Description
A 4 Fr child catheter (KIWAMI ST01; Terumo Corp., Tokyo, Japan) can be used in combination with a conventional 6 Fr mother guiding catheter to deliver stents into complex coronary lesions without difficulties1. Four Fr child catheters can be inserted into 6 Fr or 7 Fr guiding catheters with a second guidewire for side-branch protection. In this report, we introduce a new technique for delivering stents into complex bifurcation lesions with side-branch protection.
Technical specifications
KIWAMI ST01 is a long catheter (length, 120 cm). Since it has an inner diameter of 1.27 mm (0.050 in), it can accommodate most of the currently available coronary stents1. In addition, its small outer diameter of 1.43 mm (0.056 in) allows its use as a child catheter for conventional 6 Fr or 7 Fr guiding catheters with a second guidewire for side-branch protection.
Indications for use
This technique is useful for delivering stents into complex bifurcation lesions with side-branch protection.
Tips and tricks for use
After advancing the second guidewire into the side branch for protection, the Y-connector is detached from the mother catheter and attached to the child catheter. The child catheter is then advanced along the main-branch guidewire through the haemostatic valve attached to the mother catheter. At this time, the second guidewire is in the space between the walls of the two catheters (Figure 1). When advancing the child catheter to the lesion, the use of an anchor balloon technique is recommended to prevent vessel injury by the tip of the child catheter. After advancing the child catheter close to the lesion, the balloon or the stent is advanced through the child catheter while the second guidewire is retained in the side branch. This technique does not differ from the conventional mother-child technique in terms of difficulty1.
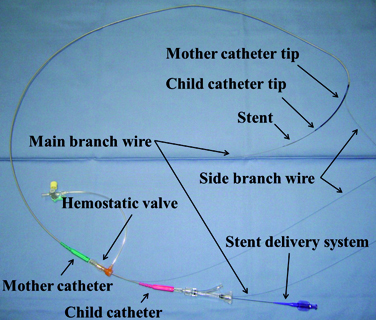
Figure 1. Mother-child system with a second guidewire for side-branch protection.
Clinical experiences
CASE 1
The patient was an 85-year-old man who presented with effort angina. A 6 Fr EBU 3.5 guiding catheter (TAIGA; Medtronic, Inc., Minneapolis, MN, USA) was engaged into the left coronary artery via the radial artery. Angiography showed severe narrowing from the left main trunk (LMT) to the left anterior descending artery (LAD) (Figure 2A, open arrow). After crossing a Runthrough® Hypercoat guidewire (Terumo Europe, Leuven, Belgium) to the LAD, the second Runthrough® Hypercoat guidewire was advanced to the left circumflex artery (LCX) for side-branch protection. Despite predilatation with a 3.5 ×15 mm balloon, a 3.5×23 mm Endeavor® Sprint stent (Medtronic) failed to cross the lesion owing to calcification of the proximal LAD (Figure 2B). With an anchor balloon technique, the 4 Fr child catheter was deeply advanced beyond the lesion (Figure 2C, large arrow), while the second guidewire was retained in the LCX (small arrow). The stent could be easily delivered to the lesion through the child catheter and was deployed from the LMT to the proximal LAD (Figure 2D). After the third guidewire (Fielder FC; Asahi Intecc, Aichi, Japan) was crossed to the jailed LCX through the stent strut, the second guidewire was retrieved and kissing balloon dilatation was performed using a 3.5 mm and a 2.0 mm balloon (Figure 2E). Subsequently, an additional 3.5×9 mm Endeavor® Sprint stent was deployed for residual stenosis in the proximal LMT (Figure 2F, arrowheads).
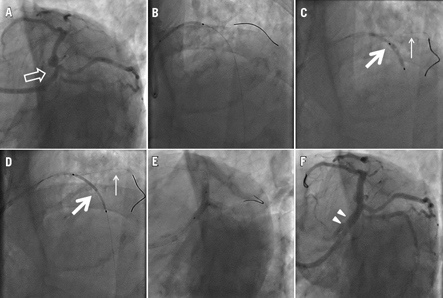
Figure 2. A) Baseline angiography showing severe narrowing from the left main trunk to the proximal left anterior descending artery (open arrow). B) The stent could not pass the lesion. C) The child catheter was advanced beyond the lesion (large arrow) with the second guidewire in the side branch (small arrow). D) The stent was delivered through the child catheter (large arrow) while the second guidewire was retained in the side branch (small arrow). E) After stenting, kissing balloon dilatation was performed. F) An additional stent was deployed in the proximal lesion (arrowheads).
CASE 2
The patient was a 62-year-old man undergoing long-term haemodialysis who presented with effort angina. A 7 Fr guiding catheter (SAL 1.0 SH, Launcher; Medtronic) was engaged into the right coronary artery (RCA) via the femoral artery. Baseline angiography revealed subtotal occlusion in the bifurcation of the atrioventricular (AV) and the posterior descending (PD) branches (Figure 3A, open arrow). A Wizard 1.0 guidewire (Japan Lifeline Co. Ltd, Tokyo, Japan) with FineCross™ microcatheter (Terumo) was advanced into the AV branch, and a Runthrough Hypercoat guidewire was advanced into the PD branch. Despite predilatation of both branches, a 2.5×24 mm Endeavor Sprint stent failed to cross the mid RCA. By deeply advancing a 4 Fr child catheter (Figure 3B, large arrow), the Endeavor Sprint stent was easily delivered and implanted in the AV branch across the PD branch. After successful re-crossing of the guidewire, the stent strut and the proximal PD branch were dilated. However, the second Endeavor Sprint stent (2.5×24 mm) could not pass the mid RCA. Thus, the 4 Fr child catheter was again advanced close to the lesion (Figure 3C, large arrow). This time, the protective guidewire was intentionally left in the AV branch (small arrow). Through the 4 Fr child catheter, the second stent could be easily delivered and was implanted into the jailed PD branch (Figure 3D). With the protective guidewire in place, the Wizard guidewire easily re-crossed to the AV branch through the strut of the second stent. Final kissing balloon dilatation was performed using two 2.5×15 mm balloons (Figure 3E). Finally, an additional 3.0×18 mm Endeavor Sprint stent was deployed in the mid RCA, using the 4 Fr mother-child technique, followed by post-dilatation with a 3.25×12 mm balloon (Figure 3F, arrowheads).
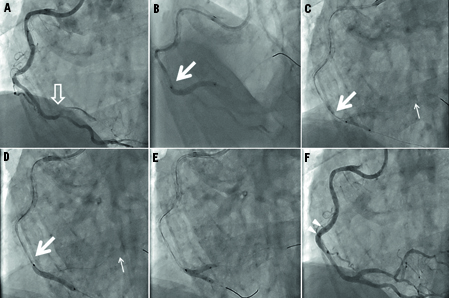
Figure 3. A) Baseline angiography showing proximal tortuosity and subtotal occlusion (open arrow) in the right coronary artery (RCA). B) The stent was implanted in the atrioventricular (AV) branch across the posterior descending (PD) branch by using a child catheter (large arrow). C) The child catheter (large arrow) was advanced to the distal RCA while the second guidewire was retained in the AV branch (small arrow). D) The second stent was implanted into the PD branch with the protective guidewire in the AV branch (small arrow). E) After stenting, kissing balloon dilatation was performed. F) An additional stent was deployed in the proximal lesion (arrowheads).
Discussion
In these two cases, delivery of coronary stents was difficult using the conventional technique because of severe calcification and/or tortuosity of the target vessel. Moreover, protecting the large side branches seemed crucial for procedural success. We thus used a 4 Fr mother-child technique with side-branch protection. Placing a second, protective guidewire in the side branch during main-branch stenting is a safe and effective approach to prevent occlusion. Although other mother-child systems, including the 5-in-6 and 5-in-7 systems with a 5 Fr child catheter2 and the 6-in-7 system with the GuideLiner catheter (Vascular Solutions, Inc., Minneapolis, MN, USA)3, can also accommodate a second guidewire, deep insertion of large child catheters easily compromise coronary flow. Furthermore, in the 5-in-6 and 5-in-7 systems, the second guidewire does not pass the space between the two catheters. Thus, the wire has to go through the inner lumen of the child catheter, the retrieving of which becomes somewhat cumbersome because it will require two extension wires.
Currently, two different Japanese manufacturers –Terumo and Asahi Intecc– produce 4 Fr child catheters. The outer diameter of the Cokatte catheter from Asahi Intecc is slightly larger than that of the Kiwami catheter from Terumo (1.50 and 1.43 mm, respectively). Although the difference in the outer diameter is <0.1 mm, the Cokatte catheter cannot be inserted into a 6 Fr mother guiding catheter with the second, protective guidewire.
This technique has several limitations. First, the second guidewire should be advanced into the side branch before introducing a child catheter because of the limited space between the child and mother catheters. Second, the 4 Fr child catheter cannot accommodate two balloon catheters2. Therefore, before the final kissing balloon inflation, the 4 Fr child catheter should be retrieved from the mother guiding catheter. Third, the operator should be cautious about the risk of air embolism while advancing the balloon/stent through a child catheter.
References