Abstract
Italy was one of the first countries in Europe to perform primary percutaneous coronary intervention (p-PCI) and some regions are still a model for the ST-elevation myocardial infarction (STEMI) network organisation. However, in Italy, as in other European countries, some regional disparities have emerged which are related to geographical, economic, organisational and structural issues. Although some regions have excellent STEMI networks, others still have to develop a model which will allow each STEMI patient to receive the best reperfusion treatment.
Seven areas where patient clinical needs are not met were identified as primary “Stent for Life” targets in Italy: five main regions in the south of Italy, namely Campania, Sicilia, Puglia, Basilicata and Calabria, and two major areas in the north, the districts of Piemonte and Veneto. In this review we describe socio-political issues and orographic barriers to implementation of STEMI guidelines that have been identified and some hints on what we have done in each target region in order to expand the p-PCI service.
Introduction
Italy’s healthcare system is regarded as the second best in the world and, according to the Central Intelligence Agency world fact book, has the world’s 19th highest life expectancy (80.9 years in 2004)1. Healthcare spending in Italy accounted for 9.0% of gross domestic product in 2006 (about 2,600 US dollars per capita) of which about 75% is public2. The public part is the National Health Service (SSN: Servizio Sanitario Nazionale) which is organised under the Ministry of Health and is administered on a regional basis.
Italy’s National Health Service is statutorily required to guarantee the uniform provision of comprehensive care throughout the country. However, this is complicated by the fact that, constitutionally, responsibility for healthcare is shared between the central government and the 20 regions. As a result, there are large and growing differences in regional health service organisation and provision, and ever-increasing regional disparities.
Primary percutaneous coronary intervention in Italy
Italy was one of the first countries in Europe to perform primary percutaneous coronary intervention (p-PCI) and some regions are still a model for the ST-elevation myocardial infarction (STEMI) network organisation. Data from the Italian Society of Invasive Cardiology (SICI-GISE) showed that approximately 28,000 p-PCI were performed by the 260 cathlabs located across the country in 2010 (an increase of 9.7% compared to 2009) with an average of 465 primary PCI/million inhabitants/year (Figure 1)3.
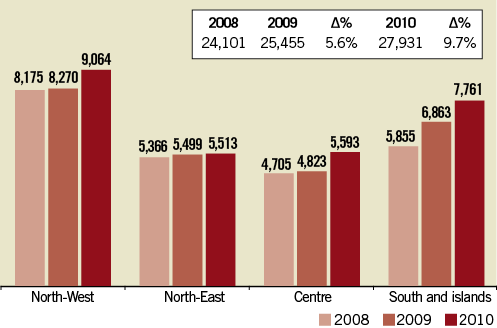
Figure 1. Number of p-PCIs in four different Italian macro-areas in the last three years (data from SICI-GISE).
However, in Italy, as in other European countries4, some regional disparities have emerged which are related to geographical, economic, organisational and structural issues. Although some regions (e.g., Emilia-Romagna, Liguria, Lombardia, Toscana) have excellent STEMI networks5, others still have to develop a model which will allow each STEMI patient to receive the best reperfusion treatment, resulting in an annual rate of p-PCI well below the national average and the standards (600/million inhabitants/year) recommended by the European Association of Percutaneous Cardiovascular Interventions (EAPCI) and the European Society of Cardiology (ESC) (Figure 2)6.
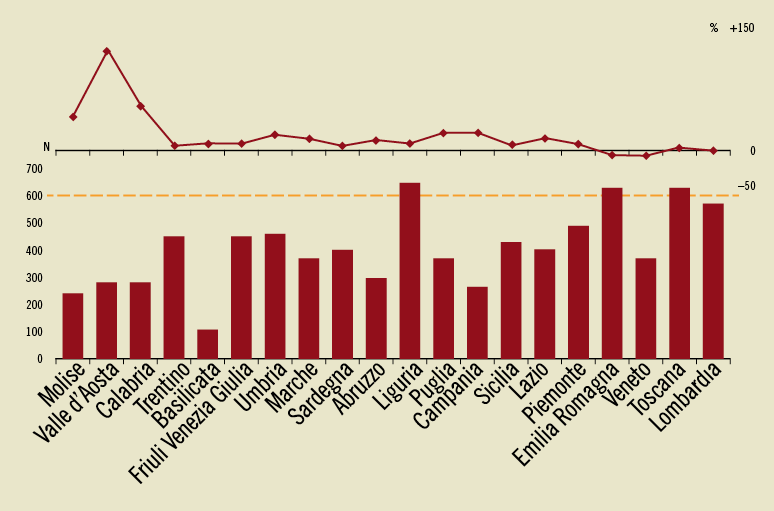
Figure 2. Primary PCI per 1,000,000 inhabitants in different Italian regions (data from SICI-GISE, year 2010). In the upper part of the graph: delta % compared to 2009 in each single region.
The RETE IMA Web survey
The RETE IMA Web survey was launched in 2007 by GISE in collaboration with the Italian Federation of Cardiology, with the aim of evaluating the current state of the regional system of care for STEMI in Italy. Interventional cardiologists and the personnel of the emergency medical system (EMS) participated in the survey7. Data collection was made using different electronic forms with access limited by personal passwords. The survey assessed the organisation of the regional system of care together with local resource availability, with specific attention given to the distance from a hub centre. The survey ended in December 31, 2008, and covered 701 hospitals admitting STEMI patients, 157 (22.4%) with uninterrupted access (24 hours/7 days) to the catheterisation laboratory (2.67 per million inhabitants). An operative network was present in 36/103 (35.9%) provinces, with important geographic variability (Figure 3)7. Among hospitals without a full-time p-PCI facility, only 46% were within a regional system of care. ECG was available in 72% of the national territory, telemedicine in 50%. Pre-hospital fibrinolysis was available in 16% of the country. Overall, 92.4% of the Italian population resides within 60 minutes of a hub centre.
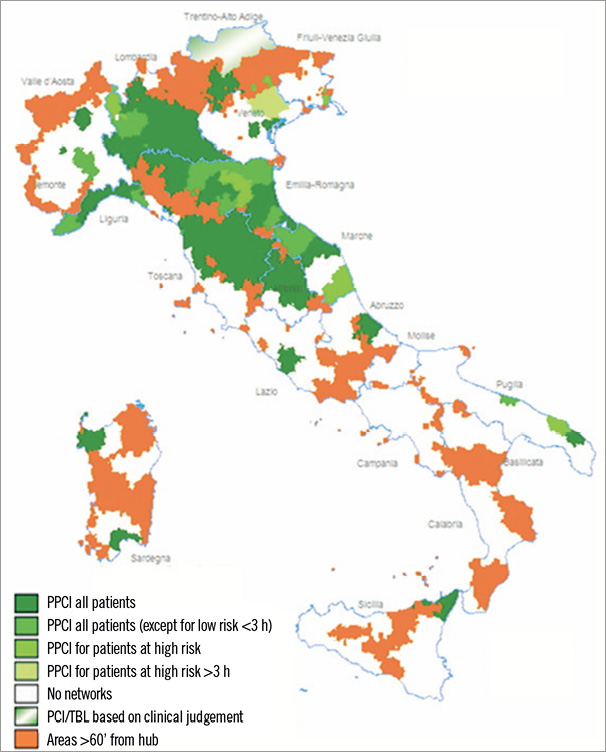
Figure 3. RETE IMA Web: operative network present in Italy in 2008 (from reference 7, with permission)
These data suggest that the lack of STEMI networks is not related to the need for infrastructures such as cathlabs or coronary care units (CCUs), but is linked more to organisational and political issues.
Stent for Life in Italy
SICI-GISE signed the Stent for Life (SFL) Declaration for Italy at the ESC Annual Congress in August 20108. From that time on, we wrote all SFL documents tailored for Italy and the GISE green paper, a consensus document on STEMI network development. Then we organised the kick-off meeting of SFL ITALIA which was held in Rome on April 8th 2011, that involved around 100 key opinion leaders and health commission representatives coming from the initiative’s target regions. During the meeting and later, we analysed and mapped health plans, reimbursements and STEMI systems of care, identified barriers for p-PCI use, and designed possible plans of action at a local level. Considering the different existing realities in territorial networks for STEMI present in Italy, we developed selective regional action plans offering a contribution in background and network plan development, qualified at the national level, in alliance with recognised external organisations. In order to ensure access to p-PCI and the success of the SFL Initiative we looked for the combined support and participation of many stakeholders and partners, including interventional cardiologists, clinical cardiologists, emergency medical systems, government representatives, industry, advocacy groups and patients themselves.
Seven areas with unmet clinical needs were identified as primary SFL targets in Italy, based on population and the results of the RETE IMA Web survey: five main regions in the south of Italy, namely, Campania, Sicilia, Puglia, Basilicata and Calabria (the latter included in the project from January 2012), and two major areas in the north, the districts of Piemonte and Veneto (Figure 4). Approximately 21 million inhabitants are potentially involved (35% of the total population).
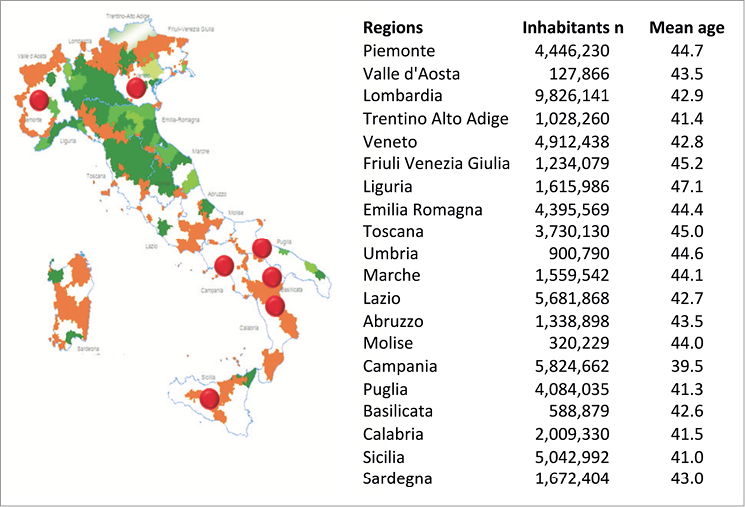
Figure 4. Target regions of SFL Italia (red bullets) identified on the basis of RETE IMA Web survey and number of inhabitants.
In all of these regions we are working to implement local STEMI treatment guidelines, identifying and eliminating specific barriers to those guidelines. In a few months of activity we had several meetings with health commissions in some of the target regions which embraced the SFL project and assigned a task to reorganise their STEMI systems of care.
Below we have detailed some socio-political issues and orographic barriers to the implementation of STEMI guidelines that have been identified, and some hints on what we have done in each target region in order to expand the p-PCI service.
SICILIA
Sicilia, located in the south-east of Italy, is the largest island in the Mediterranean Sea. Along with the surrounding minor islands, it constitutes the Sicilian autonomous region. The terrain of inland Sicilia is mostly hilly. In Sicilia there are nine provinces (five million inhabitants) and only two metropolitan areas: Palermo, that has a larger urban zone of about 900,000 people, and Catania with 650,000 people. Thirty CCUs and 19 cathlabs (2,415 p-PCIs in 2010) are present, with quite a homogeneous distribution over the entire territory. The EMS is underused (less than 20% of calls) and carries the patient to the nearest hospital, especially in rural areas.
A few months after the kick-off of the SFL programme in Italy, Sicilia issued a regional decree law on the organisation of their STEMI network. In this regional law, based on a green paper produced by the steering committee of SFL Italia, all specific duties and requirements of the EMS, emergency room, CCUs and cathlabs involved in the network, together with standards and data collection for quality control, were clearly stated. The STEMI network is scheduled to start officially in July 2012. In the meantime, the regional health government and four macro-area committees are making every effort in terms of EMS staff training, with certified courses on advanced life support and ECG lectures, and on EMS structure improvement by equipping the vast majority of ambulances with ECG teletransmission.
In this target region of SFL Italy, we are conducting a survey on the health costs of STEMI reperfusion in partnership with the CERGAS, Bocconi University of Milan. This survey will analyse the impact, in terms of cost/effectiveness before and after the set-up, and implementation of a network for p-PCI (this project is the subject of another article in the present supplement).
CAMPANIA
Campania, located in southern Italy, has a population of around 5.8 million people, making it the second most populous region of Italy; its total area of 13,590 km² makes it the most densely populated region in the country. The region is divided into five provinces: Naples, Benevento, Avellino, Caserta and Salerno. Over half of the population is resident in the province of Naples, Naples being the capital city of Campania, where there is a population density of 2,626 inhabitants per km2. Within the province, the highest density can be found along the coast where it reaches 13,000 inhabitants per km2 in the city of Portici, one of the most densely populated cities on the planet. The mountainous interior is fragmented into several massifs, rarely reaching 2,000 metres, whereas close to the coast there is the volcanic massif of Vesuvio (1,277 m). In this region, there are 47 CCUs and 20 cathlabs (10 with 24 hours/7 days facilities), performing 1,760 p-PCIs per year. The number of CCUs and cathlabs is adequate but not well distributed across the territory. The number of ambulances is inadequate, with physician staff on board but without ECG teletransmission in the vast majority of cases and not connected to a central hub.
At the end of 2010, the regional health government issued a decree for a reassessment of the hospital and territorial network for STEMI care. After several meetings with local health commissioners, SFL Italia promoted the institution of a regional commission for the definition of single provincial protocols for the STEMI network, assessment of actual status of EMS, development of ECG teletransmission and training of EMS staff. This year, a pilot project on the STEMI network is planned to start in the province of Avellino.
AREAS OF PIEMONTE AND VENETO
Piemonte, located in the north-western part of the peninsula, is the second largest of Italy’s regions after Sicilia, with an area of 25,402 km2 and a population of about 4.4 million. The population density in Piemonte is lower than the national average (on average 174 inhabitants per km2, rising to 335 inhabitants per km2 in the province of Turin, the capital city of the region). The geography of Piemonte is 43.3% mountainous (it is surrounded on three sides by the Alps), along with extensive areas of hills (30.3%) and plains (26.4%). Piemonte, divided into eight provinces, has 30 CCUs (16 hubs and 14 spokes) and 25 cathlabs well distributed in the territory. In 2010, 4,896 STEMI patients were hospitalised, with only 2,130 p-PCIs performed. Although this region has well established and documented routes for STEMI patients and ECG teletransmission is fairly diffuse in the EMS ambulances, time delays are still suboptimal and pre-hospital diagnosis is underused (with the exception of the provinces of Novara and Cuneo).
In May 2011 the Piemonte region conducted a two-month survey on the routes and modalities of access to hospital of STEMI patients, their modalities of reperfusion treatment and consequent outcomes. This registry showed that the hospital access of patients was via EMS in 51% of cases, that p-PCI was performed in 78% of cases, and that 18% of patients did not receive any reperfusion treatment, with an overall in-hospital mortality of 4.3%.
After these data, with the support of SFL, a task force for the implementation of the STEMI network in the metropolitan area of Turin, as a pilot regional area, was established, and a web-based registry for monitoring the quality of performances in the STEMI setting was instituted.
Veneto is located in the north-eastern part of Italy. It is the eighth largest region in Italy, with a total area of 18,398.9 km2, and its population is about five million, ranking fifth in Italy. Veneto can be divided into four areas: the northern mountainous Alpine zone (29% of the total area), the hill zone (14% of surface), the lower plain, and the coastal territory. Of the seven provinces of the region, the province of Padua is the most populous and has the greatest density, with 424.81 persons per km2.
Veneto has 21 cathlabs which performed 2,022 p-PCIs in 2010. Analysing several data from administrative records, regional and national registries, it emerged that: 1) the incidence of STEMI in this region is lower compared to the national average, being approximately 700/106 inhabitants/year; 2) the mean number of p-PCIs, although it has increased in recent years, is still suboptimal (59% of STEMI treatment); 3) there is a wide regional heterogeneity regarding the number of p-PCIs performed (minimum of 330 p-PCIs/106 inhabitants/year in Verona and maximum of 684 p-PCIs/106 inhabitants/year in the province of Rovigo) probably related to different levels of organisation of STEMI networks and recourse to EMS and ECG teletransmission. In this region SFL is identifying local barriers for using established STEMI routes and implementing the recourse to p-PCI, and is instituting a permanent and reliable system for data collection and analysis.
PUGLIA AND BASILICATA
Situated at the south-eastern tip of the Italian peninsula, Puglia covers over 19,000 km2 in a succession of broad plains and low-lying hills. The only mountainous area, the Gargano promontory, does not exceed 1,150 m and is to be found in the north of Apulia, which is the least mountainous region in Italy. Apulia is divided into six provinces: Bari, Foggia, Taranto, Brindisi, Lecce and Barletta-Andria-Trani (the latter instituted in 2009). The population density in Apulia is just above the national average: in 2008 it was equal to 211 inhabitants per km2. Foggia is by far the least densely populated province (96 inhabitants per km2), whereas Bari (regional capital) is the most densely populated province (308 inhabitants per km2). Apulia has 17 cathlabs which performed 1,687 p-PCIs in 2010.
Basilicata, also known as Lucania, is the most mountainous region in the south of Italy, with 47% of its area of 9,992 km2 covered by mountains, whereas 45% is hilly and 8% is made up of plains. The region can be thought of as the “instep” of Italy, with Calabria functioning as the “toe” and Apulia the “heel”. The region covers about 10,000 km2 and in 2010 had a population of about 600,000. The population density is very low compared to that of Italy as a whole: 59.1 inhabitants per km² compared to a national density of 200.4 in 2010. The region is divided into two provinces: Potenza (regional capital) and Matera. Nowadays, Basilicata has just one cathlab which performed only 61 p-PCIs in 2010. Pre-hospital thrombolysis is widely applied in this region, but coronary angiography after lysis is still underused.
Although these two regions issued a regional law for the institution of STEMI networks several years ago, and regional EMS is supplied with 100% of ambulances equipped with ECG teletransmission (more than 306,000 ECG were teletransmitted in the last six years in Apulia), the majority of STEMI patients, especially in suburban areas, are transported to the nearest hospital, regardless of the presence or absence of cathlab facilities.
SFL Italia organised several meetings with local health and EMS committees and produced a document to be presented at regional government level on the reassessment of regional networks involving EMS, non-PCI hospitals and PCI centres in order to implement p-PCI services effectively.
CALABRIA
Calabria is at the very south of the Italian peninsula, to which it is connected by the Monte Pollino massif, while on the east, south and west it is surrounded by the Ionian and Tyrrhenian seas. The region is a long and narrow peninsula and covers 15,080 km2 with a population of just over two million. Calabria is divided into five provinces: Catanzaro, Reggio, Vibo Valentia, Crotone and Cosenza. The capital city is Catanzaro but the most populated city is Reggio. Some 42% of Calabria’s area is mountainous, 49% is hilly, while plains occupy only 9% of the region’s territory.
Calabria has seven cathlabs (concentrated in two provinces) which performed 589 p-PCIs in 2010. Recently, the local health commission issued a decree on the STEMI network. The objectives of SFL, that included this region in the project just a few months ago, are: 1) to institute a close cooperation between the regional governments, hospitals, EMS and other related bodies in order to achieve the appropriate implementation of p-PCI programmes; and 2) to create local registries on the incidence, treatment and outcomes of hospitalised STEMI patients that might serve as quality control.
Future plans
In the coming months further meetings with some local health commissioners have been scheduled in order to illustrate in detail the initiative and the plans of action, and to support local health commissions for planning and/or implementing p-PCI networks. Finally, a new three-month data collection of the entire Italian network system (second edition of the Rete IMA Web registry) will start soon after a software update, in strict co-operation with the Italian EMS.
Conclusion
The state of territorial networks for STEMI treatment in Italy is heterogeneous and at the same time puzzling. There are some regions with well-developed and pioneering network systems and other areas without a structured system of care for STEMI patients.
The strategic plan of SFL in Italy is to develop a selective approach and implement an action programme to increase patient access to p-PCI in some target regions.
Conflict of interest statement
The authors have no conflict of interest to declare.