Left ventricular (LV) spherical remodelling is the hallmark of heart failure with reduced ejection fraction (EF); it limits the efficacy of established pharmacological and non-pharmacological therapies and is associated with poor prognosis12. Physical LV geometry improvement (physical reverse remodelling) can reduce LV wall stress, promoting biological reverse remodelling12. The approximation (banding) of papillary muscles (PMs), performed during open-chest cardiac surgery, reduces the interpapillary distance and results in a more physiological (elliptical) LV shape3, with randomised study evidence showing long-term improvement in cardiac function3. A percutaneous PM banding system (VSling [Cardiac Success])1 has undergone testing in animal models and human cadavers4, paving the way for clinical evaluation. The VSling system consists of (1) a steerable 14 Fr outer catheter with a snare; (2) a system of two telescopic, three-dimensional (3D)-steerable, PM-encircling catheters (an intermediate catheter, providing support, and an atraumatic-tipped inner catheter, “paving the way”); (3) a delivery wire forming a loop around the PMs; and (4) the VSling itself (PM band), a looped wire-deliverable permanent implant whose circumference is adjustable prior to device locking and detachment from the delivery system.
Herein, we share procedural imaging (Figure 1) from the first ischaemic cardiomyopathy patient in a European multicentre study of transcatheter PM approximation: a 58-year-old male (with a history of two myocardial infarctions, a dilated LV and chronic heart failure refractory to established therapies), in whom we performed percutaneous VSling band (Supplementary Figure 1) implantation.
Procedure preparation involved, first, precise determination of the PM encircling pathway using computed tomography (CT)-based simulation of fluoroscopy and transoesophageal echocardiography (TOE; MrTEEmothy [Medical Simulation Technologies]) (Figure 1A, Moving image 1). Then, the encircling route was physically verified in a 3D print of the patient’s heart (Supplementary Figure 2). Finally, VSling delivery (transfemoral transaortic access using a steerable three-catheter system), tightening, and implantation were performed (Supplementary Figure 3, Supplementary Figure 4, Moving image 2, Moving image 3) under real-life fluoroscopy, with navigation support from CT-simulated fluoroscopy and TOE (Figure 1A). The procedure reduced the interpapillary distance from 27 mm to 12 mm (Supplementary Figure 4, Moving image 4); this resulted in a more conical LV shape (Supplementary Figure 5). Clinical improvement (an increase in the 6-minute walk test and New York Heart Association Functional Class improvement from III to II) and EF increase were maintained in follow-up (Figure 1B, Moving image 5, Moving image 6).
It is important to note that handling of the mitral subvalvular apparatus is not without risks, and potential chordal interactions with the PM band need to be avoided5. For this reason, PM morphology5 and their vascularisation6 need to be considered when assessing the feasibility of PM percutaneous realignment. The procedure reported herein involved type I PMs (i.e., each forming a single uniform unit)5 in a patient with a history of myocardial infarctions arising from left anterior descending coronary artery atherosclerotic disease in the absence of ischaemic lesions in the left circumflex and right coronary arteries. The realignment of PMs may present a particular challenge for type III and IV PMs, i.e., in case of partial separation of the PM heads5. These types are more prevalent in the posterior PM (PPM), while their occurrence in the anterior PM (APM) is rare. In type V PMs (in which the heads are anatomically separated), it is imperative that both heads are fully included in the encircling loop in order to prevent the “seagull sign” phenomenon. Furthermore, the segmental nature of the PM’s blood supply may require consideration, particularly in type IV and V PMs, in which the apex is more susceptible to ischaemic complications due to the fragility of its truncal blood supply and the degree of physical stress involved56. While the APM has dual blood supply, the PPM (supplied exclusively by the circumflex branch of the left coronary artery in case of predominant left circulation and exclusively by the posterior descending branches of the right coronary artery in case of predominant right circulation) is in general more susceptible to ischaemia6. These considerations are important for patient selection to avoid potential peri- and postprocedural mechanical complications that might arise from anatomy-related chordal interactions and PM ischaemia.
In conclusion, transcatheter approximation of the papillary muscles in the beating human heart is feasible, and, in suitable anatomy, it can be performed safely and with structural and functional benefits. Percutaneous PM banding does not obstruct other established or investigational therapeutic approaches to chronic heart failure17.
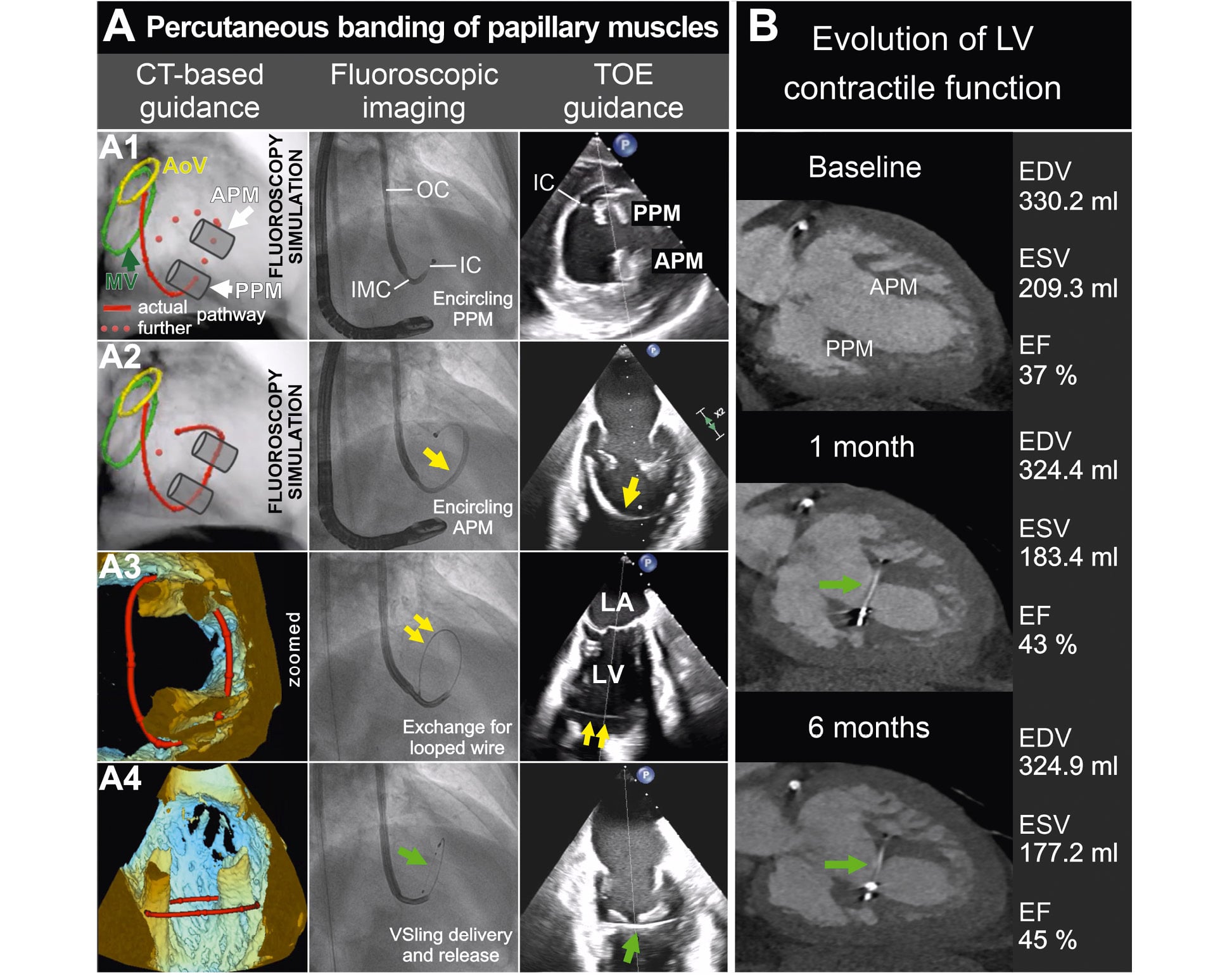
Figure 1. Transcatheter banding of papillary muscles. A) The key procedural steps are illustrated: (A1) PPM encircling with a telescopic 3D-steerable catheter system, (A2) encircling the APM (followed by snaring the inner catheter/wire), (A3) wire looped around the papillary muscles, and (A4) VSling band delivery, tightening and release. B) The evolution of LV volumes and contractile function over 6 months. Yellow arrow – the catheter system encircling papillary muscles; yellow double arrow – looped wire; green arrow – VSling. 3D: three-dimensional; AoV: aortic valve; APM: anterior papillary muscle; CT: computed tomography; EDV: end-diastolic volume; EF: ejection fraction; ESV: end-systolic volume; IC: inner catheter; IMC: intermediate catheter; LA: left atrium; LV: left ventricle; MV: mitral valve; OC: outer catheter; PPM: posterior papillary muscle; TOE: transoesophageal echocardiography
Acknowledgements
Drs Lukasz Czyz, Jakub Chmiel, Joanna Szachowicz-Jaworska and Anna Kedziora provided essential contributions to this report - along with Prof Jacek Piatek, Prof Rafal Drwila, Mr R. Pawel Banys and Ms Ewa Weglarz (all of St. John Paul II Hospital in Krakow, Poland). This publication was supported by the science fund of the St. John Paul II Hospital, Krakow, Poland (no. FN/6/2026 to P.M.).
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. CT-based simulation of the role of fluoroscopy in determining optimal procedural C-arm angulation.
Moving image 2. Transcatheter banding of papillary muscles using the VSling System – fluoroscopy cine images.
Moving image 3. Intraprocedural navigation using live transoesophageal echocardiography imaging.
Moving image 4. Transthoracic echocardiography – focus on the papillary muscles before (left) and after (right) banding.
Moving image 5. Transthoracic echocardiography imaging at baseline, and 1 and 6 months after percutaneous papillary muscle banding.
Moving image 6. Dynamic CT imaging (papillary muscles – aortic valve plane) at baseline, and 1 and 6 months after the transcatheter banding of papillary muscles.