Introduction
Stent delivery failure (SDF) is infrequently encountered during percutaneous coronary interventions (PCI) but is associated with increased morbidity1,2. SDF can occur when the proximal segment is tortuous, calcified and formerly stented. Different techniques can be tried such as exchanging the stent for a stent with an improved crossing profile, lubricating its surface, changing the guiding catheter (or using a dedicated delivery catheter) or the guidewire, or using an “anchor”.
The “anchor balloon technique” was initiated in PCI of chronic total occlusions3,4 and is achieved by inflating a balloon in a non-target vessel in order to obtain enough support to cross a lesion. Anchor balloon technique in a non-target vessel cannot be performed in all SDF because of failure of an appropriate non-target vessel, or due to low support by non-axial traction (Figure 1). Consequently, we use a modified technique in order to allow coaxial traction.
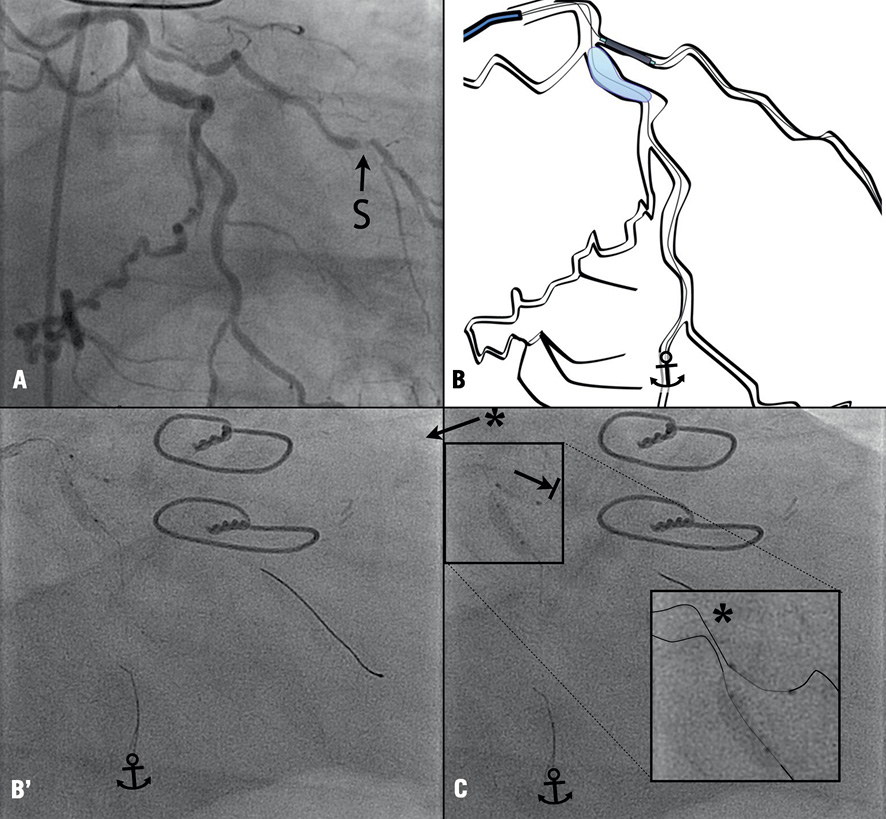
Figure 1. Failure of the classical (non-axial) balloon anchor technique. A 3.5/10 mm balloon is used as anchor ( ) in a proximal part of the left circumflex artery. Pushing down a 2.25/8 mm everolimus-eluting stent (S)(XIENCE PRIME™; Abbott Vascular) is not possible and associated with bulging (*) of the guidewires and retrieval of the 6 Fr CLS 3.5 guiding catheter (arrow).
COAXIAL BALLOON ANCHOR TECHNIQUE STEP BY STEP (Figure 2)
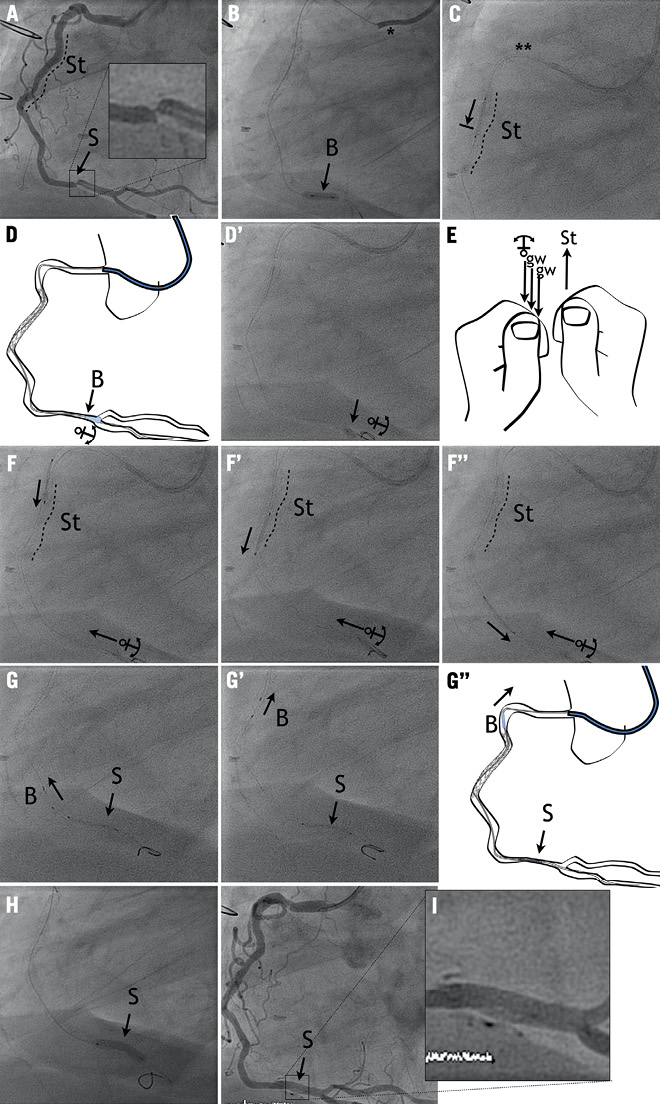
Figure 2. Modified balloon anchor technique to overcome stent delivery failure. A) The coronary angiogram showed a tight focal stenosis (S) of the distal part of the RCA and non-significant restenosis in a previously implanted proximal stent (St, dashed line). B) Using a 6 Fr Amplatzer left 2 guiding catheter (*) a balloon angioplasty was achieved with 3.0/10 mm Trek® balloon (Abbott Vascular) over a Whisper MS® guidewire (Abbott Vascular). C) Despite the use of one stiffer “buddy” guidewire (**) (Magnum®; Biotronik), a 3.5/15 mm sirolimus-eluting stent (Orsiro®, Biotronik) stayed trapped within the proximal stent. D, D’) The balloon anchoring ( ) was performed by inflating a 3.0/10 mm Trek balloon (B)(6-8 bars) at the distal bifurcation of the vessel. E, F”) This allowed delivery of the 3.5/15 mm sirolimus-eluting stent over the second guidewire by pulling on the anchor and pushing the stent. G, G”) Then the balloon was deflated and retrieved as well as the Magnum® wire acting as “buddy”. H) Finally, the 3.5/15 mm sirolimus-eluting stent (15 bars) was able to be delivered with a good final result (I).
STEP 1 – MATERIAL SELECTION, LESION PREPARATION AND BUDDY WIRE
When difficulty in crossing the proximal lesion is anticipated, the operator should choose a guiding catheter of increased size (>6 Fr) and extra-support shape (Panel A, Amplatzer left 2 guiding catheter) and polymer-covered guidewires (here, Whisper®; Abbott Vascular, Redwood City, CA, USA). The lesion should be well prepared (Panel B, 3.0/10 mm Trek®; Abbott Vascular).
A second guidewire is then placed as a “buddy”. When the initial guidewire is rigid, then the second guidewire should be more floppy, and vice versa. An attempt should be made to deliver the stent on both guidewires alternately.
STEP 2 – BALLOON ANCHORING AND STENT DELIVERY
In case of SDF (as illustrated in Panel C), a balloon is then placed distally to the target lesion. In order to perform powerful anchoring, one should consider a normal to slightly bigger balloon than the “landing” reference vessel diameter. This would allow potent anchoring with low inflation pressure (<6 atm).
The stent is then placed over the second guidewire. After opening the Y-connector to allow easy gliding of the four components, the operator pulls on the balloon and both guidewires (gw) as an anchor with one hand and pushes the stent (St) down towards the target lesion (Panels E-F’’) with the second hand.
STEP 3 – BALLOON RETRIEVAL, STENT IMPLANTATION AND FINAL ANGIOGRAM
Then, the balloon is deflated and retrieved as well as the buddy guidewire (Panels G-G”). The stent is implanted (Panel H, 3.5/15 mm Orsiro® stent, 15 bars; Biotronik, Bülach, Switzerland).
The final result (Panel I) should be carefully reviewed since such “forced” delivery might induce iatrogenic lesion at the coronary ostium, along the delivery route and at the anchoring place. An example of a spiral dissection of the anchoring zone is illustrated in Figure 3.
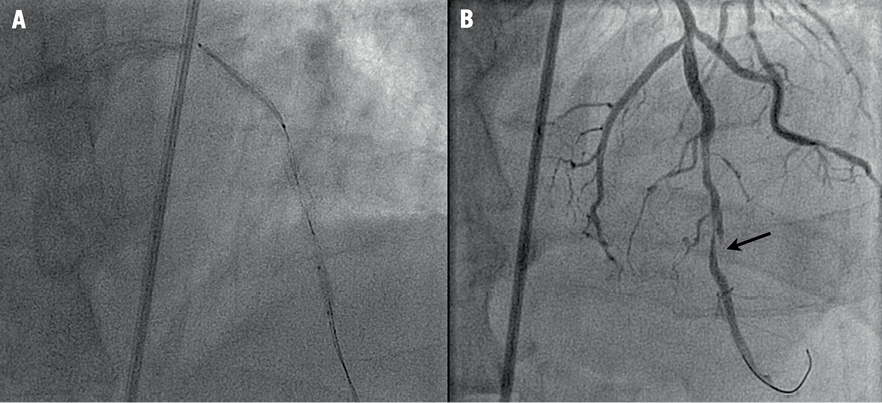
Figure 3. Dissection of the anchoring segment as acute complication of the technique. A) The anchoring technique with stent entrapment within a previously implanted stent, backwards movement of the anchor. B) This caused a spiral dissection of the anchoring segment (D).
Discussion
This modified anchor balloon technique consists of inflating a balloon inside the distal target vessel. The guiding catheter is consequently anchored and usually allows the adequate delivery of a second stent. This technique is easy to perform in a variety of coronary anatomic situations (Figure 4), and has a low risk of complications.
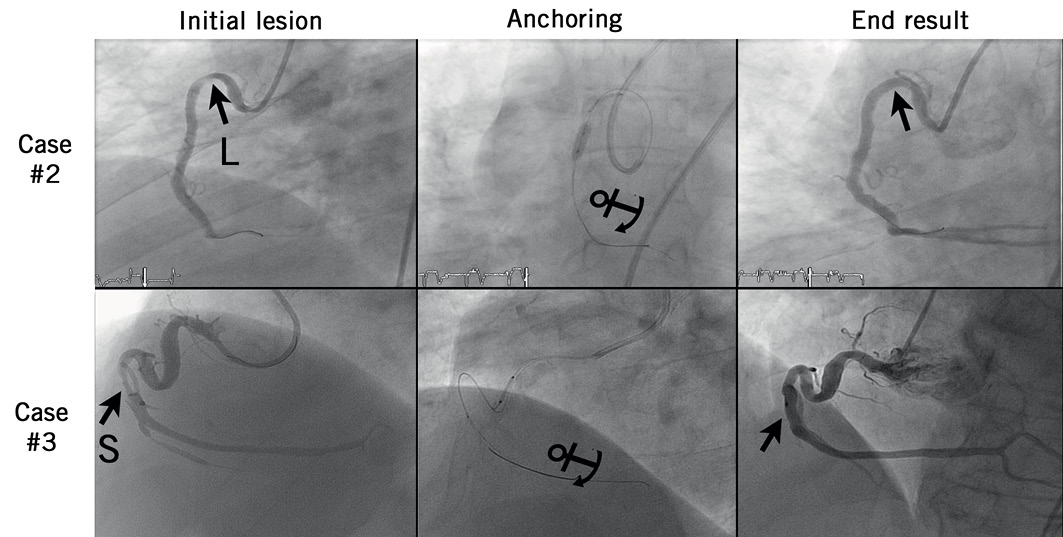
Figure 4. Coronary angiograms before and after successful use of the modified balloon anchor technique to overcome stent delivery failure in case #2 and case #3. L: lesion; S: stent
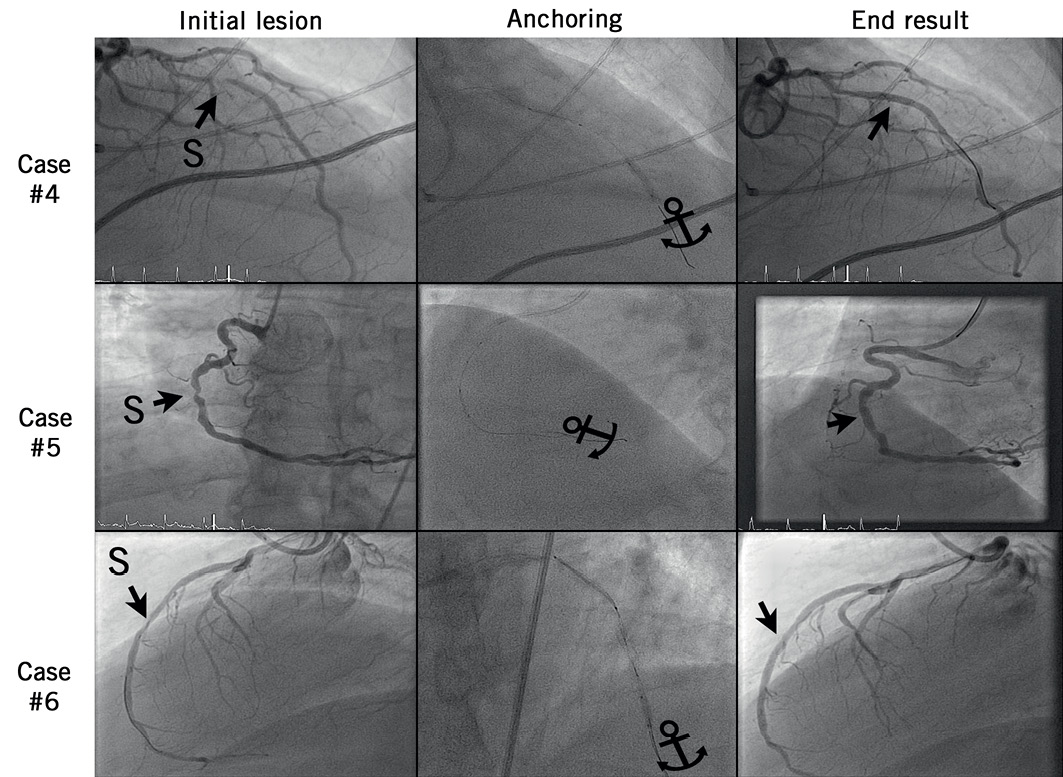
Figure 4. Coronary angiograms before and after successful use of the modified balloon anchor technique to overcome stent delivery failure in cases #4-6. S: stent
Conflict of interest statement
S. Cook received lecture fees from Biotronik, and research grants from Abbott Vasc, Biosensors Int., Biotronik, Boston Sci, Cordis, Terumo, Medtronic. The other authors have no conflicts of interest to declare.
