Abstract
Aims: The aim of this study was to assess the efficacy of the mother and child technique using a 4 Fr inner catheter in coronary angioplasty following the failure of conventional techniques.
Methods and results: We identified cases in which a 4 Fr inner catheter had been used to facilitate stent delivery following the failure of conventional techniques. Stent delivery using a 4 Fr inner catheter was performed in 30 cases and was successful in 29 cases. Nineteen cases for RCA, six cases for LAD and five cases for LCx were examined. Direct engagement of a 4 Fr inner catheter was accomplished in eight cases. In the remaining patients, deep engagement of a 4 Fr inner catheter was accomplished with the anchor technique and/or distal balloon deflation technique. Proximal stent delivery followed by distal stent deployment was performed in seven cases by using the distal balloon deflation technique in multiple stent deployment. There were no complications related to deep intubation of a 4 Fr inner catheter.
Conclusions: The use of a 4 Fr inner catheter is safe and highly effective for aiding stent delivery. The anchor technique and/or distal balloon deflation technique could be required for deep engagement of a 4 Fr inner catheter.
Introduction
A previous report showed that nearly 5% of lesions could not be successfully treated with drug-eluting stents (DES)1. When a stent fails to advance because of severe tortuosity and/or calcification of the proximal section, it is imperative to assess the stability of the guide position, the stiffness of the wire, the calcification of the vessel and the flexibility of the stent. In clinical practice, many techniques for stent delivery have been developed for difficult situations2-4. Of these techniques, the inner catheter is particularly helpful if increased back-up force is needed during the procedure when the wire has already been inserted with difficulty through a guide catheter of conventional length. The principle of the inner catheter is to combine the advantages afforded by the passive support of a large mother guide catheter with the ability to insert further a smaller inner catheter within the target vessel, without damaging the arterial segment proximal to the lesion5-8. Recently, a 4 Fr inner catheter has become available in daily practice9,10. Compared with a 5 Fr inner catheter, a 4 Fr inner catheter can make the catheter more deliverable and potentially reduce the possibility for complications such as vessel injury. However, a limited back-up force with a 4 Fr inner catheter can be accommodated10,11. Therefore, the present study examined the efficacy of a 4 Fr inner catheter for a distal stent delivery device in daily practice.
Methods
We analysed 30 consecutive cases in which a 4 Fr inner catheter had been used as a stent delivery device following initial failure using conventional techniques at the National Hospital Organization Disaster Medical Center, Tokyo, Japan, between October 2009 and March 2011. A 4 Fr inner catheter system involves insertion of a flexible tipped extra length 120 cm 4 Fr inner catheter (Kiwami; Terumo Corp., Tokyo, Japan) or a 122 cm 4 Fr inner catheter (i-Works; Medikit Co., Ltd., Tokyo, Japan) through a standard 100 cm conventional mother guide catheter. The primary endpoint of this study was successful implantation of the stent. There was no significant difference between the two inner catheters in terms of catheter profile. Procedural factors related to success and failure were determined, and complications caused by the device were recorded.
Engagement of 4 Fr inner catheter
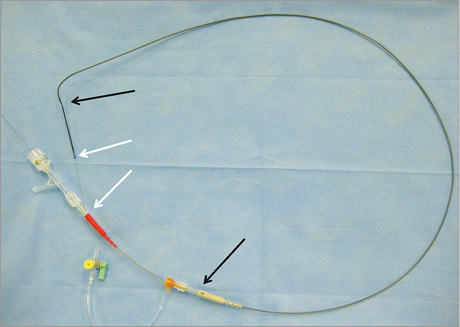
After the failure of stent delivery using the conventional technique, the Y-connector was disconnected from the guide catheter and a small haemostatic valve was connected. Then a 4 Fr inner catheter was passed through the mother guide catheter along the guidewire. The Y-connector was re-attached to the end of a 4 Fr inner catheter and the interventional procedure was performed in the usual manner (Figure 1, Online Figure 1).
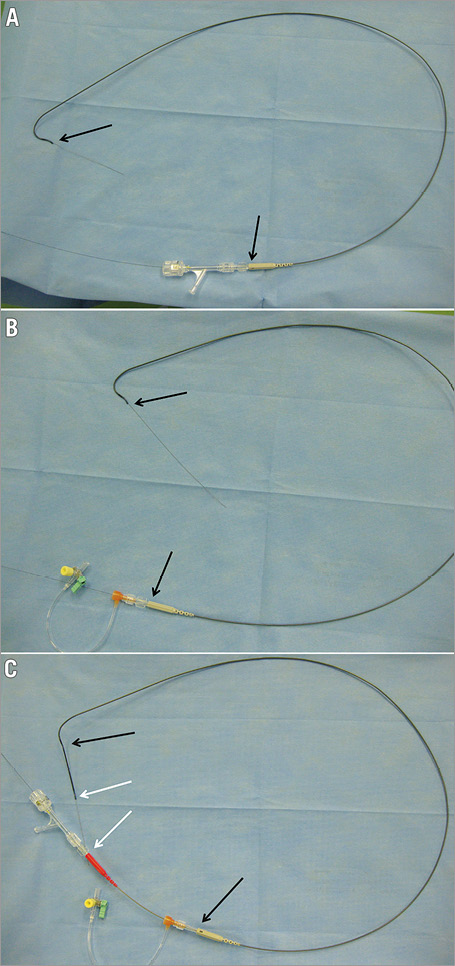
Figure 1. A 4 Fr inner catheter within a 5 Fr mother guide catheter connected with a Y-connector. A) A 5 Fr mother guide catheter was connected with a Y-connector. B) After the Y-connector was disconnected, a small haemostatic valve was re-attached. C) A 4 Fr inner catheter was passed through a mother guide catheter along the guidewire. Then the Y-connector was re-attached to the end of a 4 Fr inner catheter. Black arrows indicate the position of the 5 Fr mother guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
DIRECT ENGAGEMENT
A 4 Fr inner catheter was advanced into the vessel over either a coronary wire, or a wire and a balloon catheter with the balloon uninflated in the distal vessel. After the failure of stent delivery with direct engagement of a 4 Fr inner catheter, the anchor technique and distal balloon deflation technique were employed.
ANCHOR TECHNIQUE
At first, the balloon is placed at the distal culprit lesion. Then the balloon is inflated at 4 to 6 atm to insert a 4 Fr inner catheter slowly. By using the anchor technique between a balloon and a 4 Fr inner catheter, deep intubation of a 4 Fr inner catheter can be accomplished. The final position of a 4 Fr inner catheter is proximal to the inflated balloon.
DISTAL BALLOON DEFLATION TECHNIQUE
First, a balloon is placed at the distal culprit lesion and a 4 Fr inner catheter is also placed at the proximal lesion. Just after the deflation of the balloon, a 4 Fr inner catheter can be passed beyond the deflated balloon. The final position of a 4 Fr inner catheter is distal to the inflated balloon12.
Results
A total of 30 consecutive cases involving the use of a 4 Fr inner catheter to aid distal stent delivery where conventional techniques had failed were performed over a period of 18 months (total cases during study: 628 cases).
PATIENTS’ CHARACTERISTICS (Table 1)
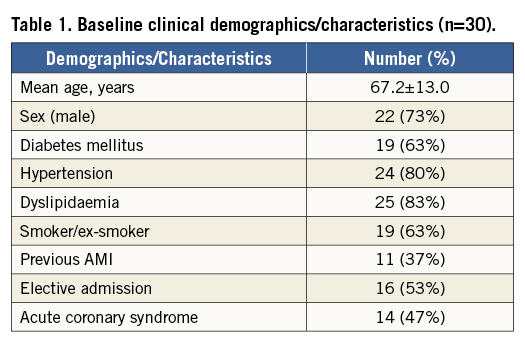
The mean age of the patients was 67.2±13.0 years (range, 40 to 82 years). There were 22 men (73%), 19 patients with diabetes mellitus (63%), 24 patients with hypertension (80%), 25 patients with dyslipidaemia (83%), and 19 smokers and/or ex-smokers (63%) among the patients. Sixteen patients (53%) were elective admissions, and 14 patients presented with acute coronary syndrome, of which one was an ST-elevation acute myocardial infarction transferred for primary PCI.
LESION CHARACTERISTICS (Table 2)
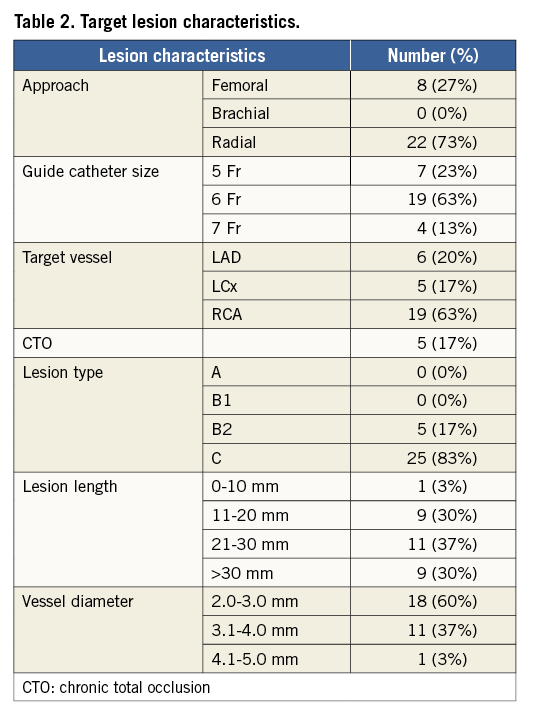
Among the 30 patients, the approach site was the femoral artery in eight (27%) and the radial artery in 22 patients (73%). The size of the mother guide catheter was 5 Fr in seven patients (23%), 6 Fr in 19 patients (63%), and 7 Fr in four (13%). Nineteen patients were right coronary artery (RCA) interventions, six were left anterior descending (LAD) interventions and five were left circumflex (LCx) interventions. Stent delivery failed in one case because of severe tortuosity in an RCA lesion (Figure 2). Five cases involved treatment of chronic total occlusion. The morphologies of the lesions consisted of five patients (17%) type B2, and 25 (83%) type C.
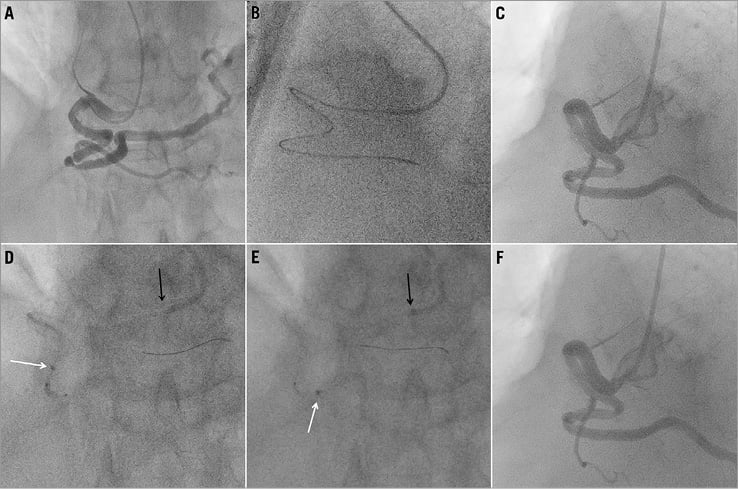
Figure 2. A case of stent delivery failure with mother-child technique using a 4 Fr inner catheter. A) Coronary angiogram showing severe stenosis in the mid RCA. B) A 6 Fr SAL 1.0 guide catheter was engaged using the right radial approach. Then a Corsair microcatheter (ASAHI Intecc, Aichi, Japan) was required to cross the guidewire to the distal lesion because of severe elongation. C) A 2.5/15 mm balloon was crossed with a 4 in 6 system. D) & E) A 4 Fr inner catheter was engaged deeply with the distal balloon deflation technique. However, the PES (3.5/24 mm) could not cross the culprit lesion. F) Since adequate vessel dilatation was accomplished with 2.5 mm POBA, stent deployment was not performed. Black arrows indicate the position of the 6 Fr mother guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
PROCEDURAL CHARACTERISTICS (Table 3 and Table 4)
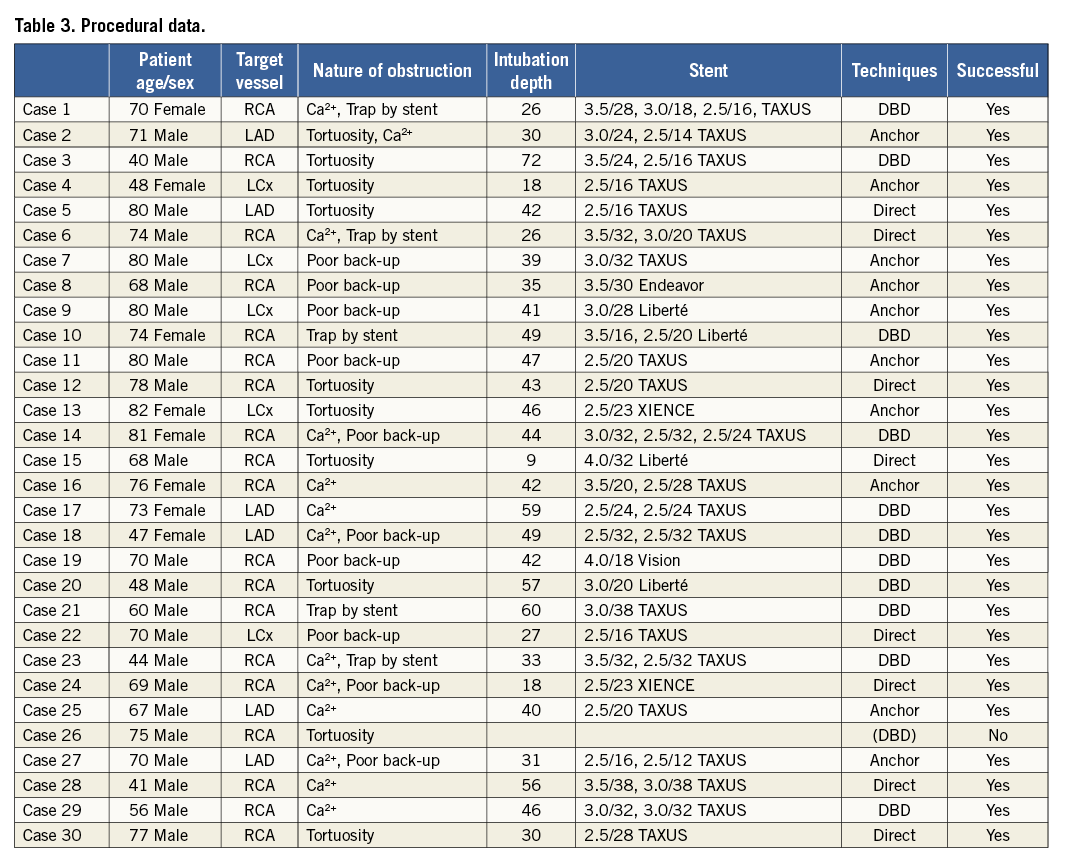
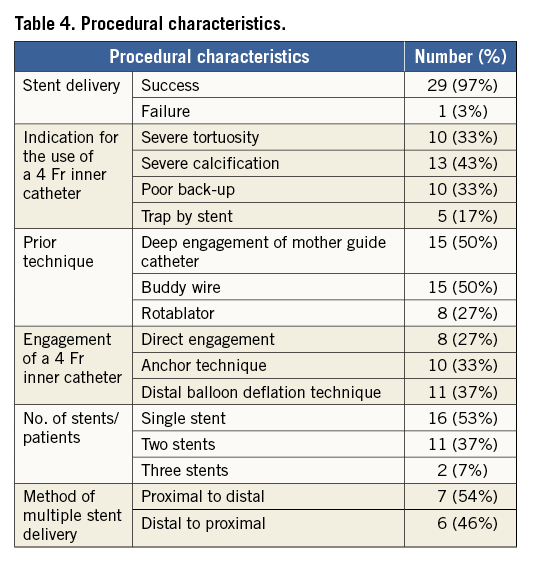
Indications for the use of a 4 Fr inner catheter were severe tortuosity (33%), severe calcification (43%), poor back-up support (33%), and trapping of the stent proximal to the target lesion (17%). Prior techniques which were not effective for stent delivery were the deep engagement of mother guide catheters in 15 patients (50%), the buddy wire technique in 15 patients (50%), and rotational atherectomy in eight patients (27%). Stent delivery was accomplished with direct engagement of a 4 Fr inner catheter in eight cases. In the remaining 22 cases, the stent could not be passed with direct engagement of a 4 Fr inner catheter. Of these, stent delivery was accomplished in 10 cases with the anchor technique, and in 11 cases with the distal balloon deflation technique (Figure 3, Online Figure 2). In four cases, the distal balloon deflation technique was effective for stent delivery after the failure of the anchor technique (Figure 4). Single stent delivery was performed in 16 cases. Multiple stent delivery was performed in 13 cases. Proximal stent delivery followed by distal stent deployment was performed in seven cases (Figure 5). This method was applied after deep engagement of a 4 Fr inner catheter with the distal balloon deflation technique in all seven cases. There were no procedural complications related to the use of the catheter (such as coronary dissection, coronary perforation and air embolism). There were no deaths, myocardial infarctions or in-hospital target vessel surgical revascularisations. Creatine phosphokinase-MB was measured after coronary angioplasty and an increase greater than three times the upper limit of the normal values was considered to represent myocardial infarction. Blood loss from the gap between the mother and child guide catheter was negligible during the procedure because a small haemostatic valve was routinely reconnected.
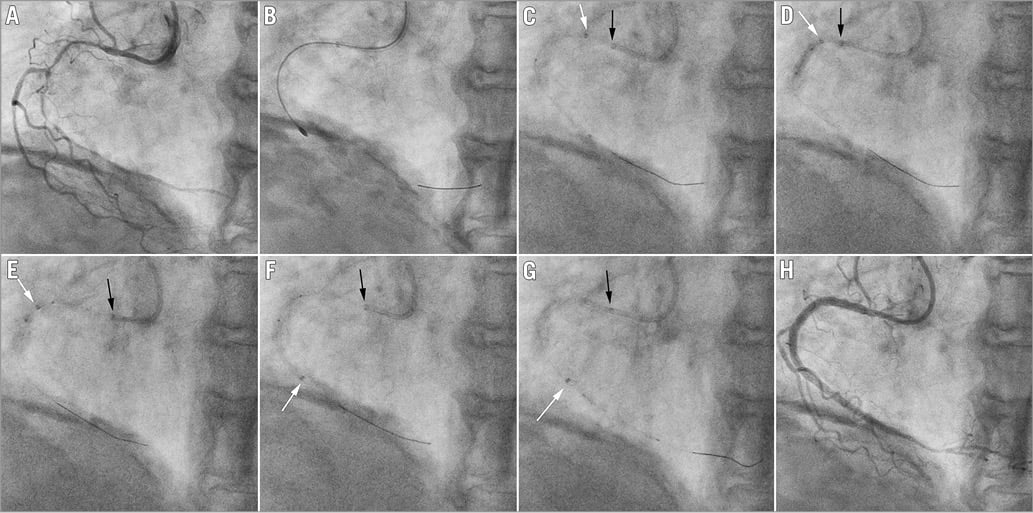
Figure 3. A case of stent delivery with mother-child technique using a 4 Fr inner catheter - distal balloon deflation technique. A) Coronary angiogram showing severe stenosis in RCA. 5 Fr SAL 1.0 mother guide catheter was engaged using the right radial approach. B) 1.5 mm rotational atherectomy was performed. After predilatation with a 2.5 mm balloon, the first PES (2.5/32 mm) could not be crossed distally and was deployed at the mid RCA with a 4 in 5 system. C) The first and second PES (3.0/32 mm) were deployed at the proximal RCA. D), E) & F) A 4 Fr inner catheter was passed within and beyond the first PES using the distal balloon deflation technique. G) The third PES (2.5/24 mm) was crossed within the 4 Fr inner catheter and deployed at the distal RCA. H) Final angiogram. Black arrows indicate the position of the 5 Fr mother guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
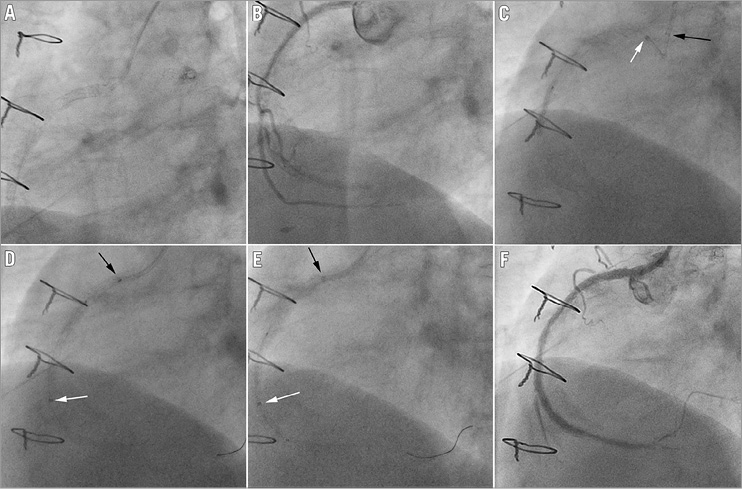
Figure 4. A case of stent delivery with mother-child technique using a 4 Fr inner catheter - distal balloon deflation technique. A) Six SES had been deployed at RCA over five years after CABG and the RCA ostium had been treated by positioning the stent with a slight degree of overhang in the aorta. B) Coronary angiogram showing restenosis at mid RCA. A 5 Fr IL 3.5 mother guide catheter was engaged after the failure of a 6 Fr JR 4.0 guide catheter. C) After 2.5 mm POBA, a 4 Fr inner catheter could not be engaged with the anchor technique. D) A 4 Fr inner catheter was deeply engaged with the distal balloon deflation technique. E) The PES (3.0/38 mm) was passed within a 4 Fr inner catheter and deployed at mid RCA. F) Final angiogram after 3.25 mm POBA. Black arrows indicate the position of the 5 Fr guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
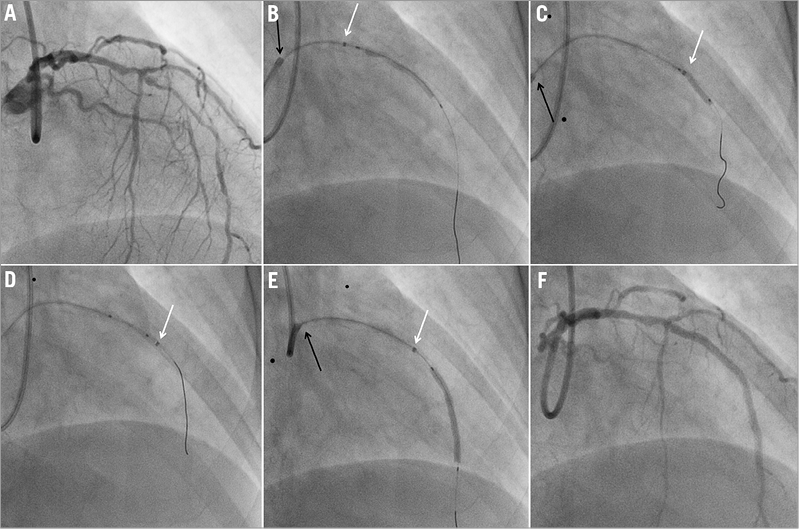
Figure 5. A case of stent delivery with mother-child technique using a 4 Fr inner catheter - proximal stent delivery followed by distal stent deployment. A) Coronary angiogram showing diffuse stenosis in LAD. A 6 Fr XB 3.5 guide catheter was engaged using the right radial approach. B) After predilatation with a 2.5/15 mm balloon, the first PES (2.5/32 mm) could not be crossed distally and was deployed at the proximal LAD with a 4 in 6 system. C) & D) A 4 Fr inner catheter was deeply engaged using the distal balloon deflation technique with a 2.5 mm balloon. E) The second PES (2.5/32 mm) was deployed distally through a 4 Fr inner catheter. F) Final angiogram. Black arrows indicate the position of the 6 Fr guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
Discussion
Transradial intervention (TRI) and the use of smaller-sized guide catheters are becoming more frequent in view of reduced invasiveness, fewer bleeding complications and early recovery to normal ambulation13-16. This technique could also provide another treatment strategy for complex angioplasty procedures. In our study, 22 out of 30 patients (73%) received TRI, which seems to be somewhat different from Western countries. In a previous report, Takahashi et al showed that the mother-child technique using a 5 Fr inner catheter had been introduced to improve back-up force and was effective as a distal stent delivery device3. Although extra deep intubation with a 5 Fr inner catheter facilitates stent delivery by traversing proximal points of obstruction and by increasing back-up force, a 5 Fr inner catheter often cannot be advanced into an angulated calcified lesion because of the larger diameter of a 5 Fr inner catheter (1.73 mm)17. The GuideLiner® catheter (Vascular Solutions Inc., Minneapolis, MN, USA) is also available for difficult stent delivery. The GuideLiner catheter, which is more than 5 Fr, is a coaxial guide catheter extension delivered through a standard guide catheter on a monorail18. Since it neither lengthens the guide catheter nor requires a second haemostatic valve, it is thought to be easy to use. However, it is still problematic for stent delivery in the angulated and/or the distal lesion because of its larger profile. The recent development of a 4 Fr inner catheter has enabled a distal stent delivery instead of a 5 Fr inner catheter in daily practice. Previous reports have demonstrated its characteristics in terms of its low profile and limited back-up force compared with a 5 Fr inner catheter10,11. The proper alignment of both a 4 Fr inner catheter and a mother guide catheter is required to overcome a limited back-up force for stent delivery in some cases without deep engagement11. However, deep engagement of a 4 Fr inner catheter was still required in many cases. Although the soft end portion of a 4 Fr inner catheter can easily negotiate the distal tortuous coronary vessel without vessel injury because of the smaller outer diameter of a 4 Fr inner catheter (1.43 mm), it is difficult to engage a 4 Fr inner catheter distally with the direct engagement method because of a limited back-up force. The anchor technique and the distal balloon deflation technique are sometimes required for deep engagement of a 4 Fr inner catheter. In particular, the distal balloon deflation technique is effective for a stent delivery which may temporarily change the orientation of the proximal section in a favourable way to allow passage of a 4 Fr inner catheter deeply12.
In general, it is well known that the distal stent should always be implanted before proximal ones and that recrossing with another stent over a recently deployed stent should be avoided because of the risk of stent loss and/or stent dislodgement19. Although a previous report has shown the risk of stent dislodgements with a 4 Fr inner catheter10, we did not encounter any cases of stent dislodgement. By using the distal balloon deflation technique, a 4 Fr inner catheter can be engaged deeply and easily within and beyond the deployed proximal stent. In this situation, a stent can easily be deployed distally within a 4 Fr inner catheter in a similar way to the aspiration catheter4.
As with the use of a 4 Fr inner catheter, care withdrawing and introducing balloons and stents is necessary to avoid sucking air into the catheter which can be injected distally. The internal lumen of a 5 Fr mother guide catheter should be more than 1.43 mm for the 4 Fr inner catheter to pass through. Types of DES which can be deployed within a 4 Fr inner catheter using a conventional 0.014 inch guidewire are the TAXUS® Liberté® (Boston Scientific, Natick, MA, USA), Endeavor® and Resolute Integrity® (Medtronic, Minneapolis, MN, USA) and XIENCE X-pedition (Abbott Vascular, Santa Clara, CA, USA) with diameters up to 3.5 mm, and the XIENCE V® (Abbott Vascular) with diameters up to 2.5 mm. All types of DES can be deployed using a 0.010 inch guidewire instead of a 0.014 inch guidewire. Most bare metal stents can be passed through a 4 Fr inner catheter.
In conclusion, the use of a 4 Fr inner catheter is both safe and effective for aiding distal stent delivery. Coaxial alignment of a 4 Fr inner catheter and mother guide catheter is highly recommended without deep engagement of a 4 Fr inner catheter. Deep engagement of a 4 Fr inner catheter can be accomplished with the anchor technique and the distal balloon deflation technique. Proximal stent delivery followed by distal stent deployment can be accomplished safely by deep engagement of a 4 Fr inner catheter. Further study will be required to compare the difference between a 4 Fr and a 5 Fr inner catheter.
| Impact on daily practice We show that the use of a 4 Fr inner catheter is both safe and effective for aiding distal stent delivery. The anchor method and the distal balloon deflation technique are highly recommended to engage a 4 Fr inner catheter deeply. Proximal stent delivery followed by distal stent deployment can be accomplished easily with a 4 Fr inner catheter. This simple method has served as a reliable and safe solution for stent delivery failure. |
Conflict of interest statement
The authors have no conflicts of interest to declare.
Online Figure 1. A 4 Fr inner catheter within a 5 Fr mother guide catheter connected with a Y-connector. Black arrows indicate the position of the 5 Fr mother guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
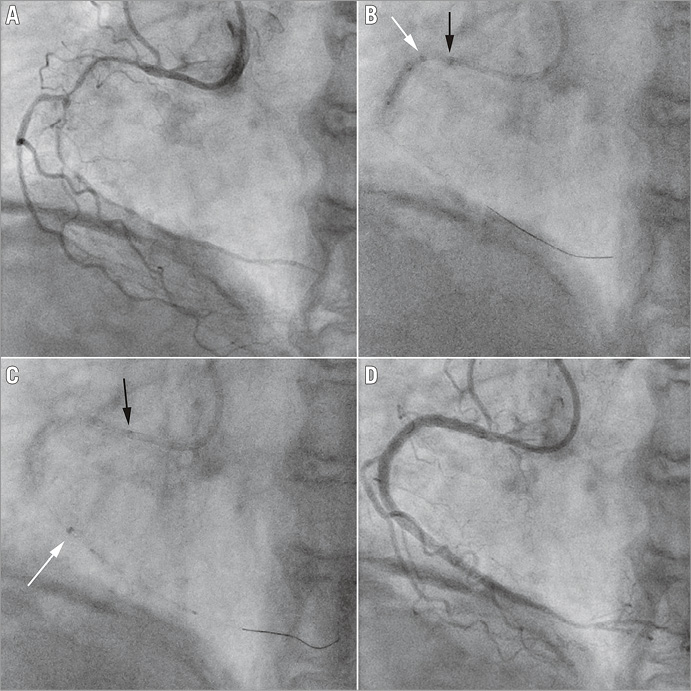
Online Figure 2. A case of stent delivery with mother-child technique using a 4 Fr inner catheter - distal balloon deflation technique. A) Coronary angiogram showing severe stenosis in RCA. A 5 Fr SAL 1.0 mother guide catheter was engaged using the right radial approach. B) A 4 Fr inner catheter was passed within and beyond the first PES using the distal balloon deflation technique. C) The third PES (2.5/24 mm) was crossed within the 4 Fr inner catheter and deployed at the distal RCA. D) Final angiogram. Black arrows indicate the position of the 5 Fr mother guide catheter, and white arrows indicate the position of the 4 Fr inner catheter.
