Abstract
Aortic stenosis is the most prevalent valvular heart disease in the Western world, affecting over 12% of individuals aged 75 years and older. The optimal timing of transcatheter aortic valve implantation or surgical aortic valve replacement remains one of the most debated topics in contemporary cardiology, particularly for asymptomatic patients with severe disease or symptomatic patients with moderate aortic stenosis. Whilst symptomatic severe aortic stenosis has established indications for intervention, the management of these other groups of patients requires careful consideration of disease progression, myocardial damage, procedural risks, and long-term outcomes. Recent randomised controlled trials have provided preliminary evidence regarding early intervention strategies. This review examines the current evidence base for the timing of aortic valve replacement, with a particular focus on transcatheter aortic valve implantation, and discusses the implications of recent trial data for clinical practice and guideline recommendations.
Aortic stenosis is the most prevalent heart valve disease in the Western world, affecting an estimated 12.4% of individuals over 75 years of age1. With no medical therapy proven to slow disease progression or improve event-free survival2, the inexorable decline in valve function leaves surgical aortic valve replacement or transcatheter aortic valve implantation as the only available therapeutic interventions. For the majority of symptomatic patients with severe aortic stenosis, aortic valve intervention is a widely accepted approach34. However, for other groups including asymptomatic patients with severe aortic stenosis or symptomatic patients with moderate aortic stenosis, the evidence remains less clear. In 1990, Dr Eugene Braunwald stated that “operative treatment is the most common cause of sudden death in asymptomatic patients with aortic stenosis”5. Whilst likely accurate for that era, improvements in technology, surgical approaches, perioperative care, and, importantly, the advent of transcatheter aortic valve implantation have improved outcomes following valve intervention. Further, our understanding of the adverse left ventricular remodelling that develops whilst patients await symptom development and valve intervention has improved. Irreversible cardiac damage occurs frequently and is strongly associated with poor outcomes in the years and decades that follow aortic valve intervention678. A focus on trying to improve these longer-term outcomes in an era of minimally invasive and low-risk valve interventions has led to interest in extending indications for aortic valve intervention beyond symptomatic patients with severe aortic stenosis. This may include asymptomatic patients with severe aortic stenosis or symptomatic patients with moderate aortic stenosis, in the belief that the long-term outcomes of these patients might be improved by valve intervention. This review examines current evidence concerning the timing of aortic valve replacement, with a particular focus on transcatheter aortic valve implantation, and incorporates recent trial data to provide a comprehensive assessment of optimal intervention strategies across the spectrum of patients with aortic stenosis.
The rationale for watchful waiting
For decades, “watchful waiting” for the onset of symptoms related to severe aortic stenosis before proceeding to aortic valve intervention has been the recommended strategy for most patients with aortic stenosis. This pathway followed Braunwald and Ross’ observation over 50 years ago that patients with aortic stenosis experience a prolonged asymptomatic phase when prognosis remains favourable, followed by a rapid increase in short-term mortality heralded by the onset of symptoms9. Evidence to support this view was based upon retrospective post mortem data with a mixture of bicuspid and rheumatic valve disease, and a mean age at death of 63 years. This would be viewed as modest-quality evidence by modern standards, but their findings have been repeatedly validated in subsequent observational series101112. These cumulative data, confirming that approximately 50% of symptomatic patients die within 3 years without intervention, underpin consistent guideline recommendations concerning the timing of aortic valve intervention in those with symptomatic severe aortic stenosis34; it remains unlikely that a randomised controlled trial will be undertaken to confirm this recommendation.
Further studies have substantiated the prolonged asymptomatic phase of aortic stenosis131415, confirming that rates of sudden cardiac death in the short term, the most feared complication of watchful waiting, are low at around 0.65% per year13. This contrasts with contemporary registries that report a 1-2% procedural mortality for both transcatheter and isolated surgical aortic valve intervention16. Longer-term consequences associated with a prosthetic valve (including infective endocarditis, thrombosis, and structural valve degeneration) should also be considered. Competing risks of death are an important factor, as patients may undergo the discomfort and hospitalisation for a major procedure yet die from a non-aortic stenosis-related condition and never experience symptomatic or prognostic benefit from aortic valve intervention. Therefore, whilst nearly all asymptomatic patients with severe aortic stenosis develop symptoms warranting valve intervention within 5 years, this may be a valuable period associated with good quality of life in patients who are frequently elderly, frail, and comorbid.
Potential benefits of early valve intervention
When assessing a patient with aortic stenosis, cardiologists will generally consider whether intervention will either improve symptoms and quality of life or alter prognosis. For patients with typical symptoms, the clinical approach is reasonably straightforward since aortic valve intervention will provide both symptomatic benefit and an improved prognosis. In asymptomatic patients, the arguments are less straightforward since it is difficult to improve the symptomatic status of an asymptomatic individual, particularly if they are about to undergo a major intervention. However, recent data have demonstrated that adverse remodelling occurs whilst patients wait for valve intervention and is associated with the adverse outcomes of heart failure and death in the ensuing years781718192021. The rationale for earlier intervention in asymptomatic patients with severe aortic stenosis therefore rests on the ability of this approach to improve long-term outcomes.
Pathophysiology and natural history of aortic stenosis
Aortic stenosis is no longer viewed as a passive degenerative process but rather as an active disease characterised by lipid accumulation, inflammatory activation, and progressive fibrocalcific remodelling of the aortic valve leaflets2223. Progressive narrowing of the aortic valve generates increasing pressure overload on the left ventricle, which triggers a cascade of compensatory remodelling and hypertrophy to maintain wall stress and preserve cardiac contractility and performance, often for many years. However, this compensatory process is inherently finite and eventually decompensates, as patients transition from left ventricular hypertrophy to heart failure, symptom development, and major adverse clinical events (Figure 1)2224.
The transition from compensatory hypertrophy to heart failure involves complex interactions between myocyte injury, apoptosis, and myofibroblast activation2526. This process results in extracellular matrix expansion and reactive interstitial and replacement fibrosis222427. Reactive interstitial fibrosis occurs diffusely throughout the myocardium following increased myofibroblast activation and collagen deposition24. This pattern is observed in earlier disease stages and may regress following valve intervention28. In contrast, replacement fibrosis is more focally distributed and occurs later in the disease course. Once established, this irreversible form of fibrosis progresses rapidly until aortic valve replacement is performed. The burden of replacement fibrosis that a patient develops whilst waiting for valve replacement therefore persists into the long term; this is of importance because this has been consistently and closely associated with an increased risk of heart failure and cardiovascular and all-cause mortality following aortic valve intervention8242529303132. This provides further rationale for early interventional strategies on the basis that these will reduce the burden of myocardial fibrosis that develops in patients with aortic stenosis, which in turn may improve longer-term outcomes.
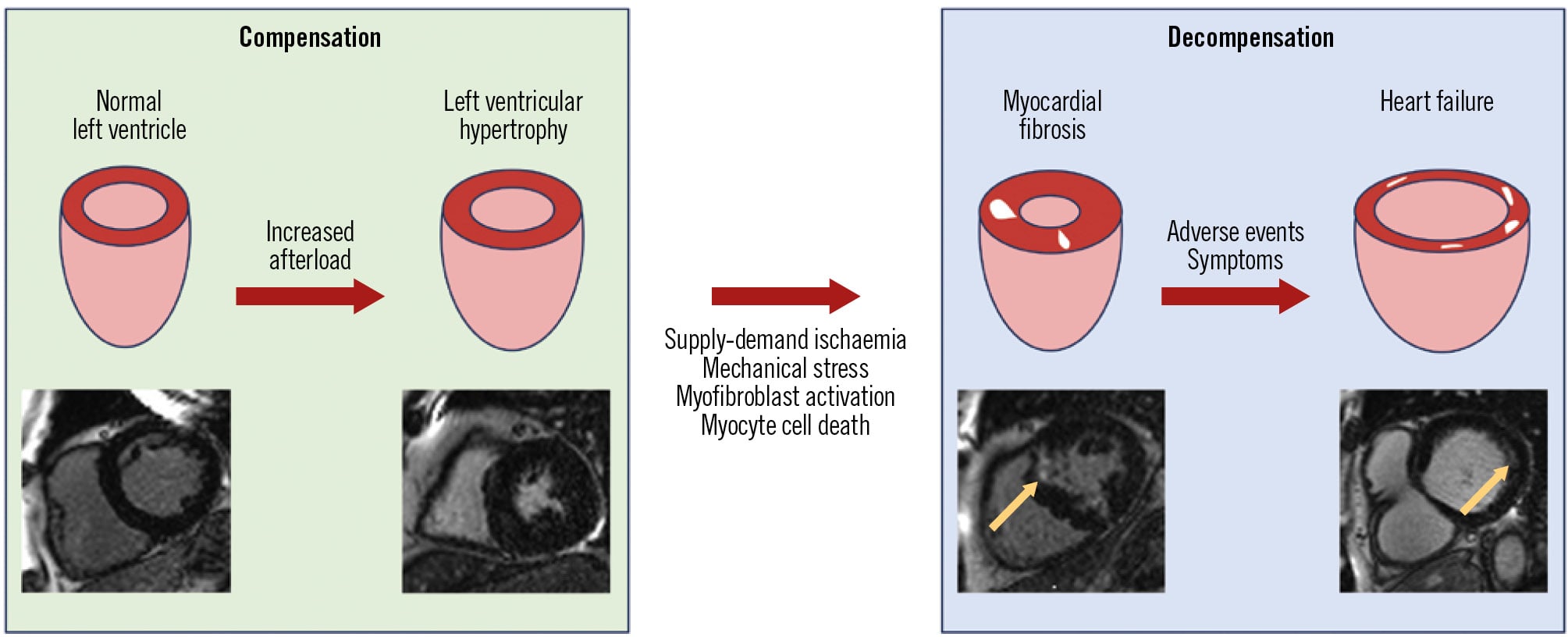
Figure 1. Left ventricular remodelling in aortic stenosis. Progressive obstruction of blood flow through the stiff, thickened valve in aortic stenosis increases afterload and wall stress on the left ventricular myocardium, which becomes hypertrophied in order to maintain cardiac contractility. However, in response to myocyte apoptosis, ischaemia, direct wall stress, and the activation of myofibroblasts through profibrotic mediators (including angiotensin II and transforming growth factor-beta), fibrosis develops (white regions within the left ventricle schematic), which can be visualised using late gadolinium enhancement on cardiac magnetic resonance (yellow arrows). Increased myocardial fibrosis leads to left ventricular systolic and diastolic impairment, heart failure, and adverse events.
Established indications for aortic valve intervention
Symptoms due to severe aortic stenosis are considered an indicator of left ventricular decompensation and indicate poor prognosis without intervention, as initially described by Braunwald and Ross in 19689 and subsequently confirmed in a post hoc analysis of the 358 symptomatic patients with severe aortic stenosis deemed unsuitable for surgery in the PARTNER I randomised controlled trial33. This analysis demonstrated 50% mortality within one year in patients receiving routine care, including balloon aortic valvuloplasty, compared with 31% of those undergoing transcatheter aortic valve implantation (hazard ratio 1.82, 95% confidence interval: 1.35-2.50; p<0.001). Current international guidelines from the American College of Cardiology/American Heart Association and European Society of Cardiology give Class I recommendations for valve intervention in symptomatic patients with severe aortic stenosis (Table 1)34.
Implementation of these guidelines in clinical practice is nevertheless challenging. The classical symptom triad in aortic stenosis – exertional dyspnoea, angina, and syncope – is commonly experienced by older adults for other reasons. False attribution of these coincidental symptoms to aortic stenosis may result in major intervention with no clinical improvement in how the patient feels and leave potential alternative diagnoses unexplored. Conversely, physical inactivity due to sarcopaenia, functional deconditioning, and medical comorbidities can mask exertional symptoms until the development of critical aortic stenosis. These clinical challenges underscore the need for randomised data to inform clinical practice and better tools for the risk stratification of patients who have the most to gain from valve intervention.
Left ventricular systolic impairment is the inevitable consequence of untreated progressive aortic stenosis without treatment and may occur without associated symptoms. Despite the absence of randomised clinical trial evidence, international guidelines recommend intervention in asymptomatic patients with severe aortic stenosis and reduced left ventricular ejection fraction (<50%) regardless of symptom status34. However, it is important to remember that left ventricular systolic impairment may have several underlying mechanisms, the natural history of which may not be altered by aortic valve intervention. Reduced ejection fraction caused by increased afterload is likely to improve following valve intervention in an otherwise healthy ventricle34353637383940. The same may not be true in patients with extensive myocardial infarction, coexistent cardiac amyloidosis, or dilated cardiomyopathy, where the mechanism of left ventricular dysfunction is independent of the valve disease.
Table 1. Key guideline recommendations for aortic valve replacement in patients with severe aortic stenosis.
| ESC/EACTS 2025 guidelines3 | ACC/AHA 2020 guidelines4 | |||
|---|---|---|---|---|
| Class (Level of Evidence) | Indications for AVR | Class (Level of Evidence) | Indications for AVR | |
| Symptomatic severe aortic stenosis | I (B) | High-gradient severe aortic stenosis (mean gradient ≥40 mmHg, Vmax ≥4.0 m/s, and AVA ≤1.0 cm2 or ≤0.6 cm2/m2) | I (A) | High-gradient severe aortic stenosis |
| I (B) | Low-flow, low-gradient severe aortic stenosis (stroke volume index ≤35 mL/m2, mean gradient <40 mmHg) with LVEF <50% | I (B) | Low-flow, low-gradient severe aortic stenosis with LVEF <50% | |
| II (B) | Confirmed low-flow, low-gradient severe aortic stenosis with LVEF >50% | II (B) | Low-flow, low-gradient severe aortic stenosis with LVEF >50% | |
| Asymptomatic severe aortic stenosis | I (B) | LVEF <50% with no identifiable cause other than aortic stenosis | I (B) | LVEF <50% with no identifiable cause other than aortic stenosis |
| II (A) | High-gradient severe aortic stenosis, as an alternative to close active surveillance if procedural risk is low | I (B) | Indication for concomitant cardiac surgery | |
| II (C) | >20 mmHg fall in systolic blood pressure during exercise testing | I (A) | Symptoms during exercise testing | |
| II (B) | Very severe aortic stenosis (Vmax >5 m/s or mean gradient ≥60 mmHg), or an increase in Vmax ≥0.3 m/s per annum, or BNP levels >3x the upper limit of normal, or LVEF <55% without any other cause | II (A) | >10 mmHg fall in systolic blood pressure during exercise testing | |
| II (A) | Low surgical risk and very severe aortic stenosis (Vmax >5 m/s), or an increase in Vmax ≥0.3 m/s per annum, or BNP levels >3x the upper limit of normal | |||
| AVA: aortic valve area; AVR: aortic valve replacement; BNP: B-type natriuretic peptide; cm: centimetres; EACTS: European Society of Cardio-Thoracic Surgery; ESC: European Society of Cardiology; LVEF: left ventricular ejection fraction; m: metres; m/s: metres per second; mL: millilitres; mmHg: millimetres of mercury; Vmax: aortic valve peak velocity | ||||
Conditional indications for intervention in asymptomatic patients
Current guidelines provide several conditional indications for intervention in asymptomatic patients with severe aortic stenosis and normal left ventricular systolic function, although these are based upon observational data rather than randomised controlled trials. These include very severe aortic stenosis (aortic valve peak velocity >5.0 m/s), abnormal exercise testing with associated symptoms or abnormal blood pressure response, rapid disease progression (an increase in aortic valve peak velocity>0.3 m/s per annum) associated with severe valve calcification on computed tomography, or markedly elevated natriuretic peptides with no other cause34.
Exercise testing
International guidelines recommend intervention for asymptomatic patients with severe aortic stenosis who develop typical symptoms during exercise testing or demonstrate a fall in systolic blood pressure at peak exercise34. This recommendation is based upon a meta-analysis of four non-randomised trials indicating that a “normal” exercise test was not associated with any sudden cardiac death during the 11- to 15-month follow-up. However, many patients with aortic stenosis are unable to complete such tests because of non-cardiac functional limitations. Furthermore, exercise test interpretation is challenging and subjective without clear thresholds, and “normal” responses are difficult to define – even elite athletes typically develop dyspnoea at some point during an exercise test. While a normal exercise test has a high negative predictive accuracy (ranging from 0.79-1.00), suggesting that these patients can be managed conservatively, the specificity of a positive test in predicting the development of spontaneous symptoms or experiencing a major adverse cardiac event is low (0.60-0.78)414243444546. Notably, ST-segment depression or an abnormal blood pressure response has not been proven to improve the accuracy of exercise testing in patients with aortic stenosis44.
Very severe or progressive aortic stenosis
Asymptomatic patients with critical aortic stenosis (aortic valve peak velocity >5.0 m/s) have a poor prognosis that is similar to those with symptoms, and registry data report a twofold increase in all-cause mortality compared to patients with velocities <5.0 m/s13. The Randomized Comparison of Early Surgery Versus Conventional Treatment in Very Severe Aortic Stenosis (RECOVERY) trial demonstrated reduced operative mortality and cardiovascular death following early surgical aortic valve replacement versus watchful waiting in 145 asymptomatic patients with very severe disease (mean aortic valve peak velocity 5.1 m/s)47. However, this study recruited a young cohort (mean age 64 years) with predominantly bicuspid valves (61%) and was restricted to surgical aortic valve replacement. Whilst these findings may be not directly extrapolated to the general population suitable for transcatheter aortic valve implantation, the trial does offer support for the current guideline recommendations (Table 2).
Haemodynamic progression is a key feature of the natural history of aortic stenosis with an average annual increase in aortic valve peak velocity of 0.15 m/s14484950. However, there is considerable variation between patients in the rate of disease progression, with a minority progressing very quickly towards critical aortic stenosis and earlier development of symptoms and adverse events. Severe aortic valve calcification on computed tomography correlates with faster progression and increased mortality in observational studies, and guidelines recommend considering intervention in asymptomatic patients with severe aortic stenosis and severe calcification and an increase in aortic valve peak velocity>0.3 m/s per annum in low-risk patients345152. However, interpreting a 0.3 m/s increase in aortic valve peak velocity between two different scans and operators can be challenging in clinical practice. The scan-rescan repeatability of aortic valve peak velocity assessments is around 0.2 to 0.3 m/s in patients with severe aortic stenosis (mean difference 5%, limits of agreement –7% to 17%)53; therefore, differentiating rapid progression from the natural variation in echocardiographic measurements is difficult.
Table 2. Summary of randomised trials assessing the timing of aortic valve intervention in patients with aortic stenosis.
| Banovic et al, 20245556 AVATAR | Kang et al, 202047 RECOVERY | Loganath et al, 202458 EVOLVED | Généreux et al, 202466 EARLY TAVR | Van Mieghem et al, 202578 TAVR UNLOAD | |
|---|---|---|---|---|---|
| Aortic stenosis severity | Severe | Severe | Severe | Severe | Moderate |
| Key inclusion criteria | Age ≥18 years Asymptomatic (without reported symptoms, or anginal chest pain, dizziness or syncope during exercise testing) AVA ≤1 cm2 or iAVA ≤0.6 cm2/m2 or Vmax ≥4.0 m/s or MG ≥40 mmHg LVEF >50% | Age 20-80 years Asymptomatic AVA ≤0.75 cm2 and either Vmax ≥4.5 m/s or MG ≥50 mmHg | Aged ≥18 years Asymptomatic LVEF >50% Vmax ≥4.0 m/s or iAVA <0.6 cm2/m2 and Vmax ≥3.5 m/s | Age ≥65 years LVEF ≥50% AVA ≤1 cm2 or iAVA ≤0.6 cm2/m2 and Vmax ≥4.0 m/s or MG ≥40 mmHg Asymptomatic (confirmed by exercise testing) | Symptomatic LVEF <50% NT-proBNP >1,500 pg/mL or hospitalisation for heart failure within 12 months MG ≥20 mmHg and <40 mmHg at rest and AVA >1.0 cm2 and ≤1.5 cm2 at rest, or MG ≥20 mmHg and <40 mmHg at rest and AVA ≤1.0 cm2 at rest but >1.0 cm2 by low-dose dobutamine stress echo |
| Transcatheter aortic valve implantation | Early intervention: 0 (0) Conservative: 0 (0) | Early intervention: 0 (0) Conservative: 1 (1) | Early intervention: 26 (23) Conservative: 38 (34) | Early intervention: 444 (98) Conservative: 388 (87) | Early intervention: 88 (99) Conservative: 38 (43) |
| Surgical aortic valve replacement | Early intervention: 72 (92) Conservative: 25 (32) | Early intervention: 72 (100) Conservative: 52 (70) | Early intervention: 80 (71) Conservative: 47 (42) | Early intervention: 0 (0) Conservative: 7 (2) | Early intervention: 1 (1) Conservative: 0 (0) |
| Mean age, years | 67.0 | 64.5 | 73.4 | 75.8 | 77.4 |
| Female sex | 43% | 51% | 28% | 31% | 21% |
| Mean gradient, mmHg | Early intervention: 51 (45-58) Conservative: 50 (43-58) | Early intervention: 64±14 Conservative: 63±12 | 45.1±10.8 | 46.9±10.3 | 18.8±5.9 |
| Bicuspid aortic valve disease | 14% | 61% | 29% (determined by CMR) | 8.4% | Not reported |
| Left ventricular ejection fraction, % | Early intervention: 70 (65-76) Conservative: 69 (63-75) | Early intervention: 65±5 Conservative: 65±4 | 68±8 | 67±6 | 39±9 |
| Study locations | 9 centres: Europe | 4 centres: Republic of Korea | 24 centres: United Kingdom and Australia | 74 centres: USA and Canada | 66 centres: USA, the Netherlands, and Austria |
| Median follow-up, months | 63 | 73 | 42 | 46 | 23 |
| Time to early intervention, days | 55 (36-79) | 23 (10-36) | 152 (103-243) | 14 (9-24) | 13 (7-15) |
| Time to intervention in surveillance arm, days | 476 (226-1,098) | 700 (277-1,469) | 614 (346-1,277) | 333 (150-591) | 360 (180-600) |
| Primary endpoint | All-cause mortality or MACE composed of acute myocardial infarction, stroke, and unplanned heart failure hospitalisation needing intravenous treatment | Operative mortality (during or within 30 days of surgery) or cardiac mortality during entire follow-up (minimum of 4 years) | All-cause mortality and unplanned aortic stenosis-related hospitalisation | All-cause death, stroke and unplanned cardiovascular hospitalisation | Hierarchical occurrence of (1) all-cause death; (2) disabling stroke; (3) disease-related hospitalisations and heart failure hospitalisation equivalents; (4) change from baseline in the KCCQ-OSS |
| Key findings | Significantly lower incidence of the primary endpoint with early intervention compared to clinical surveillance (23.1% vs 46.8%, HR 0.42, 95% CI: 0.24-0.73; p=0.002) Lower rate of mortality with SAVR | Significantly lower incidence of the primary endpoint with early intervention compared to clinical surveillance (1% vs 15%, HR 0.09, 95% CI: 0.01-0.67; p=0.003) Lower rate of mortality with early SAVR | No significant difference in the incidence of the primary endpoint No difference in mortality Significantly fewer unplanned aortic stenosis-related hospitalisations with early intervention compared with conservative management (6.2% vs 17.1%, HR 0.42, 95% CI: 0.24-0.73) | Significantly lower incidence of the primary endpoint with early intervention compared to clinical surveillance (26.8% vs 45.3%, HR 0.50, 95% CI: 0.40-0.63; p<0.0001) No difference in mortality | No significant difference in the incidence of the hierarchical primary endpoint Significant improvement in KCCQ-OSS with early intervention compared with clinical surveillance (12.8±21.9 vs 3.2±22.8; p=0.02) |
| Data are presented as n (%), mean±SD or median (interquartile range), as reported. AVA: aortic valve area; CI: confidence interval; cm: centimetres; CMR: cardiac magnetic resonance; HR: hazard ratio; iAVA: indexed aortic valve area; KCCQ-OSS: Kansas City Cardiomyopathy Questionnaire overall summary score; LVEF: left ventricular ejection fraction; m: metres; MACE: major adverse cardiovascular events; MG: mean transvalvular gradient; mmHg: millimetres of mercury; NT-proBNP: N-terminal pro-B-type natriuretic peptide; s: seconds; SAVR: surgical aortic valve replacement; SD: standard deviation; Vmax: aortic valve peak velocity | |||||
Biomarkers
Previous studies have shown that N-terminal pro-B-type natriuretic peptide concentrations correlate with indices of adverse left ventricular remodelling, earlier symptom onset, and inferior outcomes following intervention36. These observational findings underpin current guideline recommendations that intervention should be considered in asymptomatic patients with severe aortic stenosis and markedly elevated serum N-terminal pro-B-type natriuretic peptide concentrations34. However, while post hoc data from subsequent randomised trials have confirmed the association between high N-terminal pro-B-type natriuretic peptide concentrations and adverse clinical events, this did not translate into improved outcomes with earlier transcatheter aortic valve implantation when examined in the Evaluation of Transcatheter Aortic Valve Replacement Compared to Surveillance for Patients with Asymptomatic Severe Aortic Stenosis (EARLY TAVR) trial54. This may reflect the non-specific nature of N-terminal pro-B-type natriuretic peptide which can be affected by multiple factors beyond aortic stenosis.
Recent randomised trials in asymptomatic patients with severe aortic stenosis
Based upon the results of recently published randomised controlled trials, the most recent iteration of the European Society of Cardiology and European Association of Cardio-Thoracic Surgery guidelines have given a new Class IIa recommendation with Level of Evidence A that intervention should be considered in asymptomatic patients with severe, high-gradient aortic stenosis and normal left ventricular ejection fraction as an alternative to close active surveillance, if the procedural risk is low3. Two of these trials have been performed in patients undergoing surgical aortic valve replacement rather than transcatheter aortic valve implantation. Their results are of potential relevance to the timing of transcatheter aortic valve implantation if we accept that outcomes are likely to be similar with the two methods of intervention. The RECOVERY trial in patients with critical asymptomatic aortic stenosis has already been discussed. The Aortic Valve Replacement Versus Conservative Treatment in Asymptomatic Severe Aortic Stenosis (AVATAR) trial randomised 157 asymptomatic patients (mean age 67 years, 14% with bicuspid valves) with severe aortic stenosis (median aortic valve peak velocity 4.5 m/s) to surgical aortic valve replacement or conservative treatment and demonstrated a reduction in all-cause, though not cardiovascular, mortality at 5-year follow-up (Table 2)5556.
The EVOLVED trial
The Early Valve Replacement Guided by Biomarkers of Left Ventricular Decompensation in Asymptomatic Patients with Severe Aortic Stenosis (EVOLVED) trial enrolled a population (n=224) of asymptomatic patients with severe aortic stenosis, electrocardiographic left ventricular hypertrophy, and elevated high-sensitivity cardiac troponin I, with myocardial fibrosis confirmed on cardiac magnetic resonance imaging (Table 2)57. The hypothesis was that early intervention might improve clinical outcomes in this study population enriched for high cardiac risk. Eligible patients were randomised to early valve intervention or guideline-directed conservative management across 24 participating sites in the United Kingdom and Australia. The mode of intervention was determined by the local Heart Team at individual participating sites, reflecting real-world practice. Two-thirds of patients underwent surgical aortic valve replacement, whilst one-third underwent transcatheter aortic valve implantation, 97% via the transfemoral approach. The trial found that earlier aortic valve intervention had no demonstrable impact on the combined primary endpoint of all-cause mortality or unplanned aortic stenosis-related hospitalisation when compared with guideline-directed conservative management. However, early intervention resulted in fewer unplanned aortic stenosis-related hospitalisations compared with guideline-directed conservative management, and the burden of heart failure symptoms at 12 months was higher in patients allocated to conservative care58. These findings remain important for an often elderly population in whom the avoidance of limiting symptoms and hospital admissions may be the primary treatment goal.
These results need to be assessed in light of significant trial limitations. Importantly, the rate of transcatheter aortic valve implantation was higher as a crossover treatment in the guideline-directed conservative management arm than the early intervention arm (45% and 25%, respectively). This likely reflects improved access to transcatheter aortic valve implantation during the course of the trial and the need for urgent intervention following unplanned aortic stenosis-related hospitalisations in patients who were too unwell for surgical aortic valve replacement. This observation limits generalisation of the trial findings to all patients being considered for transcatheter aortic valve implantation, and post hoc analysis of this group would be of interest. Whilst the 15-month difference in time to intervention between study arms in EVOLVED was the longest of all 4 randomised trials addressing this question, the median time to intervention in the early intervention arm was 5.5 months. Indeed, 6 patients randomised to early intervention died before their procedure. Whilst this reflects the real-world waiting time for valve intervention in many healthcare systems59606162, concerns have been raised that this delay is too long636465.
The EARLY TAVR trial
EARLY TAVR is the largest randomised controlled trial in asymptomatic patients with severe aortic stenosis and normal left ventricular systolic function (Table 2)66. This multicentre study randomised 901 patients across 75 centres in the USA and Canada to either early transfemoral transcatheter aortic valve implantation with the balloon-expandable SAPIEN 3 or SAPIEN 3 Ultra valve (both Edwards Lifesciences), or guideline-directed clinical surveillance. Early transcatheter aortic valve implantation was associated with a reduction in the primary composite endpoint of death, stroke, or unplanned cardiovascular hospitalisation (26.8% vs 45.3%, hazard ratio 0.50, 95% confidence interval: 0.40-0.63; p<0.001).
The primary outcome result of EARLY TAVR has led to calls for changes in international guidelines and a strategy of early intervention for most asymptomatic patients with severe aortic stenosis65. However, the impact of early intervention on the primary outcome was principally driven by unplanned cardiovascular hospitalisations, with no influence on mortality. An important and unique aspect of the EARLY TAVR trial’s primary endpoint was that any transcatheter aortic valve implantation within 6 months of randomisation, even a planned intervention in a stable patient, was considered a primary outcome event. This scenario arose in 116 patients (26%) in the clinical surveillance group, whilst it did not occur in the early intervention group. Given that patients in the open-label EARLY TAVR trial underwent transcatheter aortic valve implantation work-up at the time of enrolment and prior to randomisation, it has been suggested that subtraction anxiety may have contributed to this high early crossover rate and these primary outcome events. Of reassurance, a post hoc analysis has shown that early transcatheter aortic valve implantation was associated with a reduction in an endpoint of major adverse cardiovascular events comprising death, heart failure hospitalisation, and stroke66. Finally, even though the mean age of the study participants (76 years) was representative of a general aortic stenosis population, the low average Society of Thoracic Surgeons score (1.8%) suggests this was a relatively low-risk population, many of whom would have been suitable for surgical aortic valve replacement.
Meta-analysis of randomised trials in asymptomatic patients with severe aortic stenosis
A recent study-level meta-analysis incorporating data from the 4 randomised controlled trials in asymptomatic patients with severe aortic stenosis (including EARLY TAVR and EVOLVED) provides important insights concerning the overall evidence base67. Compared with clinical surveillance, early aortic valve intervention via surgical or transcatheter techniques was associated with a reduction in unplanned cardiovascular or heart failure hospitalisation but no difference in all-cause or cardiovascular mortality. Intriguingly, there was also a reduction in the incidence of clinical stroke – a paradox given the known risk of periprocedural stroke associated with aortic valve intervention, which requires further exploration in dedicated studies.
However, there are important differences between the trials pooled in the meta-analysis that warrant consideration, many of which are detailed in Table 267. The most obvious is the mode of intervention. Whilst all 4 trials compared an early intervention strategy with clinical surveillance, RECOVERY and AVATAR focused on surgical aortic valve replacement, while EARLY TAVR assessed transfemoral transcatheter aortic valve implantation with a balloon-expandable valve alone – only in EVOLVED did the local heart valve team pragmatically select between surgical and transcatheter aortic valve intervention47555866. Whilst there was a significant interaction between the mode of intervention and all-cause mortality, this likely reflects differing trial enrolment criteria rather than the specific procedure. Accordingly, it is worth highlighting that the mean age of participants in the RECOVERY trial was 64 years, with bicuspid aortic valve disease in 61% and a mean aortic valve peak velocity of 5.1 m/s, in comparison to EARLY TAVR, where the mean age was 76 years, 8% had a bicuspid aortic valve, and the mean aortic valve peak velocity was 4.3 m/s4766.
The trials were also conducted across different healthcare systems. As a result, there were large differences in the time to early intervention and both time to crossover and time from referral to intervention in the clinical surveillance arms. Specifically, the mean times from randomisation to valve intervention in those who crossed over from the clinical surveillance arms were 330 days, 476 days, 614 days, and 700 days in EARLY TAVR, AVATAR, EVOLVED, and RECOVERY, respectively47555866. In these patients, the time to intervention from referral was 32 days in EARLY TAVR compared with 100 days in EVOLVED and 123 days in AVATAR; these data are not available for RECOVERY. It is therefore possible that these differences contributed to the absence of a mortality difference in EARLY TAVR compared with RECOVERY and AVATAR, alongside other significant confounders, such as age, disease severity, valve morphology, and intervention strategy. This uncertainty can only be resolved with individual patient-level meta-analyses.
Nonetheless, the findings suggest that while early intervention may prevent emergency hospitalisation and the development of symptoms, survival benefit remains uncertain except in the highest-risk cohort with the most severe stenosis. Therefore, based on current evidence, the main reason to consider early intervention in asymptomatic patients with severe aortic stenosis would appear to be the prevention of heart failure in this at-risk population. There is likely to be important variation in how patients decide to proceed. Some will not wish to undergo a major heart valve procedure when they are currently free from symptoms without the clear prospect of living longer. Others may prefer to undergo early intervention in order to give them the best chance of remaining healthy and asymptomatic for as long as possible. In this context, detailed patient-centred discussions and decisions will be required.
Transcatheter aortic valve implantation in patients with moderate aortic stenosis
Although no guideline recommendations exist for transcatheter or surgical aortic valve intervention in patients with moderate aortic stenosis, it is recognised that these patients may also experience symptoms and that survival outcomes in moderate aortic stenosis patients are similar to those in severe aortic stenosis patients in large observational studies686970. However, distinguishing between symptoms attributable to valve disease versus those arising from frequently encountered comorbidities, including coronary artery disease and chronic lung disease, presents a significant clinical challenge. Furthermore, patients with moderate aortic stenosis demonstrate survival outcomes that are similar to those with severe aortic stenosis in large observational studies717273. In these observational studies, this relationship is sustained after adjustment for potential confounders, including hypertension, diabetes, coronary artery disease, chronic kidney disease, and medication use. However, whether this association is truly related to aortic stenosis or comorbidity, and therefore whether it is modifiable with the timing of aortic valve replacement, will only become evident with randomised controlled trials. It is perhaps worth noting that other observational studies have demonstrated that patients with aortic sclerosis also have an adverse prognosis, an association almost certainly related to comorbidity, and in particular their associated coronary atherosclerosis7475. Few would consider aortic valve intervention likely to be of benefit in these patients. Nonetheless, the extent of adverse left ventricular remodelling (including the presence of replacement fibrosis) is similar in patients with moderate and severe aortic stenosis76.
In patients with both heart failure and moderate aortic stenosis, the negative impact of symptoms and reduced left ventricular systolic function on clinical outcomes is well described. Correction of valvular impedance in this population in order to reduce left ventricular afterload and unload the failing left ventricle is an attractive hypothesis7778. To date, the Transcatheter Aortic Valve Replacement to Unload the Left Ventricle in Patients with Advanced Heart Failure (TAVR UNLOAD) trial provides the only randomised data in this setting, enrolling 178 patients at 66 institutions in the USA, the Netherlands, and Austria. The patients were randomised to transfemoral transcatheter aortic valve implantation using the balloon-expandable SAPIEN 3 valve or clinical surveillance (Table 2)78. Eligible patients were symptomatic (New York Heart Association Class II-IV) with reduced left ventricular ejection fraction (20-50%) despite guideline-directed medical therapy for at least 1 month. In the early intervention arm, 99% underwent transcatheter aortic valve implantation at a median of 13 days following randomisation, whereas in the clinical surveillance group, 43% underwent transcatheter aortic valve implantation at a median of 12 months, mostly (92%) due to progression to severe aortic stenosis. This underscores the fact that moderate aortic stenosis can progress rapidly and that close surveillance is essential.
Although transcatheter aortic valve implantation was not superior to clinical surveillance in this population (win ratio for the primary composite endpoint [assessed at the longest common follow-up for each patient pair] 1.31, 95% confidence interval: 0.91-1.88; p=0.14), enrolment targets were not met, prompting multiple protocol amendments, iterative assumptions affecting sample size calculations, and adjustments to outcome assessment timepoints. The authors have acknowledged that the study was underpowered and that further trials are required to confirm their findings. The results of ongoing trials − Management of Moderate Aortic Stenosis by Clinical Surveillance or TAVR (PROGRESS; ClinicalTrials.gov: NCT04889872) and the Evolut EXPAND TAVR II Pivotal Trial (NCT05149755) − are therefore eagerly anticipated (Table 3). However, to date, no data exist to justify pre-emptive transcatheter aortic valve implantation in symptomatic patients with moderate aortic stenosis, heart failure, and reduced left ventricular ejection fraction.
Table 3. Active randomised controlled trials on the timing of aortic valve intervention in patients with aortic stenosis.
| EASY-AS | DANAVR | PROGRESS | EXPAND TAVR II | |
|---|---|---|---|---|
| ClinicalTrials.gov registration | NCT04204915 | NCT03972644 | NCT04889872 | NCT05149755 |
| Recruitment target | 2,844 | 1,700 | 2,250 | 650 |
| Estimated completion | April 2031 | September 2029 | June 2029 | February 2026 |
| Trial intervention | Early valve intervention (SAVR or TAVI) versus expectant management | Early valve intervention (SAVR or TAVI) versus watchful waiting | Early TAVI (SAPIEN 3a, SAPIEN 3 Ultraa, or SAPIEN 3 Ultra RESILIAa) versus clinical surveillance | Early TAVI (Evolut PRO+b or Evolut FXb) & GDMT versus GDMT & guideline-directed management |
| Key inclusion criteria | Age >18 years Asymptomatic Severe AS (Vmax >4 m/s or MG >40 mmHg with AVA <1.0 cm2 or Vmax 3.5-3.9 m/s and MG <40 mmHg with AVA <1.0 cm2 and high sex-specific CT calcium score) Suitable for SAVR or TAVI (deemed by treating cardiologist) LVEF >50% | Age >18 and <85 years Asymptomatic Severe AS (AVA <1 cm2 and Vmax >3.5 m/s) Evidence of increased left ventricular filling pressures by any of the following: LAVi >34 mL/m2 E/e’ ratio >13 NT-proBNP >3x the upper limit of normal GLS >–15.5% | Age >65 years Moderate AS Symptoms or evidence of cardiac damage/dysfunction Suitable for transfemoral TAVI LVEF >20% | Age >65 years Moderate AS Suitable for transfemoral TAVI LVEF >20% Any of the following: Symptoms Reduced functional capacity Heart failure event in the previous year NT-proBNP >600 pg/mL Atrial fibrillation High CT calcium score |
| Primary endpoint | Cardiovascular death and hospitalisation for heart failure | All-cause mortality | All-cause death and heart failure hospitalisation or event | All-cause mortality, heart failure hospitalisation or event, or medical instability leading to SAVR or reintervention |
| Data presented as n (%), mean±SD or median (interquartile interval) as reported. aBy Edwards Lifesciences; bby Medtronic. AS: aortic stenosis; AVA: aortic valve area; cm: centimetres; CT: computed tomography; E: early diastolic peak mitral inflow velocity; e’: early mitral annulus diastolic velocity; GDMT: guideline-directed medical therapy; GLS: global longitudinal strain; LAVi: indexed left atrial volume; LVEF: left ventricular ejection fraction; m: metres; MG: mean transvalvular gradient; mL: millilitres; mmHg: millimetres of mercury; NT-proBNP: N-terminal pro-B-type natriuretic peptide; pg: picograms; s: seconds; SAVR: surgical aortic valve replacement; SD: standard deviation; TAVI: transcatheter aortic valve implantation; Vmax: aortic valve peak velocity | ||||
Lifelong management
The potential benefits of earlier aortic valve intervention need to be balanced against the short- and long-term risks of intervention, including prosthetic valve infective endocarditis, thromboembolic complications, difficulties with future coronary access, and structural valve deterioration requiring repeat intervention68. Recent 10-year follow-up data from the Nordic Aortic Valve Intervention (NOTION) trial demonstrate a 10% rate of valve failure in both transcatheter and surgically implanted bioprosthetic valves79, and although valve-in-valve transcatheter aortic valve implantation is feasible in both settings, there are associated risks of acute coronary obstruction, challenging future coronary access, and patient-prosthesis mismatch80. The effective orifice area of an implanted transcatheter aortic valve will decrease with successive valve-in-valve procedures, and severe patient-prosthesis mismatch is associated with increased mortality8182. These factors are of particular importance for younger patients who may potentially face multiple interventions over a lifetime. Some have argued that valve degeneration should not be an important factor when considering the timing of valve intervention in asymptomatic severe aortic stenosis, citing the fact that asymptomatic patients are likely to develop an indication for intervention within 2 years83. This assertion is based on data from the EARLY TAVR trial, in which 71.4% of patients in the clinical surveillance arm had undergone transcatheter aortic valve implantation at 2 years and 47.2% at 1 year66. These observations contrast with the EVOLVED trial, in which only 28% of patients crossed over to intervention in the first 12 months, although waiting lists differ substantially between the healthcare systems where these trials were performed58. However, a meta-analysis of observational data published before the completion of EARLY TAVR suggested that symptoms develop at a rate of 18.5% per year across the spectrum of patients with asymptomatic severe aortic stenosis84. It is unclear whether the higher rate of crossover treatment in EARLY TAVR reflects closer clinical surveillance or subtraction anxiety in patients who are prepared for intervention but randomised to clinical surveillance. Nonetheless, a substantial proportion still do not undergo intervention after 2 years; this may be valuable time for elderly patients and avoid the need for a repeat procedure in some younger patients. Further, a substantial proportion of patients may go through the discomfort, hospitalisation, and risk of aortic valve intervention without realising a symptomatic or theoretical mortality benefit. Extended follow-up of recently published trials will provide crucial data concerning valve durability, rates of repeat intervention and long-term survival, and balanced assessment of the lifetime risks and benefits of each strategy.
Special considerations
Anatomical factors
The feasibility and risk of transcatheter aortic valve implantation depends heavily on anatomical factors, including aortic root dimensions, calcification patterns, coronary height, and the feasibility of transfemoral access858687. Patients unsuitable for a transfemoral approach were excluded from EARLY TAVR66, and only 2 transcatheter procedures were performed via alternative access in EVOLVED58. Decisions concerning optimal access often come after the decision to intervene, and non-transfemoral access may be associated with a higher risk of adverse outcomes. For example, in one large meta-analysis (including 1 randomised trial and 20 observational studies), transapical transcatheter aortic valve implantation was associated with higher rates of in-hospital and 1-year mortality, major bleeding and acute kidney injury, as well as a longer hospital stay88. Regardless of the timing of intervention, pre-emptive cross-sectional imaging and Heart Team discussion are essential to assess feasibility and quantify risk in order to facilitate fully informed, personalised decision-making between patients and their clinicians.
Patient-specific factors
Decisions concerning the timing of transcatheter aortic valve implantation must be patient-centred and consider factors beyond haemodynamic severity alone. Age, frailty, comorbidities (including concomitant valve disease), life expectancy, and patient preferences all influence the risk-benefit ratio of early versus delayed intervention in individual patients17. Multiple interacting factors, including symptom burden, expectation of risks and benefits, domestic and healthcare-based support, personal obligations and responsibilities, and logistical barriers all have the potential to influence a patient’s decision to undergo aortic valve intervention89. It is also important to note that most deaths in the conservatively managed arms of RECOVERY, AVATAR, EARLY TAVR, and EVOLVED were not related to aortic stenosis4755565866, highlighting the importance of competing risks of death in this frequently elderly population. It is therefore possible that many patients undergoing earlier aortic valve intervention may experience hospitalisation and the discomfort of a major procedure with its associated risks but never derive symptomatic or prognostic benefit.
Evaluating the presence of symptoms in the cohort of elderly patients with aortic stenosis is challenging, whether due to comorbidities such as chronic obstructive pulmonary disease which may also cause dyspnoea, or the fact that many patients limit their daily activities to avoid symptoms or are unable to perform such activities because of extreme age, limited mobility, or other issues. These patients are also often incapable of exercise testing and were largely excluded from the trials. Objective assessment and risk stratification (for example, with N-terminal pro-B-type natriuretic peptide or cardiac magnetic resonance to detect mid-wall fibrosis) may be helpful, but this requires further study in dedicated trials. In the era of pragmatic and realistic medicine, it is also worth considering that older patients with limited mobility and significant comorbidity are likely to have higher competing risks of death, and arguably less to gain from an early intervention strategy. Indeed, for these patients, undergoing transcatheter aortic valve implantation may be exposing them to an unnecessary procedure if they die from a non-aortic stenosis-related cause before developing symptoms from aortic stenosis or suffering an aortic stenosis-related death.
Close clinical surveillance
The success of a clinical surveillance strategy is likely to be dependent on both the likelihood of a patient reporting the development of symptoms promptly and the healthcare system’s ability to provide rapid clinical assessment, access to early transthoracic echocardiography, and timely aortic valve intervention upon the development of symptoms or left ventricular systolic dysfunction. The former requires careful evaluation of each particular patient, while the latter involves consideration of local healthcare systems’ capacity and resource allocation. In EARLY TAVR, clinical surveillance constituted clinical and echocardiographic assessments at baseline, 1, 2, 3, and 5 years post-randomisation, and standard care in accordance with American College of Cardiology and American Heart Association guidelines466. Whilst this may be possible to replicate in routine practice, the median of 32 days from referral to intervention in patients crossing over from the clinical surveillance arm may be more challenging to deliver. Cross-sectional imaging to determine the feasibility of transcatheter aortic valve implantation, early dental assessment, and other local preparatory procedures should therefore be organised at an early stage to enable timely intervention from the point of referral. These limitations of clinical surveillance in routine practice should be considered when determining treatment pathways for individual patients and institutions.
Recommendations and future directions
Until now, many guideline-recommended indications for aortic valve intervention have been based upon observational, retrospective data with inherent risk of bias, and several have failed to demonstrate improved outcomes in subsequent randomised trials. Recent evidence with Level of Evidence A475556586667 in asymptomatic patients with severe aortic stenosis provides important data to guide clinical decisions in this patient population, and considerations influencing the timing of transcatheter aortic valve implantation in patients with aortic stenosis are provided in the Central illustration.
Symptomatic patients with severe aortic stenosis and those who are asymptomatic with left ventricular systolic dysfunction due to their valve disease should undergo prompt valve intervention.
The EARLY TAVR and EVOLVED trials suggest that most asymptomatic patients with severe aortic stenosis and normal left ventricular ejection fraction can be reassured that the risk of mortality is low while waiting for the development of symptoms or left ventricular systolic dysfunction, provided that they are watched closely. Aggregate data from the randomised controlled trials confirm that an early intervention strategy for all asymptomatic patients with severe aortic stenosis has no clear overall mortality benefit. However, there may be important considerations and subgroups of patients in whom early intervention may prevent death. For example, strict clinical surveillance and prompt intervention upon the development of symptoms may reduce sudden cardiac death, whilst data from RECOVERY suggest that younger patients with very severe aortic stenosis also derive mortality benefit. These considerations should be balanced against the risk of periprocedural complications and future events, including infective endocarditis and valve degeneration. The primary benefit of early intervention appears to be the prevention of symptoms and need for emergency heart failure hospitalisation, which itself is not benign and is associated with longer-term mortality. Long-term outcome data from the 4 randomised controlled trials will therefore be essential to truly understand the risks and benefits of each strategy.
Overall, this information requires careful discussion with patients in relation to their values and preferences, supporting a move towards personalised decision-making rather than universal early intervention. Factors supporting early intervention include acceptance of procedural risk, a desire to prevent symptoms and hospitalisations, favourable anatomy, younger age, very severe aortic stenosis (aortic valve peak velocity >5.0 m/s), myocardial fibrosis on cardiac magnetic resonance, and the ability of patients and the local healthcare system to maintain close clinical surveillance. Alternatively, factors favouring watchful waiting include lower tolerance of procedural risk, very young age (with durability concerns), extreme age with a competing risk of death, other personal responsibilities that might be disrupted by intervention, and willingness to accept the requirements of close surveillance.
Regardless of the selected strategy, all patients with moderate or severe aortic stenosis require regular clinical and echocardiographic surveillance. Education concerning the expected disease course is important to facilitate prompt symptom reporting, and healthcare services must be prepared to facilitate prompt reassessment in the event of symptoms or clinical deterioration. Given that the procedural risk of transcatheter aortic valve implantation is partly determined by anatomical characteristics, pre-emptive cross-sectional imaging once severe aortic stenosis is confirmed not only assists procedural planning but, importantly, allows accurate presentation of the risks and benefits of intervention before a decision to intervene is made. Use of biomarkers including N-terminal pro-B-type natriuretic peptide concentration, electrocardiographic evidence of left ventricular hypertrophy with strain, and advanced imaging assessments including cardiac magnetic resonance for risk stratification should also be considered in selected patients where there is persistent uncertainty concerning the optimal treatment strategy.
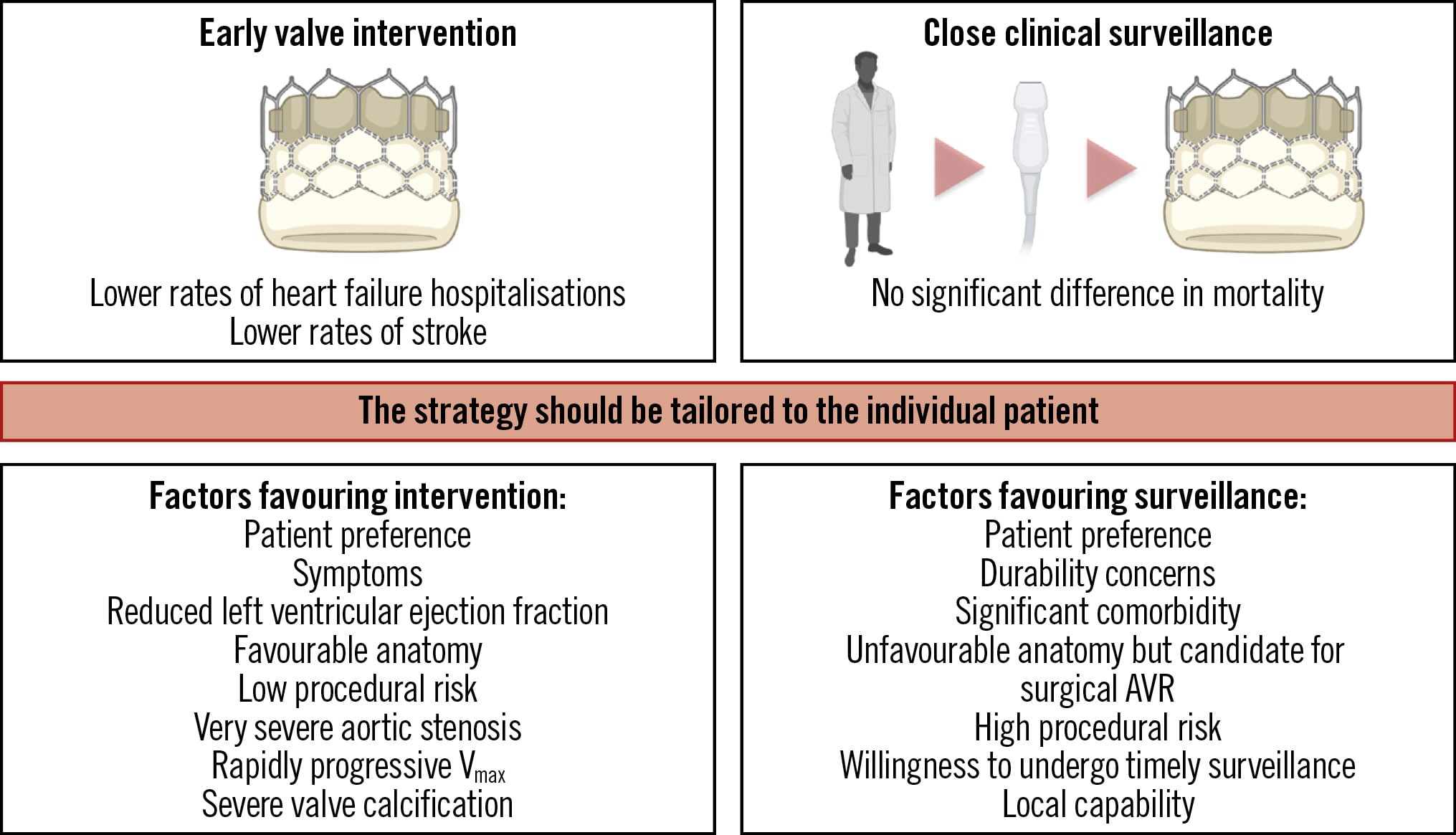
Central illustration. Management strategies in asymptomatic patients with severe aortic stenosis. Factors influencing the timing of valve intervention in aortic stenosis. AVR: aortic valve replacement; Vmax: aortic valve peak velocity
Future research priorities
The large, investigator-led Early Valve Replacement in Severe Asymptomatic Aortic Stenosis Study (EASY-AS; ClinicalTrials.gov: NCT04204915) aims to randomise over 2,000 patients to a strategy of early aortic valve intervention (either surgical aortic valve replacement or transcatheter aortic valve implantation) or conservative management with no other enrichment criteria. Similarly, the Danish National Randomized Study on Early Aortic Valve Replacement in Patients With Asymptomatic Severe Aortic Stenosis (DANAVR; NCT03972644) is actively recruiting 1,700 asymptomatic patients with severe aortic stenosis enriched by the presence of elevated left atrial filling pressures, who are randomised to early aortic valve intervention (including surgical aortic valve replacement or transcatheter aortic valve implantation) or watchful waiting. The results of these studies are eagerly anticipated90. In patients with moderate aortic stenosis, ongoing trials in symptomatic patients (PROGRESS [NCT04889872] and EXPAND TAVR II [NCT05149755]) will provide much-needed data to guide decisions in this complex patient cohort. Key details of all of these trials, including inclusion and exclusion criteria and the primary endpoint definitions, are summarised in Table 3. Individual patient-level meta-analyses of the existing aortic stenosis trials may help to determine which specific subgroups derive most benefit from early valve intervention, and extended follow-up of these trials will provide a comprehensive understanding of the longer-term risks and benefits of early valve intervention. Recent data from the Dapagliflozin in Patients Undergoing Transcatheter Aortic Valve Implantation (DapaTAVI) trial demonstrate that adjunctive dapagliflozin results in a lower incidence of all-cause death or worsening heart failure following transcatheter aortic valve implantation in patients with a history of preceding heart failure91. Whilst beyond the scope of this review, this introduces the exciting concept of medical therapy and valve intervention acting in synergy to improve reverse remodelling and to prevent the development of heart failure in these patients.
Conclusions
Transcatheter aortic valve implantation has now evolved beyond the treatment of high-risk, symptomatic patients with severe aortic stenosis. Recent randomised trials demonstrate that earlier intervention in asymptomatic severe aortic stenosis is safe, reduces hospitalisations, and prevents the development of symptoms, although mortality benefits remain uncertain. Moves towards more personalised approaches that integrate clinical characteristics, imaging data, and individual patient preferences are now essential. Future research should focus on the long-term outcomes of current trials, patients with moderate aortic stenosis, and the use of evidence-based adjunctive medical therapies alongside transcatheter aortic valve implantation.
Conflict of interest statement
M.R. Dweck has received speaker fees from Pfizer, Radcliffe Cardiology, Amarin, Bristol-Myers Squibb, Edwards Lifesciences, and Novartis; he has received consultancy fees from Novartis, Jupiter Bioventures, AstraZeneca, Novo Nordisk, UCB Biopharma, Beren, and Silence Therapeutics; and is funded by the British Heart Foundation (FS/SCRF/21/32010). B. Prendergast has received speaker fees from Edwards Lifesciences and Polares Medical. N.J. Craig is funded by the Medical Research Council (MR/Y009932/1). D.E. Newby (CH/09/002/26360, RG/F/22/110093, RE/24/130012) is funded by the British Heart Foundation.