Abstract
Primary percutaneous coronary intervention (p-PCI) is considered the gold standard reperfusion strategy for patients with ST-elevation myocardial infarction (STEMI). In the last two years, the Stent for Life (SFL) Initiative has aimed at expanding the use of p-PCI in Greece and several other European countries. During this short period of time, intensive efforts towards propagating the main objectives of the programme in Greece and important actions on the organisation and activation of two p-PCI networks in Athens, the Greek capital, and Patras in south-western Greece, have led to a dramatic nationwide increase of p-PCI rates among STEMI patients (from 9% to 32%). Especially in Athens, p-PCI is implemented in almost 60% of the cases with a diagnosis of STEMI. Recent data from the Greek national registry on acute coronary syndromes underscore the need to improve p-PCI time delays which are partially attributed to inter-hospital delays from hospitals with no p-PCI facilities to p-PCI hospitals. A national public campaign for the promotion of p-PCI is progressing very fast, while specific planning for the recruitment of additional hospitals in urban and rural areas to join old, or to form new p-PCI networks is still developing.
Introduction
The heterogeneity of care among different continents, countries or even areas of the same country for patients with acute coronary syndromes (ACS) has been reported often in several studies and registries1. Early revascularisation with primary percutaneous coronary intervention (p-PCI) in patients with ST-elevation myocardial infarction (STEMI) is life-saving and, according to ESCARDIO guidelines, is the preferred reperfusion strategy2. However, the use and access to p-PCI varies substantially across Europe3.
A recent report on the reperfusion therapy for STEMI patients in 30 European countries showed a suboptimal p-PCI implementation in Greece and five other European countries1. To increase patient access to p-PCI across Europe, the European Association of Percutaneous Cardiovascular Interventions and EuroPCR, together with the European Society of Cardiology Working Group on Acute Cardiac Care, invited the national societies of cardiology of those six countries to participate in the Stent for Life Initiative (SFL). After this first SFL recruitment, four additional countries were invited to participate in the programme.
The mission of the SFL coalition is to promote the life-saving indication of PCI in ACS to reduce the mortality and morbidity rates of patients suffering from ACS.
The following report aims to provide an overview of the organisation of the SFL programme in Greece and some of the progress on the reperfusion therapy in STEMI which has already been seen after its implementation .
The Stent for Life Initiative in Greece
SFL STRUCTURE AND ORGANISATION
Greece became a member of the SFL Initiative in August 2009. The first step was the establishment of the Hellenic steering committee with representatives from the Hellenic Society of Cardiology, Ministry of Health, and the emergency medical system (EMS). The next step was to appoint a SFL project manager, and a task force committee to coordinate and manage SFL activities throughout the country.
GREEK NATIONAL MEETINGS
More than twenty national meetings dedicated to SFL have been held in almost every region of the country including isolated areas and islands. Furthermore, the SFL objectives and plans for implementation have been presented to industry representatives, the Board of the Hellenic Society of Cardiology, the Ministry of Health and cardiologists.
PRIMARY PCI NETWORKS
Two major p-PCI networks have been established: the first in Athens, the Greek capital with almost four million inhabitants (≈40% of the total Greek population), and the second in Patras, a p-PCI network covering a region of almost 750,000 inhabitants in south-western Greece.
EMS
In Athens, the following comprehensive EMS actions to facilitate the transfer of patients with STEMI to p-PCI centres have recently been applied:
– Priority transfer is given for chest pain patients. A fully equipped ambulance nearest to the patient transfers the patient to the nearest p-PCI hospital
– Time delays >5 minutes for patient pick-up are considered an alarm code. In this case, the chief EMS doctor is alerted and has the responsibility to organise the immediate transfer of the chest pain patient
– Non-PCI hospitals are bypassed and the patient is transferred directly to a p-PCI hospital
The Greek ACS national registry
To improve the quality of both ACS and non-ACS care in patients referred for PCI, a comprehensive national registry was conducted by the Hellenic Working Group of Interventional Cardiology between 2008 and 2010.
To improve implementation and identification of possible barriers to the SFL strategy in Greece, a national ACS registry started to enrol patients in September 2011. Obtaining and extrapolating the data from both registries, the daily practice and contemporary trends in ACS treatment and outcomes in Greece were investigated.
Preliminary results of the registry
In total, 16,778 PCI procedures were performed. Twenty-two per cent of them (n=3,733) were p-PCIs.
ANNUAL INCIDENCE OF ACS
The annual hospital admissions for ACS were 21,687. The absolute number of annual hospital admissions for STEMI was 11,731 and for non-ST-elevation myocardial infarction (NSTEMI) 9,956.
REPERFUSION STRATEGY IN STEMI
A reperfusion strategy (p-PCI or TL) was used in the majority of patients with STEMI (72.12%). Thrombolysis (TL) is still the dominant reperfusion therapy in STEMI patients (40.3%), as it was in the previous national registry (41%). The use of p-PCI as the first reperfusion choice was significantly increased as compared to the pre-SFL era (31.82% vs. 9%)4. Of note, “no reperfusion” rates decreased by 44% (from 50% in previous years to 27.88%) (Figure 1).
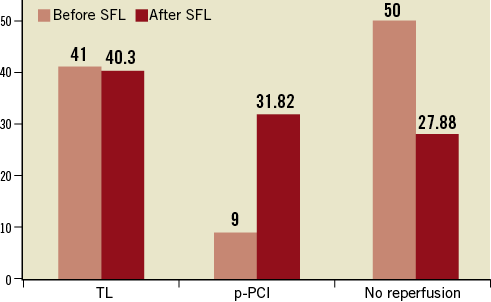
Figure 1. STEMI reperfusion strategy before and after Stent for Life Initiative.
Especially in Athens, p-PCI and TL were implemented in 59.5% and 25% of patients with STEMI, respectively, and only a very small subgroup of patients did not receive any reperfusion (15.5%). Preliminary data from Patras suggest that p-PCI is the dominant reperfusion therapy for STEMI patients.
Rescue PCI was required in 7.4% of cases and a pharmaco-invasive approach was considered for only 6.4% of patients.
IN-HOSPITAL MORTALITY RATES
In-hospital mortality rates for STEMI patients are shown in Figure 2. Patients with STEMI referred for p-PCI had the lowest mortality rates as compared to TL, rescue PCI and no reperfusion. In-hospital mortality in NSTEMI patients was 4%.
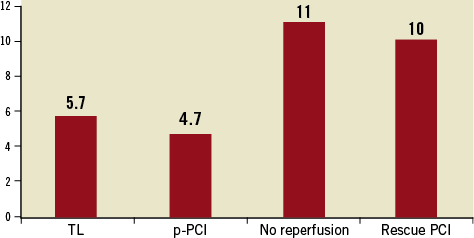
Figure 2. In-hospital mortality rates in STEMI patients according to reperfusion strategy.
TIME DELAYS
The mean time from symptom onset to first medical-contact (FMC), which is defined as the time of diagnostic electrocardiogram or the ambulance arrival, was 140 minutes. Although only 37.9% of STEMI patients registered were transferred to the p-PCI hospital via EMS, a twofold increase of the EMS STEMI transfers was observed as compared to the pre-SFL period (17%).
The time from FMC to arrival at the PCI centre for all STEMI patients was 129.11 minutes. The door-to-balloon time or the time from arrival at the PCI centre to PPCI was 53.41 minutes. The FMC to balloon time was 182.52 minutes and includes both inter-hospital transfers and direct admissions to p-PPCI hospitals. Conversely, FMC to needle for patients in the TL group was 62.17 minutes.
Discussion
The present registry is organised to provide real-world data on contemporary STEMI care in Greece. Primary PCI use rose rapidly after Greece joined the SFL coalition. It is noteworthy that p-PCI now appears to be the dominant therapy for STEMI patients in the Athens and Patras regions. In these regions there are two well-organised networks. More than 40% of the total population of Greece live in Athens and p-PCI may be offered in as many as 59% of STEMI patients. Our findings confirm the general notion that there are wide variations in the choice of reperfusion therapy and time to treatment.
INCIDENCE OF STEMIS AND NSTEMIS
In contrast to other studies from Europe1 and USA5, STEMI’s annual incidence is higher in Greece as compared to NSTEMI’s. This is in accordance with previous Greek registries conducted in rural areas and the countryside4 although the data are preliminary and have to be confirmed on the basis of a long-term registration of ACS patients.
NUMBER OF P-PCIS VS. TL VS. NO REPERFUSION
As it has already been mentioned, there is a clear increase in the number of p-PCI procedures in recent years. There was a threefold increase in the number of p-PCIs in 2011 as compared to the last p-PCI report (2008-2010). This increase is linked to a dramatic decrease (44%) of the no-reperfusion option for STEMIs. The high p-PCI rates in Athens (≈60%), where the first p-PCI network was activated, have to be emphasised. For this area, one of the initial goals of the SFL Initiative (p-PCI in >70% of STEMIs), has almost been accomplished. Organisation and activation of other p-PCI networks all over the country could increase the access and delivery of p-PCI in Greece even more.
IN-HOSPITAL MORTALITY RATES
Our data again suggest the superiority of p-PCI over TL in regard to prognosis. Although the purpose of the registry was not a direct comparison among reperfusion strategies in STEMI, p-PCI was associated with the lowest in-hospital mortality rates, as it has been shown in other studies6-10. Very interestingly, rescue PCI after failed TL is associated with high in-hospital mortality rates similar to the no-reperfusion subgroup of patients. The weight of evidence is very strong and favours a p-PCI rather than a TL reperfusion strategy.
TIME TO REPERFUSION
In the current registry, the percentage of patients arriving via EMS at the p-PCI hospitals has increased significantly (37.9%) as compared to the previous European report (17%). This is a big step in order to reach the final goal of the SFL Initiative, to transfer the vast majority of STEMI patients to hospitals with p-PCI facilities via EMS. The extensive and detailed presentation of the Stent for Life programme to medical community in the context of several congresses and meetings, and the opportunity to exchange opinions with doctors, nurses, industry and politicians as well as a public campaign with press conferences and special broadcasting in different local and national television and radio stations might have contributed to the progress seen in STEMI transfer rates via EMS. The ACT NOW - SAVE A LIFE campaign will shortly be launched and an expansion of the access and absolute number of p-PCIs is anticipated.
The FMC-to-balloon time is still suboptimal (≈182 minutes). To improve this time and reduce the delays substantially, a better organisation of the pre-hospital service is warranted. Pre-hospital electrocardiogram and early diagnosis of STEMI, together with a direct transfer to a p-PCI centre, results in lower mortality11-13.
As in other European countries, the majority of STEMI patients in Greece present to hospitals without p-PCI facilities, so the need for dedicated pre-hospital systems for early diagnosis and transport to a p-PCI centre is of paramount importance. Future plans comprise the development of an effective EMS with adequately equipped ambulances (12-lead electrocardiogram, teletransmission and resuscitation facilities) and trained personnel. From our personal experience the better organisation of the out-of-hours system in p-PCI hospitals might result in a significant reduction in the FMC-to-balloon time in the future.
For certain regions of the country the transfer time to p-PCI centres exceeds the two-hour golden time window. In these areas the majority of patients arrive at hospitals by private means of transport, usually after visiting the local primary healthcare centre or first aid station. Rapid administration of TL and transfer for coronary angiography and PCI three to 24 hours after TL is recommended according to current guidelines14. This pharmaco-invasive approach seems the best reperfusion approach for islands, mountainous villages and isolated areas of the country. For the moment, this strategy is reserved for a very small minority of STEMI patients.
The short FMC to needle time observed might be attributed to the wide availability of TL in primary health care centres.
RESCUE PCI
The number of patients referred for rescue PCI is very low. The current clinical practice in some of the countryside hospitals of re-administration of TL or a conservative strategy after failed TL, especially for small infarctions, may explain the low rescue PCI rates observed in our registry.
Conclusion
The implementation of the SFL Initiative in Greece has led to significant access and use of p-PCI with acceptable in-hospital mortality rates. Recruitment of additional local p-PCI networks, improvement of pre-hospital diagnosis and transfer EMS facilities and expansion of the public Stent for Life campaign could further improve reperfusion success rates, quality of care and reduce mortality and morbidity in STEMI patients.
Conflict of interest statement
The authors have no conflict of interest to declare.