An 83-year-old gentleman with severe aortic valve stenosis was deemed eligible for transfemoral transcatheter aortic valve replacement (TAVR) after a Heart Team evaluation. Cardiac computed tomography showed severe calcification of the native aortic valve leaflets (Figure 1A1, Figure 1A2). A 30 mm self-expanding Hydra (Sahajanand Medical Technologies) transcatheter heart valve (THV) was chosen (Moving image 1). This novel supra-annular THV has a nitinol frame with large stent cells (≥15 Fr) and a three-tentacle design at the stent outflow. Bovine pericardium leaflets are attached to the stent by three commissures, placed between the three tentacles. Six radiopaque markers, aligned three by three in two rows, are positioned on the THV frame and guide the implantation depth during valve deployment. The location of the lower row of these markers on the stent frame corresponds to the base of each of the three cusps, but with a slightly asymmetrical distance to the middle of the base. Consequently, each of the prosthetic commissures is situated between the markers, also with a slightly asymmetrical distance (Figure 1A3). Currently, there are no specific recommendations concerning the optimal implantation technique to achieve a patient-specific commissural alignment (CA) with the Hydra THV1. Such a CA would require positioning the tentacles of the Hydra THV exactly above the base of each cusp of the native aortic valve, which would accordingly align each of the three prosthetic commissures with the native commissures (Figure 1B1, Figure 1B2). Patient-specific CA with the Hydra THV can be achieved using the angiographic right coronary cusp (RCC)-left coronary cusp (LCC) overlap view. In this projection, before valve deployment, one tentacle should be isolated on the left side of the screen and the other two tentacles should be overlapping on the right side of the screen (“1:2 pattern”); such positioning would be indicative of a proper CA, considering that one prosthetic commissure is placed exactly between the two overlapping tentacles (Figure 1B3). However, the tentacles are poorly visible when clustered within the catheter prior to valve deployment. Since the alignment of each of the six markers on the stent frame is much easier to assess in our patient, we tried to achieve CA by considering the orientation of these markers. A near-perfect CA can be achieved, if one of the base markers in the RCC-LCC overlap view is isolated on the left side of the screen and the other two base markers are situated on the right side of the screen; the same pattern can then be seen in the upper row of the stent markers. Keeping in mind the asymmetric distance between the markers and the prosthetic commissures placed between them, we call this a “near 1:2 pattern” (Figure 1B1-Figure 1B3). Employing this technique, we safely implanted the Hydra THV (Figure 1B4). After the THV deployment, we were able to easily recannulate both the right and left coronary arteries (Moving image 2, Figure 1C1, Figure 1C2). This empirically demonstrated, at least, a near-perfect patient-specific CA. Preserving coronary artery reaccess has become imperative in TAVR scenarios, and different techniques have been described to achieve a reliable CA with other commercially available THVs23. Hereby, we described a potential method for reaching a satisfactory CA with the novel Hydra THV. In the event that the alignment of the stent in the RCC-LCC view required some rotation of the delivery catheter, pulling back the delivery system into the descending aorta and turning it there could potentially modify the orientation of the stent markers. We do not suggest performing this manoeuvre in the aortic annulus or the ascending aorta, since the Hydra delivery catheter is not primarily designed to be rotated whilst curved (given the absence of a spine). Clearly, more robust clinical and post-implantation imaging data are needed to assess the safety and efficacy of the described technique in a broader patient population.
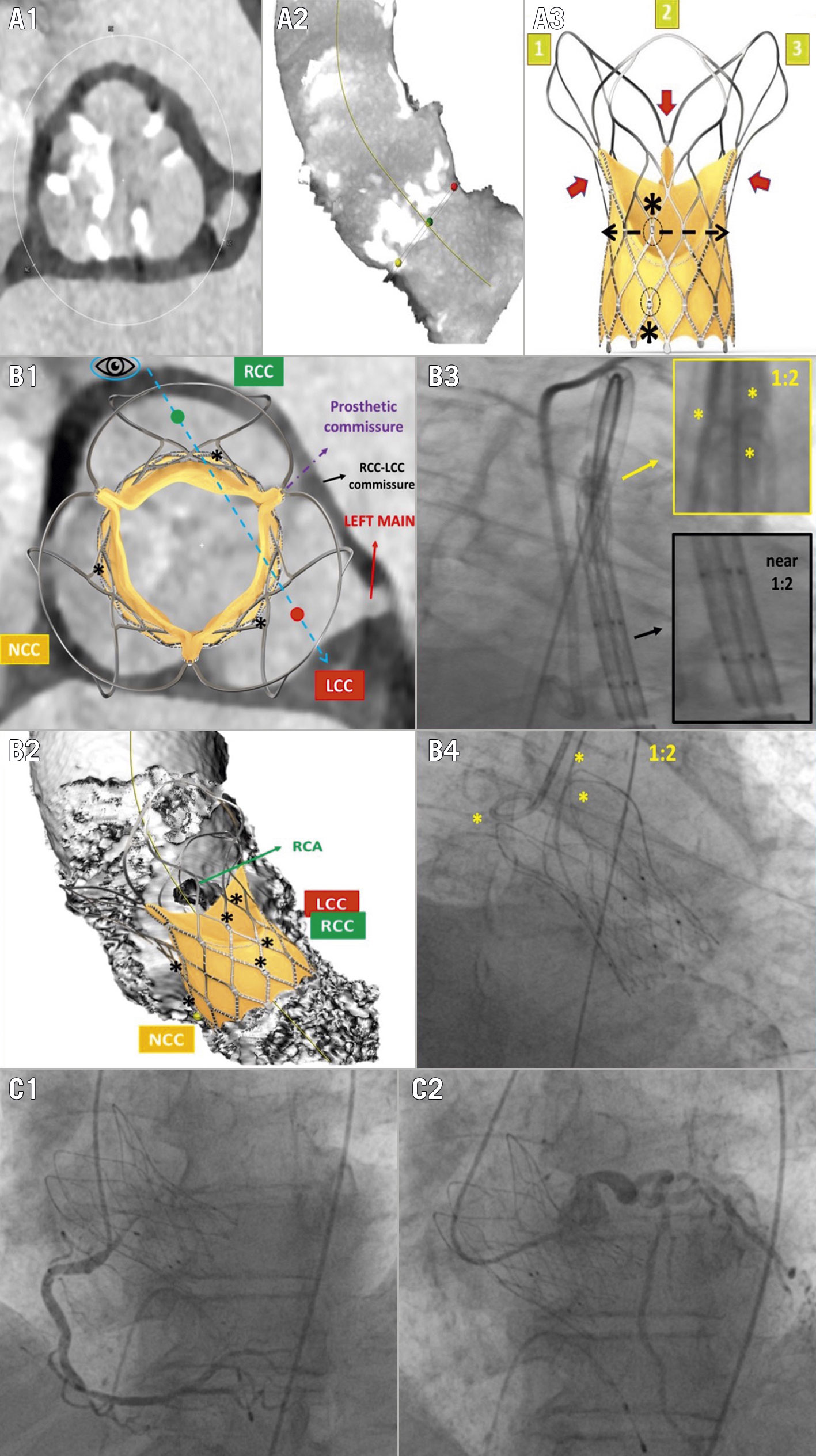
Figure 1. Commissural alignment with Hydra THV. Computed tomography showing severe aortic valve stenosis (A1), with 3-cusp view reconstruction (A2). The novel Hydra THV (A3) with the three-tentacle design (1,2,3) and commissural posts (red arrows) at their bases; six radiopaque markers are located three by three in two rows (black asterisks), each asymmetrically positioned between two prosthetic commissures (dashed lines). Proper commissural alignment (B1) is achieved using the RCC-LCC overlap view (B2, blue dashed line in B1) when one tentacle is on the left and the other two appear on the right (yellow box in B3); the radiopaque markers are seen in a “near 1:2 pattern”, without complete overlap of those located on the right side (black box in B3). Final angiographic result in RCC-LCC overlap view (B4). Easy right (C1) and left (C2) coronary artery reaccess. LCC: left coronary cusp; NCC: non-coronary cusp; RCA: right coronary artery; RCC: right coronary cusp; THV: transcatheter heart valve
Conflict of interest statement
G. Bieliauskas received consulting fees from Sahajanand Medical Technologies. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Hydra implantation with commissural alignment.
Moving image 2. Coronary artery reaccess.