A frail 88-year-old female, who 9 years earlier underwent surgical aortic valve replacement (21 mm Trifecta valve; Abbott) and coronary artery bypass graft (left internal mammary artery [LIMA] to left anterior descending artery), presented with heart failure due to severe intraprosthetic regurgitation and a dysfunctional LIMA. The patient suffered a severe anaphylactic reaction to contrast media after coronary angiography and, somewhat unexpectedly, had a second near-fatal anaphylactic reaction during multislice computed tomography (MSCT), despite steroid and antihistamine premedication. MSCT identified a high risk of bilateral coronary artery obstruction accompanying transcatheter aortic valve-in-valve implantation (ViV-TAVI) (Figure 1A).
In this challenging scenario, a pre-emptive double chimney stenting technique during ViV-TAVI was considered the only feasible treatment option (Figure 1B). During transfemoral ViV-TAVI under local anaesthesia, drug-eluting stents (DES) were parked in the left (LCA; 4.0x20 mm; left radial access) and right (RCA; 3.5x24 mm; right radial access) coronary arteries, and a 23 mm Evolut PRO (Medtronic) transcatheter heart valve (THV) was deployed. The size of both DES was determined according to the previous coronary angiography. Both DES were retracted and positioned alongside the THV frame prior to the final THV release and then simultaneously deployed on the release (Moving image 1). Intravascular ultrasound (IVUS) confirmed adequate position of both DES but revealed underexpansion of the LCA DES, requiring post-dilatation with a 5.0x21 mm non-compliant balloon (Figure 1C, Moving image 2, Moving image 3). Transthoracic echocardiography showed no paravalvular leak and a 12 mmHg transprosthetic mean gradient. No contrast was used throughout the procedure. The patient was discharged on day 2 post-procedure on dual antiplatelet therapy and remains well at 1-year clinical follow-up. A 6-week non-contrast MSCT showed adequate position and expansion of both DES (Figure 1D).
No-contrast ViV-TAVI is feasible in patients with contrast allergy or a high risk of acute kidney injury, as most surgical heart valves provide anatomic landmarks for THV deployment. In patients at high risk for coronary artery obstruction, IVUS facilitates the assessment and optimisation of chimney stenting.
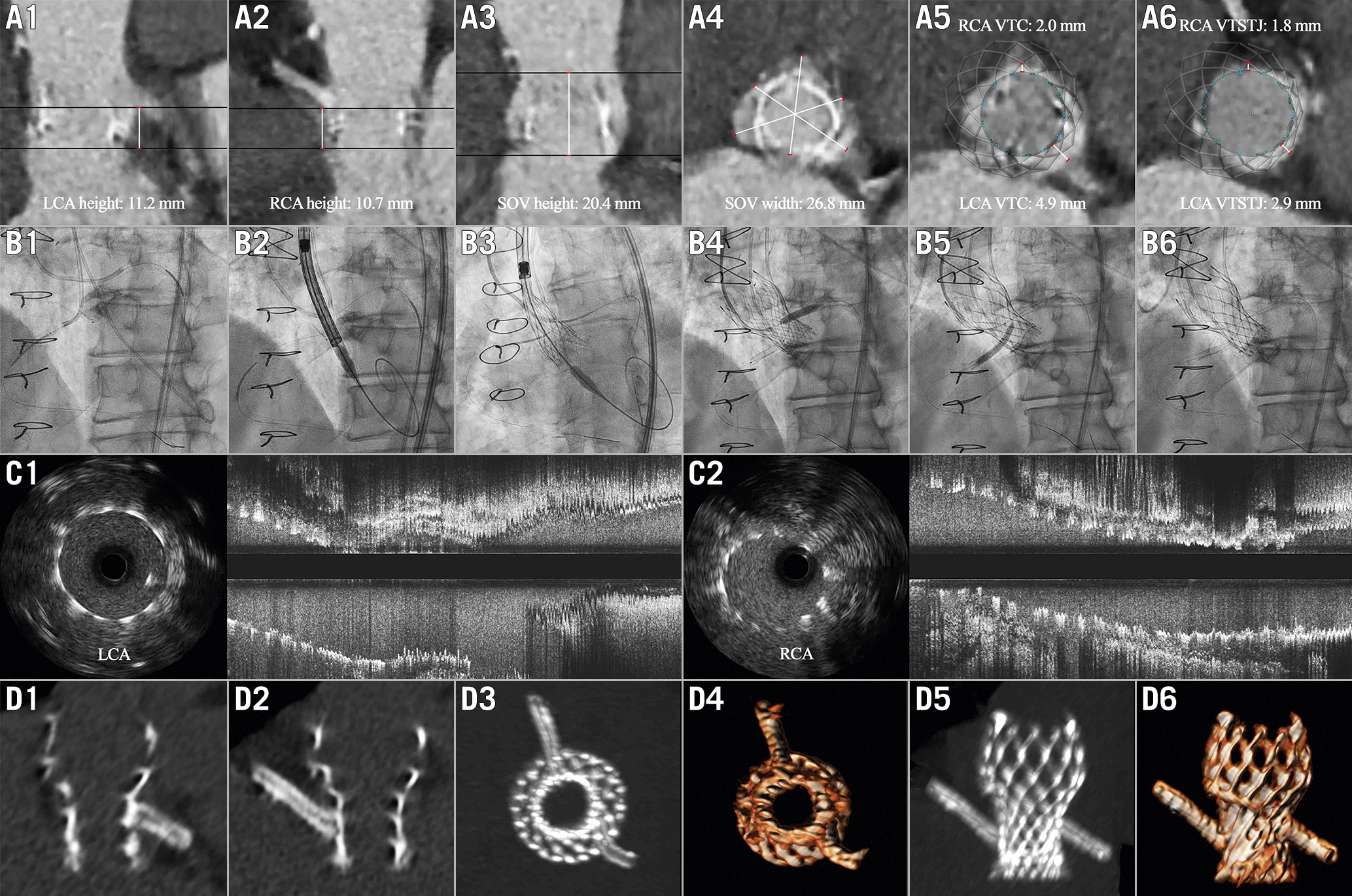
Figure 1. Double chimney stenting without contrast during transcatheter aortic valve-in-valve implantation. A) MSCT showing high risk of bilateral coronary artery obstruction. B) Double chimney stenting technique. C-D) IVUS and non-contrast MSCT confirming adequate position of both DES. DES: drug-eluting stent; IVUS: intravascular ultrasound; LCA: left coronary artery; MSCT: multislice computed tomography; RCA: right coronary artery; SOV: sinus of Valsalva; VTC: virtual transcatheter heart valve to coronary artery ostium distance; VTSTJ: virtual transcatheter heart valve to sinotubular junction distance
Guest editor
This paper was guest edited by Franz-Josef Neumann, MD; Department of Cardiology and Angiology II, University Heart Center Freiburg - Bad Krozingen, Bad Krozingen, Germany.
Conflict of interest statement
D. Mylotte is a consultant for Medtronic, Boston Scientific, and Microport. The other authors have no conflicts of interest to declare. The Guest Editor reports lecture fees paid to his institution from Amgen, Bayer Healthcare, Biotronik, Boehringer Ingelheim, Boston Scientific, Daiichi Sankyo, Edwards Lifesciences, Ferrer, Pfizer, and Novartis; consultancy fees paid to his institution from Boehringer Ingelheim; and grant support from Bayer Healthcare, Boston Scientific, Biotronik, Edwards Lifesciences, GlaxoSmithKline, Medtronic, and Pfizer.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Simultaneous THV and DES deployment.
Moving image 2. LCA IVUS after chimney stenting.
Moving image 3. RCA IVUS after chimney stenting.