An 84-year-old male patient with symptomatic severe calcific aortic stenosis was scheduled for elective transcatheter aortic valve implantation (TAVI). The preprocedural echocardiographic examination incidentally revealed, on the suprasternal view, findings indicative of a double-lumen aortic arch (Figure 1A, Figure 1B, Moving image 1, Moving image 2). This is a type of abnormal vascular ring which completely surrounds the trachea and oesophagus and, in the majority of cases, leads to symptoms resulting from compression of these structures12. The subsequent computed tomography confirmed the double-lumen aortic arch arising from the ascending aorta at the level of the sternal angle (Figure 1C, Figure 1D). A dominant left aortic arch (LAA) and a hypoplastic right aortic arch (RAA) encircled the trachea and the oesophagus resulting in a complete vascular ring formation which terminated into the proximal descending aorta (Figure 1E). The left subclavian and carotid artery branched from the LAA, while the right subclavian and carotid artery emerged from the RAA with an absence of the brachiocephalic artery, thus forming the classic “4-vessel sign”12. The vascular channel had no haemodynamic consequences, as in this case, there was no compression of the trachea or oesophagus, and the patient had no respiratory or gastrointestinal symptoms. Moreover, no congenital malformations were detected, and echocardiography showed no accompanying intracardiac anomalies or defects.
As the patient was an octogenarian, with an estimated European System for Cardiac Operative Risk Evaluation (EuroSCORE) of 8%, the Heart Team decided to perform TAVI. Fluoroscopic assessment and other selected projections showed that the straight trajectory of the LAA was the most straightforward interventional route for the safest delivery of the valve (Moving image 3).
Under fluoroscopy we ensured that the pigtail passed through the RAA with the smaller diameter to the non-coronary cusp for contrast injections during the procedure (Moving image 4). Using the pigtail as a marker, we advanced the Amplatzer (Abbott) catheter over the wire through the LAA, and the usual sequence of the interventional steps were then done for TAVI (Moving image 5). No additional interventional manoeuvres were needed for optimal TAVI (Moving image 6). Finally, we did not perform any predilatation of the valve, and direct TAVI was performed with no need of post-dilatation.
Aortography after TAVI depicted the correct valve position and the double aortic arch (Moving image 7, Figure 1F), and after 3 months, the patient was asymptomatic without paravalvular aortic leakage. To our knowledge, this is the first ever reported case of an asymptomatic double-lumen aortic arch in an octogenarian who has successfully undergone TAVI for severe aortic stenosis.
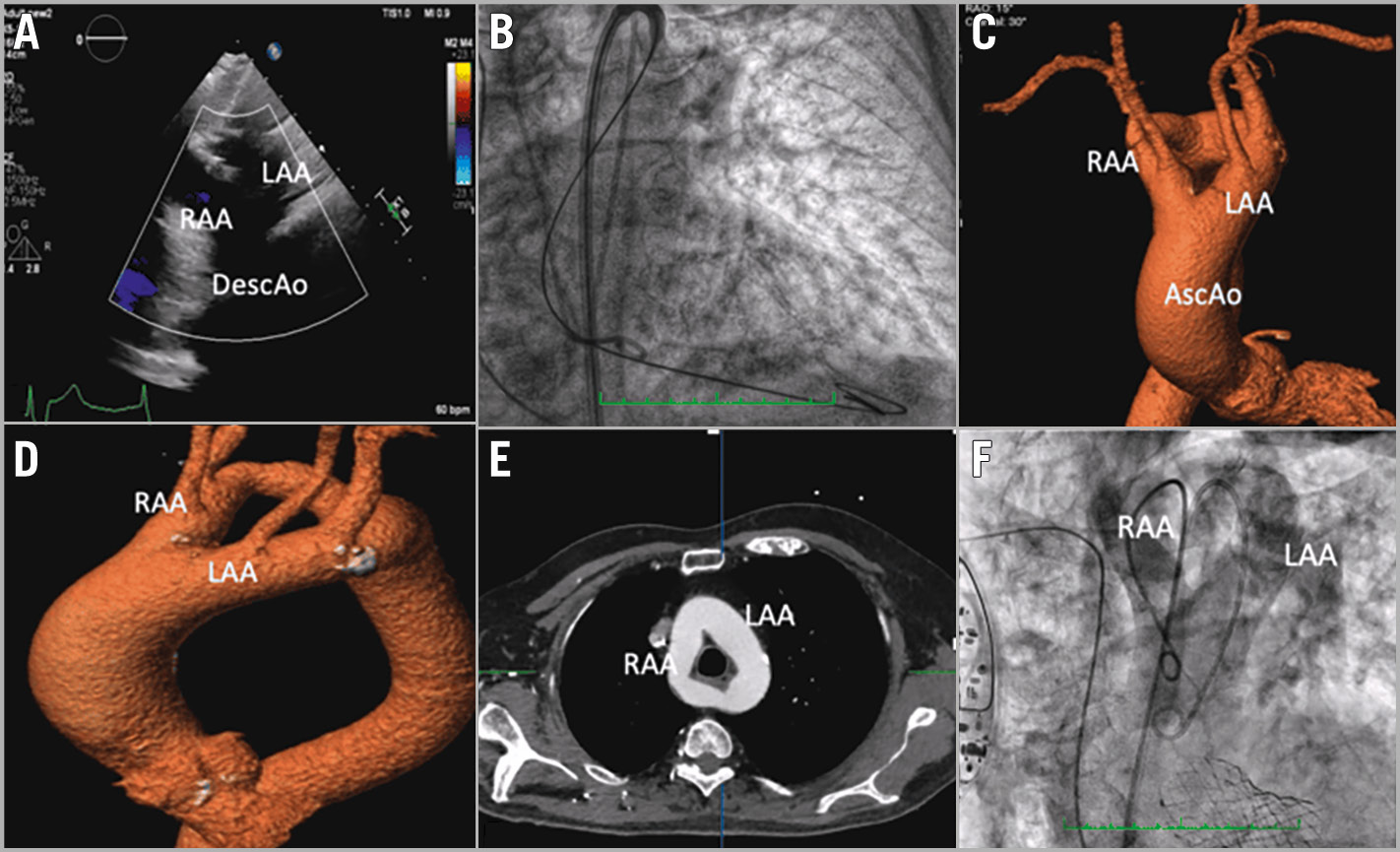
Figure 1. Multimodality imaging of the case. A) Suprasternal echocardiographic views indicative of a double-lumen aortic arch. B) Fluoroscopy showing the valve passing by the left aortic arch. C-D) Computed tomography confirming the double-lumen aortic arch arising from the ascending aorta (AscAo) at the level of the sternal angle. E) A dominant left aortic arch (LAA) and a hypoplastic right aortic arch (RAA) terminating into the proximal descending aorta (DescAo). F) Final aortography after transcatheter aortic valve implantation.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 5. Using the pigtail as a marker, we advanced the Amplatzer catheter over the wire through the LAA and the usual sequence of the interventional steps were done for transcatheter aortic valve implantation (TAVI).
Moving image 6. No additional interventional manoeuvres were needed for optimal TAVI.
Moving image 7. Aortography after TAVI depicted the correct valve position and the double aortic arch.
Moving image 1. The suprasternal view of the preprocedural echocardiographic examination incidentally revealed findings indicative of a double-lumen aortic arch.
Moving image 2. The suprasternal view of the preprocedural echocardiographic examination incidentally revealed findings indicative of a double-lumen aortic arch.
Moving image 3. The straight trajectory of the left aortic arch (LAA) was the most straightforward interventional route for the safest delivery of the valve according to the fluoroscopic assessment and selected projections.
Moving image 4. Under fluoroscopy we ensured that the pigtail passed through the right aortic arch (RAA) with the smaller diameter to the non-coronary cusp for contrast injections during the procedure.
