Description - technical specifications
The Helio transcatheter aortic dock (Edwards Lifesciences, Irvine, CA, USA) consists of a self-expandable nitinol stent encased in polyethylene terephthalate (PET) fabric (Online Figure 1). The dock is fixed inside the aortic root and it is intended to assist in annular fixation of a standard balloon-expandable SAPIEN XT transcatheter heart valve (THV) by incorporating and entrapping the native cusps (Figure 1). The currently available dock has a diameter of 25 mm, suitable for implantation with a 29 mm SAPIEN XT THV. It is intended that future devices will be compatibl e with a full range of balloon-expandable valves.
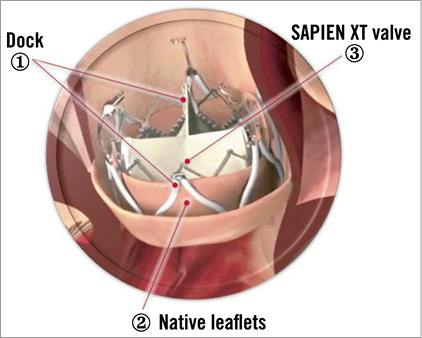
Figure 1. Illustration of the SAPIEN XT valve placed into the Helio dock. The dock is positioned behind the aortic cusps which are captured between the SAPIEN XT valve and the dock.
The dock is fixed to a delivery catheter by means of three detachable arms. The transarterial delivery catheter is similar in design to the steerable and deflectable NovaFlex THV delivery catheter (Edwards Lifesciences).
The first iteration of the Helio system (transfemoral-transapical) required a median sternotomy and left ventricular puncture followed by snaring and externalisation of a wire from the femoral artery. The dock and THV were then introduced simultaneously from the femoral artery and apex on the single wire. Although feasible and successful the procedure was complex. The current iteration of the device has been redesigned to facilitate a fully percutaneous approach using both common femoral arteries for the Helio and the THV insertion (Figure 2).
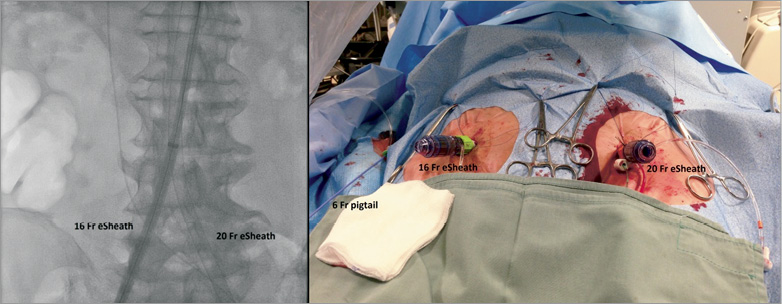
Figure 2. 16 Fr and 20 Fr eSheaths placed in the right and left common femoral arteries. The 6 Fr pigtail is advanced through the right radial artery.
Implantation procedure
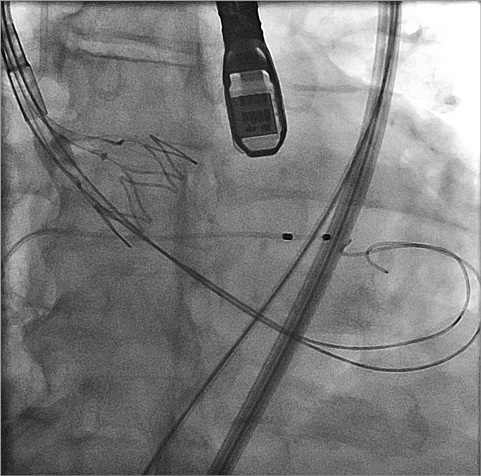
The current iteration of Helio device allows for a fully transfemoral approach and, with preclosure, allows for fully percutaneous access. The two common femoral arteries are cannulated with 16 Fr and 20 Fr expandable sheaths (eSheath; Edwards Lifesciences) (Figure 2). A pigtail catheter is placed in the ascending aorta through a radial artery (Figure 2). The aortic valve is crossed in a standard manner and a 0.035” Amplatz Extra-Stiff wire (Cook Medical, Bloomington, IN, USA) is placed into the left ventricle with a curve to reduce ectopics and improve stability. The Helio delivery catheter is advanced through the 16 Fr eSheath over the stiff wire. The dock is then expanded within the aortic root by retracting a covering sleeve and positioned deep within the sinuses, but outside the aortic valve cusps (Figure 3 and Online moving image 1). Optimal dock positioning is assessed with angiography and transoesophageal echocardiography. The Helio nose cone is withdrawn.
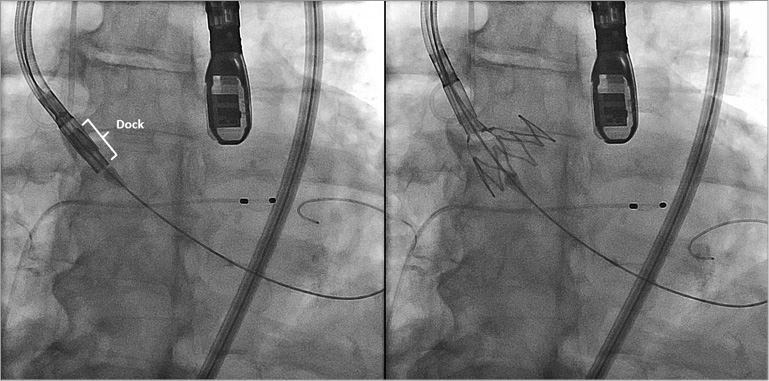
Figure 3. Helio dock deployment into the aortic root.
A second guidewire is placed through the expanded dock and native valve into the left ventricle (Online Figure 2). A NovaFlex THV delivery catheter is then advanced through the contralateral femoral sheath and a SAPIEN XT THV positioned within the dock and within the native valve (Online Figure 3). The Helio guidewire is then retrieved from the left ventricle. The THV is then expanded within the native valve and outer dock. Burst pacing and slow balloon inflation are utilised to facilitate accurate placement (Figure 4). Following echocardiographic and fluoroscopic assessment, the dock is detached and both delivery catheters removed (Figure 5, Online moving images 2, 3, 4 and 5).
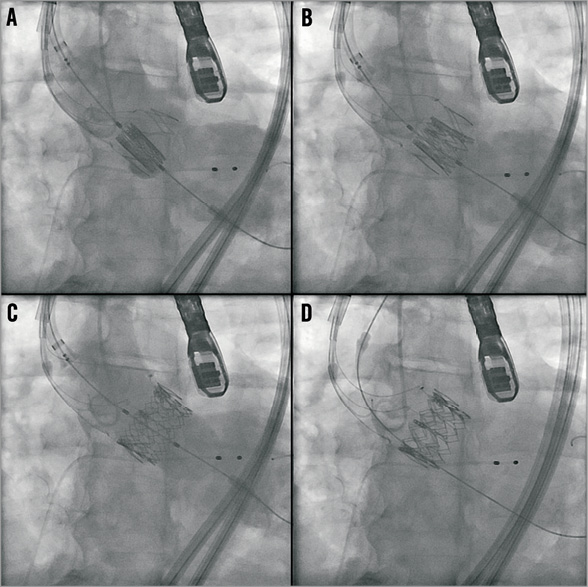
Figure 4. 29 mm SAPIEN XT deployment into the Helio dock.
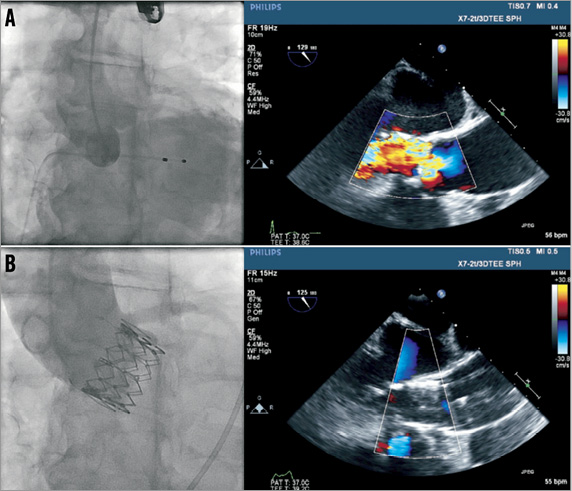
Figure 5. Angiographic and TEE assessment of the aortic regurgitation pre (A) and post (B) Helio and SAPIEN XT implantation.
Discussion
The Helio transcatheter aortic dock is the first dedicated transcatheter device for the treatment of pure AR. The current system facilitates a fully percutaneous transarterial procedure. A potential advantage of the system is that incorporation of the native cusps into the device contributes not only to fixation, but also to effective paravalvular sealing. An intended benefit of incorporating the cusps into the device is the potential to stabilise the aortic root and reduce the tendency for ongoing dilation of the aortic root. Earlier experience with the transapical-transarterial approach also demonstrated the feasibility of treating carefully selected aortic stenosis patients with annuli too large for conventional balloon-expandable transcatheter aortic valve implantation.
Alternative devices
Recent reports have documented early experience with “off-label” use of self-expanding THVs in the setting of predominant AR1-4. With the CoreValve device (Medtronic, Minneapolis, MN, USA), secondary anchoring in the ascending aorta contributes to stabilisation, while with the JenaValve device (JenaValve Technology GmbH, Munich, Germany) clips assist with positioning at the level of the native cusps5. Although successful implantation and favourable clinical outcomes have been reported, paravalvular AR, malposition, and ongoing dilation of the aortic root remain concerns4.
Procedural concerns
As compared to conventional transfemoral TAVR for severe aortic stenosis there are additional considerations. The requirement for large sheath access simultaneously from both femoral arteries and the aorta may exclude some patients from consideration. Positioning of the dock requires transoesophageal echocardiographic guidance. Simultaneous positioning and deployment of the dock and SAPIEN XT THV adds a level of complexity. Retrieval and removal of the deployed dock system is not currently possible. Future design modifications may reduce these concerns.
Conclusion
In conclusion, isolated native AR in patients in whom conventional aortic valve replacement is undesirable represents a therapeutic challenge because of the lack of purpose-specific transcatheter devices. THVs intended for patients with aortic stenosis have been used in this setting. However, suboptimal annular anchoring resulting in malposition and migration, suboptimal sealing with paravalvular regurgitation, and ongoing outward radial forces associated with self-expanding devices in the setting of an enlarged and enlarging root are a concern. The Helio transcatheter aortic dock is the first dedicated device for the percutaneous treatment of pure AR. Early experience demonstrates feasibility and efficacy. Further evaluation continues.
Conflict of interest statement
J. G. Webb and J. Ye are consultants for Edwards Lifesciences. S. Pasupati is a proctor for Edwards Lifesciences, Medtronic and St. Jude Medical. The other authors have no conflicts of interest to declare.
Online data supplement
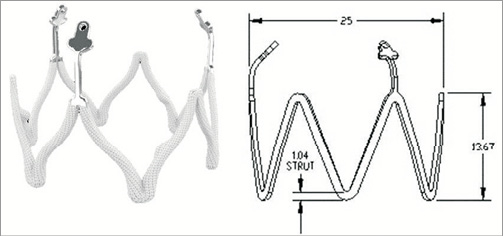
Online Figure 1. The Helio dock.
Online Figure 2. Two Amplatz Extra-Stiff wires placed into the left ventricle.
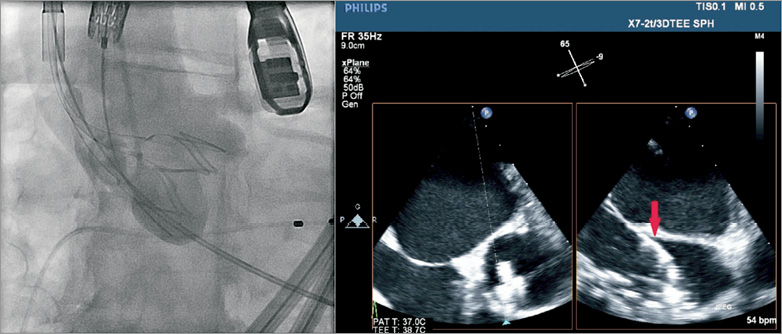
Online Figure 3. Angiographic (left panel) and TEE (right panel) final assessment of dock position (red arrow) before SAPIEN XT deployment. The dock is nicely placed at the basal attachment of the native aortic cusps.
