A 43-year-old male underwent primary angioplasty over the left circumflex artery and was scheduled to have lesions in the left anterior descending artery (LAD) treated days later (Appendix Figure 1A). The intention was to treat all lesions with bioresorbable scaffolds but the most distal lesion had to be covered with a lower profile 2.25/38 mm everolimus Pt-Cr stent (SYNERGY™; Boston Scientific, Marlborough, MA, USA). Two 2.5/28 mm Absorb bioresorbable vascular scaffolds (BVS) (Abbott Vascular, Santa Clara, CA, USA) were implanted in the mid and proximal segments (Appendix Figure 1B).
The patient was admitted two months later for unstable angina showing progression of a previously moderate lesion in the right coronary artery which was treated. We evaluated the LAD with optical coherence tomography.
In the SYNERGY stent, a complete and smooth coverage was observed over all struts (Figure 1A). In the BVS, the degree of coverage was high but not complete (Figure 1B). The difference between the two could be related mostly to the large difference in strut thickness (74 µm vs. 150 µm). Nevertheless, we could not distinguish the neointimal or fibrin components of the thin strut-covering layers.
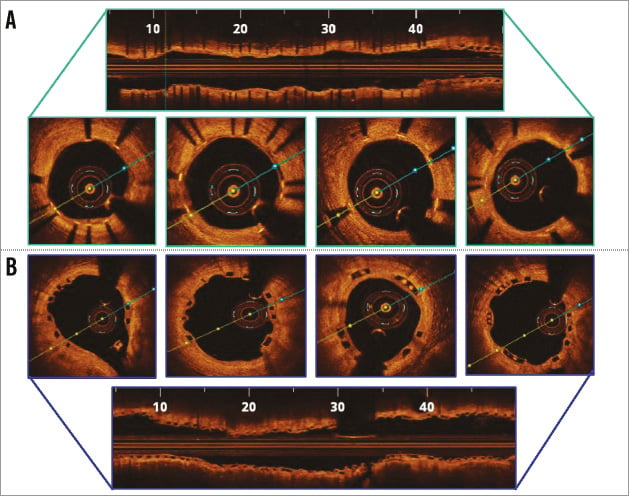
Figure 1. OCT findings two months after implantation. A) Everolimus Pt-Cr (SYNERGY) stent. B) Bioresorbable scaffolds (BVS).
Conflict of interest statement
J. M. de la Torre Hernandez receives research grants from Abbott Vascular, Boston Scientific, Biotronik, Biosensors, and St. Jude. He also receives payments for presentations and/or advisory board membership from Abbott, Boston Scientific, Biotronik, Medtronic, Biosensors, Volcano, Lilly, AstraZeneca. The other authors have no conflicts of interest to declare.
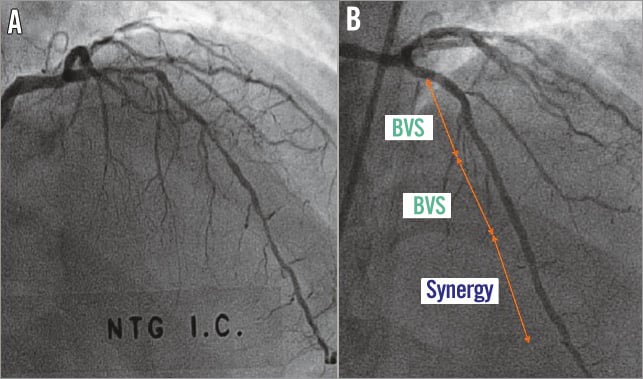
Appendix Figure 1. Angiographic images before and after stent implantation. A) Angiography showing lesions in the LAD. B) Angiographic result after stent implantation.
