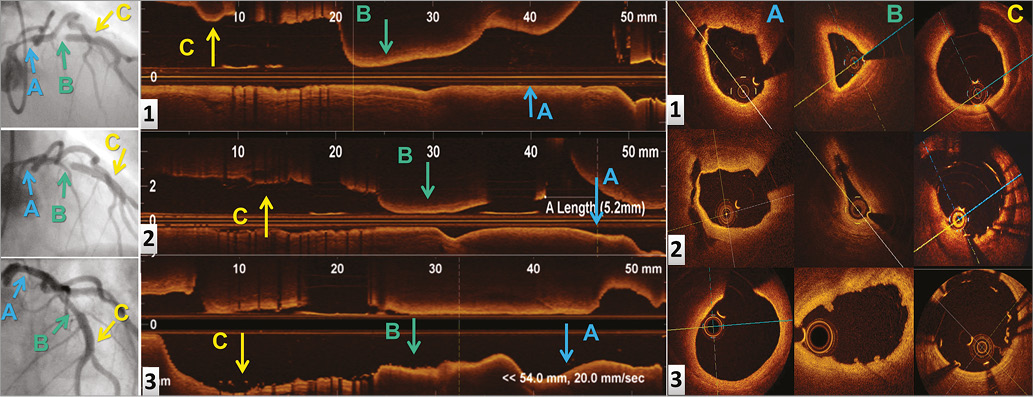
Figure 1. Imaging of the left coronary artery. Angiographic (left column) and OCT images in longitudinal (mid column) and cross-sectional view (right column) of the distal LM (A), proximal LAD (B) and mid LAD (C), after deployment of the first (1) and second (2) stent during the index PCI, and 10 days later (3).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Appendix. Spasm and intramural haematoma of the left main
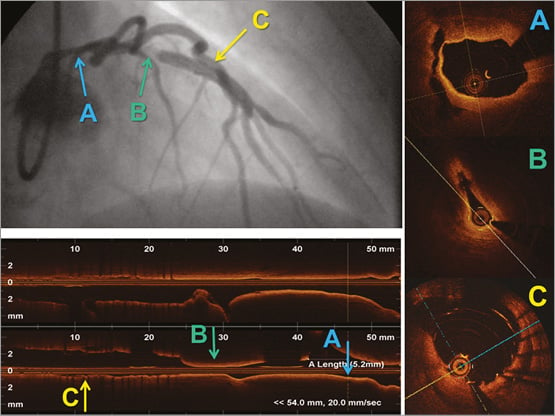
A 41-year-old woman, with no cardiovascular risk factors but with a history of recent abuse of salbuterol because of bronchial asthma, was admitted to our institution for acute myocardial infarction. Coronary angiography showed a normal right coronary artery, diffuse narrowing of the left main (LM) and of the proximal left anterior descending artery (LAD), and subocclusion of the mid LAD with a hazy filling defect, compatible with thrombus, coronary dissection, intramural haematoma, severe spasm, or a combination thereof (Moving image 1, Moving image 2). Firstly, we administered intracoronary nitrates and verapamil, without effect. We subsequently performed manual and rheolytic thrombectomy, without retrieving thrombus and improving flow. As the patient was haemodynamically unstable, we decided to deploy a 3.5×12 mm drug-eluting stent (DES) at the site of subocclusion (Moving image 3). We then performed a first optical coherence tomography (OCT) scan (Moving image 4), which demonstrated severe spasm of the distal LM, with a focal detachment of the intima from the media in an area not touched by the guiding catheter (Appendix Figure 1, label A), severe spasm and an extensive intramural haematoma of the proximal LAD (Appendix Figure 1, label B), good expansion and apposition of the DES, with a small closed dissection at its distal margin (Appendix Figure 1, label C). The deployment of the DES probably squeezed the haematoma both proximally, as the site of tightest stenosis shifted proximally (Appendix Figure 2), and distally, causing the mild stenosis at the distal margin of the stent. We hypothesised the presence of intramural haematoma in the LAD since no clear intimal tear was visualised; we believe that spasm was also present, as the luminal diameter of the distal LM and proximal LAD progressively shrank during the procedure. Such relevant and dynamic changes can be explained by spasm, presumably induced by contrast injection and vessel instrumentation.
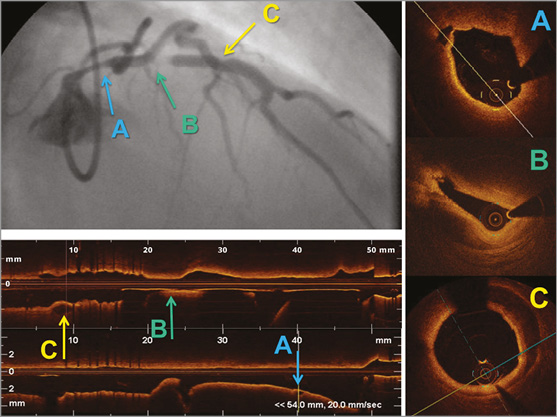
Appendix Figure 1. Imaging of the left anterior descending artery after deployment of the first stent. Top left: angiographic appearance of the left coronary artery after deployment of the first stent during the index procedure, showing severe narrowing of the distal LM (A), subocclusion of the LAD proximal to the stent (B), and a small “bump” at the distal margin of the stent (C). Bottom left: subsequent OCT scan of the left coronary with longitudinal and (right) cross-sectional images, showing severe spasm of the distal LM, with a focal detachment of the intima from the media (A), severe spasm and an extensive intramural haematoma of the proximal LAD (B), a small closed dissection at the distal margin of the stent (C).
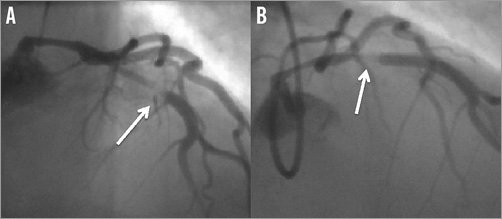
Appendix Figure 2. Angiography before and after deployment of the first stent. Angiographic appearance of the left coronary artery before (A) and after (B) deployment of the first stent during the index procedure, demonstrating a proximal shift of the site of worse luminal narrowing of the proximal LAD (arrow), probably caused by squeezing of the intramural haematoma during stent deployment.
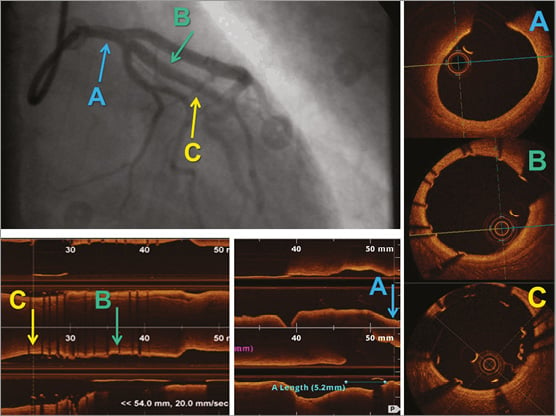
We then deployed a second DES (3.5×8 mm) distally overlapping the first, to seal the dissection (Moving image 5). A second OCT run (Moving image 6) showed worsening of the spasm and of the dissection of the distal LM (Appendix Figure 3, label A), worsening of the stenosis of the proximal LAD (Appendix Figure 3, label B), and malapposition of the distal DES over a 230° arc in the cross-sectional view (Appendix Figure 3, label C). As the patient was stable and we feared the potential complications of further interventions, we stopped the procedure and continued i.v. nitrates and verapamil for 24 hours.
Appendix Figure 3. Imaging of the left anterior descending artery after deployment of the second stent. Top left: angiographic appearance of the left coronary artery after deployment of the second stent, showing worsening of the narrowing of the LM (A) and proximal LAD (B), and good result of the deployment of the second stent (C). Bottom left: subsequent OCT scan with longitudinal and (right) cross-sectional images, showing worsening of the spasm and of the dissection of the distal LM (A), worsening of the stenosis of the proximal LAD (B), and malapposition of the distal DES over a 230° arc (C).
Ten days later coronary angiography was repeated, showing a normal appearance of the LM and LAD (Moving image 7). A first OCT scan (Moving image 8) showed resolution of the LM spasm and distal dissection (Appendix Figure 4, label A), partial resorption of the haematoma in the proximal LAD, good apposition of the proximal stent (Appendix Figure 4, label B), and severe malappostion of the distal stent, floating in the lumen over a 360° arc (Appendix Figure 4, label C), probably due to the resolution of spasm. Therefore we post-dilated both DES with a non-compliant 4.0 mm balloon (Moving image 9). A second OCT scan (Moving image 10) showed recurrence of severe spasm in the proximal LAD (Appendix Figure 5, label A), with “blebbing” of the intima and/or adherent microthrombi (Appendix Figure 5, label B), improved apposition of the distal DES, and a new interruption in the intimal layer within the proximal DES over a 50° angle for 3 mm of length (Appendix Figure 5, label C). The patient remained clinically stable and was discharged on oral nitrates and verapamil.
Appendix Figure 4. Initial imaging of the left anterior descending artery 10 days after the index PCI. Top left: angiographic appearance of the left coronary artery 10 days after the index procedure, showing a normal appearance of the LM (A), proximal LAD (B), and of the two stents (C). Bottom left: subsequent OCT scan with longitudinal and (right) cross-sectional images, showing resolution of the LM spasm and distal dissection (A), good apposition of the proximal stent (B), and severe malappostion of the distal stent (C).
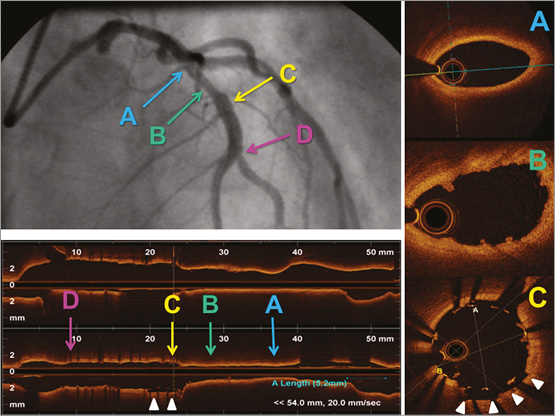
Appendix Figure 5. Final imaging of the left anterior descending artery ten days after the index PCI. Top left: angiographic appearance of the left coronary artery after aggressive post-dilatation of the stents. Bottom left: subsequent OCT scan with longitudinal and (right) cross-sectional images, showing recurrence of spasm in the proximal LAD (A), with “blebbing” of the intima and/or adherent microthrombi (B), a new interruption in the intimal layer within the proximal DES for a 50° angle for 3 mm of length (C, arrowheads), and improved apposition of the distal stent (D).
After nine months, the patient developed atypical chest pain and underwent coronary angiography, showing a normal LM and proximal LAD and an excellent result of DES implantation in mid LAD (Moving image 11, Moving image 12).
In our opinion, this patient suffered a spontaneous intramural haematoma of the LAD, with superimposed severe spasm, probably enhanced by salbuterol and vessel instrumentation. The dynamic changes in lumen diameter and morphology documented by serial OCT reflect a functional phenomenon, coronary spasm, presumably leading to focal detachment of the intima from the media in the LM, and to endothelial “blebbing” in the LAD. A less severe, “wavy” appearance of the intimal layer at OCT during coronary spasm has already been described in patients with coronary spastic angina. Coronary spasm is a common component of the pathophysiology of STEMI, and in our patient it could have been magnified by salbuterol abuse.
Online data supplement
Moving image 1. First cine loop of the left coronary artery during the index procedure, showing narrowing of the proximal LAD and subocclusion of the mid LAD.
Moving image 2. Second cine loop of the left coronary artery during the index procedure, showing narrowing of the LM and proximal LAD and a hazy subocclusion of the mid LAD.
Moving image 3. Cine loop after deployment of the first stent in mid LAD, showing worsening of the narrowing of the LM and proximal LAD.
Moving image 4. OCT scan of the left coronary artery after first stent deployment, showing severe spasm of the distal LM, with a focal detachment of the intima from the media, extensive intramural haematoma and severe spasm of the proximal LAD, and a closed dissection at the distal margin of the stent.
Moving image 5. Final angiography of the index procedure, after deployment of a second stent overlapping distal to the first, showing persistent severe narrowing of the LM and proximal LAD.
Moving image 6. Final OCT scan during the index procedure, showing worsening of the spasm and focal dissection of the distal LM, extensive intramural haematoma and severe spasm of the proximal LAD, and malapposition of the distal stent along a 230° arc.
Moving image 7. First cine loop of the left coronary artery 10 days after the index procedure, showing an apparently normal LM and proximal LAD and good angiographic result of stent implantation in mid LAD.
Moving image 8. First OCT scan of the left coronary artery 10 days after the index procedure, showing resolution of spasm and dissection in the distal LM, partial resorption of the haematoma in the proximal LAD, and 360° malapposition of the distal stent, probably due to the resolution of spasm.
Moving image 9. Final angiographic result after post-dilatation of the stents, showing recurrent spasm of the LM and proximal LAD.
Moving image 10. OCT scan after post-dilatation of the distal stent, showing recurrence of severe spasm in the proximal LAD, with “blebbing” of the intima and/or adherent microthrombi, apposition of the distal DES, and a new interruption in the intimal layer within the proximal DES for a 50° angle for 3 mm of length, possibly caused by aggressive post-dilatation.
Moving image 11 and Moving image 12. Angiographies of the left coronary artery nine months after the index procedure, showing a normal appearance of the LM and proximal LAD and good result of DES implantation in mid LAD.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. First cine loop of the left coronary artery during the index procedure, showing narrowing of the proximal LAD and subocclusion of the mid LAD.
Moving image 2. Second cine loop of the left coronary artery during the index procedure, showing narrowing of the LM and proximal LAD and a hazy subocclusion of the mid LAD.
Moving image 3. Cine loop after deployment of the first stent in mid LAD, showing worsening of the narrowing of the LM and proximal LAD.
Moving image 4. OCT scan of the left coronary artery after first stent deployment, showing severe spasm of the distal LM, with a focal detachment of the intima from the media, extensive intramural haematoma and severe spasm of the proximal LAD, and a closed dissection at the distal margin of the stent.
Moving image 5. Final angiography of the index procedure, after deployment of a second stent overlapping distal to the first, showing persistent severe narrowing of the LM and proximal LAD.
Moving image 6. Final OCT scan during the index procedure, showing worsening of the spasm and focal dissection of the distal LM, extensive intramural haematoma and severe spasm of the proximal LAD, and malapposition of the distal stent along a 230° arc.
Moving image 7. First cine loop of the left coronary artery 10 days after the index procedure, showing an apparently normal LM and proximal LAD and good angiographic result of stent implantation in mid LAD.
Moving image 8. First OCT scan of the left coronary artery 10 days after the index procedure, showing resolution of spasm and dissection in the distal LM, partial resorption of the haematoma in the proximal LAD, and 360° malapposition of the distal stent, probably due to the resolution of spasm.
Moving image 9. Final angiographic result after post-dilatation of the stents, showing recurrent spasm of the LM and proximal LAD.
Moving image 10. OCT scan after post-dilatation of the distal stent, showing recurrence of severe spasm in the proximal LAD, with blebbing of the intima and/or adherent microthrombi, apposition of the distal DES, and a new interruption in the intimal layer within the proximal DES for a 50° angle for 3 mm of length, possibly caused by aggressive post-dilatation.
Moving image 11. Angiographies of the left coronary artery nine months after the index procedure, showing a normal appearance of the LM and proximal LAD and good result of DES implantation in mid LAD.
Moving image 12. Angiographies of the left coronary artery nine months after the index procedure, showing a normal appearance of the LM and proximal LAD and good result of DES implantation in mid LAD.