“To doubt everything or to believe everything are two equally convenient solutions, which, in both cases, frees us from thinking.”
Henri Poincaré (1854-1912)
The current convergence of several publications on the longitudinal deformation of coronary stents during percutaneous coronary interventions (PCI) caused by a conflict with one of our endovascular tools raises several comments1-4. The approaches were certainly different: one publication involved three precisely described cases1; another, nine cases –just as well described– associated with a 4-year retrospective analysis of the incidence of this complication in a very high-volume centre3; another article was an engineering analysis2, and, finally, a comparative mechanical and experimental evaluation of 14 contemporary coronary stent designs using a bench test method proposed by a team of researchers from Abbott Vascular4.
In summarising all of these publications, we come up with several points concerning deformation and compression:
1) Certain are stent longitudinal deformations by accidental compression, exceptionally occurring during PCI (0.2% of cases) by conflict with an endovascular tools1,2,4.
2) Others are new mechanical complications1-4.
3) Others occur on new generation stent platforms1,3.
4) There are also possible questions concerning the mechanical originality of contemporary coronary stent designs (stent strut thickness, alloys, 3D stent design)1-4.
5) This appears to occur more often with the Promus Element stent®3, an offset peak-to-peak stent design as described in the specific classifications proposed by Prabhu et al (from Abbott Vascular), which could be responsible for a longitudinal deformation 4.7 times higher than the average of deformations observed in the remaining 13 stents tested during a longitudinal compression force of 50 grams or approximately 0.5 N4 (this paper represents careful experimental work, but has a clear conflict of interest).
These findings merit discussion as they can stigmatise a particular stent design or a specific stent beyond the primary goal of these publications, which was to highlight an exceptional mechanical complication, the longitudinal deformation by accidental compression of these stents during PCI.
Mechanical compression, systematically accidental in PCI?
The claim that because the nine cases reported were treated by six different operators3 than the deformations observed cannot be exclusively due to procedural technique is inexact; all of these (and we ourselves commit these same things as well!) were accidental and a matter of procedure. The force required to induce longitudinal deformation in a stent is 0.1 to 1 N. Angioplasty is always highly operator-dependent. This accounts for the non-reproducibility of procedures. Moreover, the cases highlighted by Williams et al were exceptional, at 0.097% of the 9,310 implanted stents or 0.2% of the 4,455 PCIs. The 12 published cases (3+9 cases)1,3 describe 11 proximal crushes and one distal crush. In eight cases, the longitudinal compression was caused by an unexpected or excessive penetration of the guide catheter, guide catheter extension or proximal embolic protection catheter. The radial approach, the curves of some guide catheters, or a 5 Fr catheter rather than a 6 Fr catheter, are all technical elements that can facilitate the intracoronary penetration of the guide catheter. In addition, during the removal of a balloon or a device, any resistance can cause a counteraction of the guide catheter. In four other cases this compression was likely caused by a mechanical conflict between proximal malapposed stent struts and post-dilatation balloons. These cases involved seven Promus Element (Pt-Cr), two Biomatrix (316 SS), one Endeavor (Co-Cr), one Taxus Liberté (316 SS) and one Resolute Integrity (Co-Cr). It should be noted that the average length of the stents implanted (one or two stents with overlapping) was 30.7 mm. An implanted stent is not going to deform all on its own: it needs some external stress.
A new mechanical complication in contemporary coronary stents?
Longitudinal compression is presented as being a new failure in coronary stenting. We should not, however, forget the early filament designs used in the Wiktor® and Freedom® stents (sinusoid design with helical coiling). The flexibility of the Freedom® stent was 2,500 times greater than that of the Palmaz-Shatz model5. Many operators will recall the de-structuring to which these stents were subject to6. The design was directly implicated in this, but had, on the other hand, two qualities that were greatly prized at the time – flexibility and arterial conformation. Stent design is all about compromise (Figure 1). These early designs, however, have since been abandoned because those two qualities were being ensured at the undue expense of others. This issue goes to the heart of the present argument about mechanical sensitivity to longitudinal compression. It is being reported now, and thus creating a focus of interest.
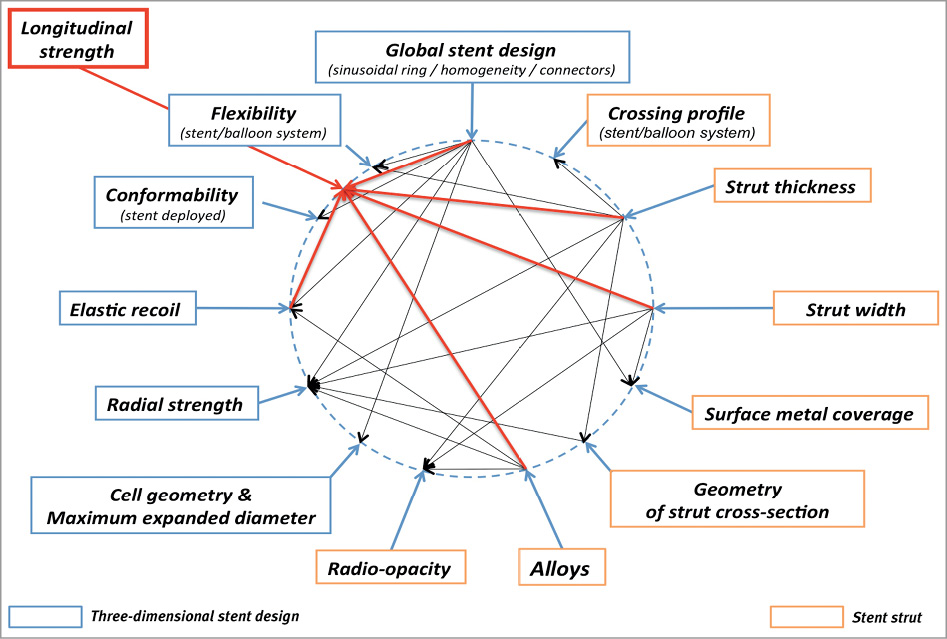
Figure 1. Intrication of various mechanical properties of stent platforms. The longitudinal compressive strength can become an additional criterion required in the selection of stents. It depends on the three-dimensional stent design, strut thickness, strut width and the alloy used with its intrinsic elastic modulus.
Longitudinal deformation detected by angiography
All cases were quickly detected and identified on angiography thanks to the accumulation of struts packed together –and sometimes superimposed– by accidental compression, thus increasing radio-opacity, particularly when the alloys contain platinum. Biophysics tells us that the probability of absorption of photons by photoelectric effect is dependent on the x-ray energy and proportional to the cube of the atomic number Z of the absorber, to triple Z is to increase the x-ray absorption by nine. The platinum has a Z at 78. Co, Cr, Ni, and Fe have a Z at 27, 24, 28, 26, respectively. The Promus Element stent is the only stent with Pt-Cr alloy (33% Pt, 37% Fe, 18% Cr). Its radio-opacity is much higher, and can thus lead to much easier angiographic detection (6/9 for Williams et al and 1/3 for Hanratty et al). So, for a given longitudinal stent deformation, angiographic detection can vary greatly from one model to another, which may lead to methodological confusion in incriminating one particular kind of stent. Hanratty and Walsh have detected a longitudinal compression by IVUS, undetectable by angiography with one Integrity Resolute stent (Co-Cr alloy).
The direct consequence of a specific stent design or a particular stent?
The classification used, which is specific to Abbott Vascular4, makes sense. However, the number, and particularly the longitudinal angle of the connectors (or links) between each sinusoid ring, play a key role in the stent’s longitudinal behaviour. Connectors parallel to the longitudinal stent axis show compression (or traction) under longitudinal stress (such as for the Multilink Vision, Prokinetic Energy, Coroflex blue, and Cypher), whereas those (such as in Promus Element) at a 30-45° angle show flexion. For a given deformation, the requisite force is generally 50 to 100-fold less under flexion than compression of the material. This provides a clear advantage in terms of other qualities (flexibility and conformation), once again, a compromise has to be achieved (Figure 1).
The force applied to the stents in the study of Prabhu et al was measured at 0.49 N from the force applied by balloon catheter on a constriction (mimicking the cases numbers 1-2-4-7-9 of Williams), but in all the other cases the compressive force was exerted directly by the tip of a guide catheter. In this case, the forces applied are much higher and can easily exceed 1 N. Beyond 0.50 N, the test could show that all stents crushed. The linearity between stress and strain is not always appropriate as shown by tests performed by Rieu et al during the experimental evaluation of radial force7. The Promus Element is the only one with Pt-Cr alloy, therefore this alloy could be responsible for mechanical differences. In fact, Pt-Cr alloy has a density and a tensile strength higher than Co-Cr and 316L, which is advantageous8. The mechanical sensitivity to longitudinal compression of the Promus Element is therefore only dependent on its design. Resistance to longitudinal compression is not the prime mechanical property to be looked for in a coronary stent. Increasing it means increasing stent structure rigidity and thus reducing flexibility (stent/balloon system) and arterial conformation following stent deployment, which are both major mechanical parameters in stenting, with direct effects on the coronary lesion being treated (intra-plaque stress distribution and arterial wall shear stress at either extremity of the stent) and non-negligible clinical impact.
Does accidental longitudinal deformation impact clinical safety for the patient?
There have been no adverse events in any of the cases presented by Hanratty, and two stent thrombosis at two months in the cases discussed by Williams et al (therefore a total of two of the 12 cases). PLATINIUM, a large scale (1,530 patients) prospective single-blind randomised trial comparing a Pt-Cr everolimus stent versus a Co-Cr everolimus stent showed no significant difference in terms of safety and efficacy through to 12-month FU after PCI9.
What lessons for PCI?
These studies have the great interest of collating and precisely describing 12 cases of longitudinal stent deformation by accidental longitudinal compression during PCI. The descriptive approach is exemplary, drawing attention to an exceptional event; it cannot, however, be said to be a novel phenomenon. Paradoxically, exceptional complications tend not to be reported, as they are hard to collate (being exceptional). The authors alert us to an incident that may entail serious technical consequences. In most cases, it is inextricably linked to the procedure itself. All scenarios must be anticipated so as to ensure against such events during intervention. To go beyond the precise analytic description of the 12 cases reported, specifically implicating a stent design with respect to its mechanical behaviour, remains, in the present state of our knowledge, entirely hypothetical and deductive as it is difficult to isolate a mechanical parameter without influencing the global mechanical behaviour of the stent.
Conflict of interest statement
The authors have no conflict of interest to declare.
