Abstract
Aims: Primary percutaneous coronary intervention (PPCI) is the recommended treatment for patients with acute ST-segment elevation myocardial infarction (STEMI). Despite substantial evidence of its effectiveness, a 2007 study reported that only 40-45% of European STEMI patients were treated with PPCI, with large variations in treatment availability between countries. In 2008, the Stent for Life (SFL) initiative was launched by the European Association of Percutaneous Cardiovascular Interventions and EuroPCR in partnership with the European Society of Cardiology (ESC) Working Group on Acute Cardiac Care and country-specific national cardiac societies. The aim is to promote the prioritisation of percutaneous coronary intervention treatment towards those who will benefit most, namely STEMI patients. The following countries are currently participating: Bulgaria, Egypt, France, Greece, Italy, Portugal, Romania, Serbia, Spain and Turkey.
Methods and results: Since SFL was launched, several activities have been initiated in the participating countries. Preliminary reports suggest that major increases have been seen in the numbers of PPCI performed, with some countries reporting very significant increases in PPCI use from 2008-2010. Improvements in STEMI mortality rates have also been observed.
Conclusions: This report summarises the progress of the SFL initiative in the 10 target countries.
Introduction
Guidelines from the European Society of Cardiology (ESC) and the American College of Cardiology (ACC)/American Heart Association (AHA) recommend primary percutaneous coronary intervention (PPCI) as the preferred reperfusion strategy for patients with ST-elevation myocardial infarction (STEMI) when time-to-treatment is less than 90-120 minutes and patients can be treated in a high-volume, well-equipped centre by expert interventional cardiologists1-4. The number of PPCI performed in Europe has steadily increased over the past decade. However a European survey from 2007 reported that only 40-45% of European STEMI patients were treated with PPCI, with large variations in treatment availability between countries5. The challenges involved when introducing new technologies into clinical practice can be substantial and include a complex mix of medical, organisational, patient-related, regulatory and economic factors6.
The Stent for Life initiative
In 2008, the Stent for Life (SFL) initiative was launched by the European Association of Percutaneous Cardiovascular Interventions (EAPCI) and EuroPCR in partnership with the ESC Working Group on Acute Cardiac Care and country-specific national cardiac societies.
The main goal of the initiative is to achieve optimal treatment of STEMI in all member states of the ESC7. The SFL initiative is driven by national cardiac interventional working groups in collaboration with local stakeholders (such as professional societies, government, industry and the public) to improve access to PPCI for all patients with STEMI. National SFL leadership offers general support in developing local action plans, securing SFL budgets, hiring a local project coordinator, presenting country progress at congresses/meetings and supporting involvement from the public and media, with the aim of achieving synergy with existing initiatives7.
THE SFL INITIATIVE WAS SET OUT IN THREE PHASES7:
Phase one
An up-to-date picture of how patients with STEMI were treated in Europe was obtained from a 2010 survey (containing data from 2005-2008) conducted in 30 ESC countries5. Data were collected regarding: 1) prevalence of percutaneous coronary intervention (PCI) and PPCI procedures and numbers of existing PCI and PPCI capable centres; 2) STEMI epidemiology and current treatment organisation; and 3) existing national STEMI or PCI registries. This survey revealed large treatment variations between countries. In northern, western and central Europe, PPCI is offered to 60-90% of STEMI patients. In southern and eastern Europe, thrombolysis is the preferred strategy. The survey also revealed that in countries where thrombolysis is the predominant therapy, fewer patients are offered any type of reperfusion therapy at all5. Based on this publication and on interest from national cardiology societies, the following 10 countries were invited to participate in SFL: Bulgaria, Egypt, France, Greece, Italy, Portugal, Romania, Serbia, Spain and Turkey.
Phase two
Key facilitators of effective implementation of PPCI were identified, based on experiences from “best practice countries”, defined as countries and regions that had succeeded in implementing PPCI for nearly all patients presenting with STEMI8. An article describing the management practice of STEMI in five European countries (Austria, Czech Republic, Denmark, The Netherlands and Sweden8) revealed that several key factors are important for the successful implementation of PPCI. These included stakeholder involvement (professional societies, government, patients), establishment of PPCI networks, 24-hour service seven days a week (24/7), to cover the whole STEMI population and the launch of transportation protocols to bypass hospitals without catheterisation laboratories8. The publication was intended to serve as a guide for the 10 countries working to meet the targets set out in phase three.
Phase three
The main task was to implement local action programmes to increase access to PPCI in the 10 countries. The following three targets were set: 1) Increase the use of PPCI to more than 70% of all STEMI patients; 2) Achieve PPCI rates of more than 600 per million inhabitants per year; 3) Offer a 24-hour PPCI service seven days a week in PPCI centres to cover the needs of the STEMI patient population. Current progress in each of the target countries is detailed below.
TARGET COUNTRIES WHERE THE SFL INITIATIVE WAS LAUNCHED IN 2009
Bulgaria
Since Bulgaria joined the SFL initiative, there has been a significant increase in the number of PPCI per year, from 130 procedures per million inhabitants in 2008 to 530 per million in 2010 (Figure 1). Furthermore, a decrease in mortality (untreated and treated either by thrombolysis or PPCI) from 15.6% in 2008 to 10.4% in 2010 was reported. The numbers reflect an increased number of patients with acute myocardial infarction (AMI) undergoing PPCI.
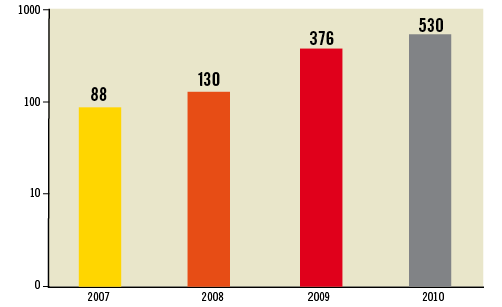
Figure 1. Increase in the numbers of primary percutaneous coronary intervention per million inhabitants from 2007-2010 in Bulgaria. The progress of the SFL initiative led to increased number of patients with acute myocardial infarction (AMI) undergoing PPCI with significant decrease of total AMI mortality from 15.6% to 10.4% for the period, while PPCI AMI mortality remains around 5%. Data from the Bulgarian National Health Insurance Fund
AMI mortality after PPCI remains unchanged at around 5% (numbers are based on data from the Bulgarian national health insurance fund). The number of catheterisation laboratories performing PPCI 24/7 increased from 21 to 30 in 2010.
The Bulgarian Ministry of Health, together with the SFL local initiative, demanded non-stop coverage of PPCI as a requirement for reimbursement of PCI from the National Health Insurance Fund.
The initiative also facilitated the necessary organisational changes concerning patient transportation directly to PPCI hospitals and from non-PCI hospitals to PPCI hospitals.
Substantial progress has also been made in training and certification of new interventional cardiologists, ensuring the presence of qualified staff in all catheterisation laboratories. A national registry for PPCI activities has also been established since November 2011, providing valid data on the number of PPCI, timing and mortality rates.
A public awareness campaign was rolled out in Bulgaria in late 2011. The aim of the campaign was to increase public knowledge about heart attack symptoms, to highlight the need to act quickly and to provide instructions on how to call the national emergency service number for transportation directly to the PPCI centre.
During participation in the SFL, there was considerable organisational improvement in Bulgaria. However, several barriers still are needed to be overcome in order to fully implement the programme. A major goal for the future is to continue to increase the number of patients with STEMI treated by PPCI, and to clarify the benefits of the interventional treatment in order to counteract the negative attitude that has been adopted by some Bulgarian authorities to interventional cardiology. Furthermore, implementation of transmission of electrocardiograms (ECG) by telemedicine in mountain regions is a focus area.
France
As reported in the French Registry of Acute ST-elevation and Non-ST-elevation Myocardial Infarction (FAST MI)9, in 2005 almost 40% of French patients with STEMI did not undergo PPCI or thrombolysis.
To improve this statistic, an action plan was implemented. Initially, five territories in France were selected (Nord, Essonne, Côte d’Or, Haute Savoie and Haute Garonne) according to surface area, population density, hospital accessibility, number of 24/7 PCI centres and number of centres with intensive care units but no catheterisation laboratories.
A prospective and exhaustive registration of the management of STEMI patients was performed for one month during November 2010 in the identified territories. The registry reported that 64% of the study group underwent PPCI, 22% received thrombolysis and 14% did not undergo revascularisation with PPCI or thrombolysis; a substantial improvement from 2005. Although 71% of the patients reacted quickly to their symptoms, less than 50% of these patients called the emergency medical system (EMS) directly.
An action plan was implemented to further improve these results. A national press conference took place in March 2011 and regional press conferences (medical and public media) were organised in the five territories. The main objective of these conferences was to educate patients with chest pain to call the EMS number “15” directly. A cellular phone application has also been developed to explain what to do in case of chest pain. In addition, letters were mailed out to general physicians to make them aware of STEMI management and the SFL initiative.
A new one-month registry took place in November 2011 to evaluate the impact of the action plan. If the results show major improvement in STEMI management compared to November 2010, the action plan will be applied to all territories in France.
Greece
Following enrolment in the SFL initiative, a Hellenic steering committee was formed with representatives from the Ministry of Health and EMS, and a SFL project manager and a task force committee were appointed to coordinate and manage SFL activities throughout the country. Several national meetings were held where SFL objectives and plans for implementation were presented to industry representatives, the Board of the Hellenic Society of Cardiology, the Ministry of Health and cardiologists.
Two major PPCI networks have been established, the first in Athens, a city with almost five million inhabitants (representing 40% of the total Greek population) and a second in south-western Greece covering a region with 750,000 inhabitants. EMS actions for facilitating the transfer for PPCI in the area of Athens have recently been applied and guidelines for the transfer priority of chest pain patients have been implemented. As a result of the above-mentioned actions, overall PPCI rates have increased from 9% to 20%. In the area of Athens, it is now estimated that PPCI is the first choice reperfusion strategy in 35-40% of patients presenting with STEMI.
SFL plans for the future include: a) collection of the data from an ongoing national registry based on all AMI cases; and b) the activation of an additional PPCI network in northern Greece to cover the area of Thessaloniki, the second biggest city in the country.
Spain
In Spain, health system management is under the control of each of the 17 regional governments. In 2008, there were only four regional networks for the treatment of AMI (Murcia, Navarra, Galicia and the Balearic Islands) covering 12.8% of the total Spanish population (5.9 million inhabitants) with an annual PPCI rate of 169 per million inhabitants10. There were 87 centres able to perform PPCI 24/7 (71% of the total number of centres10), with the remaining centres only performing PPCI during normal working hours. In 2009, an AMI network was established in Catalonia, increasing the percentage of the population with access to a PPCI network to 28.8% (13.4 million people) and the overall annual rate to 216 PPCI per million inhabitants11.
In 2010, the SFL Declaration was signed in all 17 regions affiliated with the Spanish Society of Cardiology. An education plan was launched at the National Cardiology Congress and SFL teams were established in three regions with low PPCI rates (Asturias, Aragon and Valencia).
A new STEMI network was launched in 2011 in the region of Castilla La Mancha. This increased the current population with access to a STEMI network to 15.6 million (33.2% of the population in Spain). At the recent Congress of the Spanish Working Group in Interventional Cardiology, the annual mean rate of PPCI was reported to have increased to 235 procedures per million inhabitants in 2010 (Figure 2). Between 2008 and 2010 there was an overall increase of 18% in the number of PPCI performed (12,079 in 2008; 13,395 in 2009; and 14,248 in 2010).
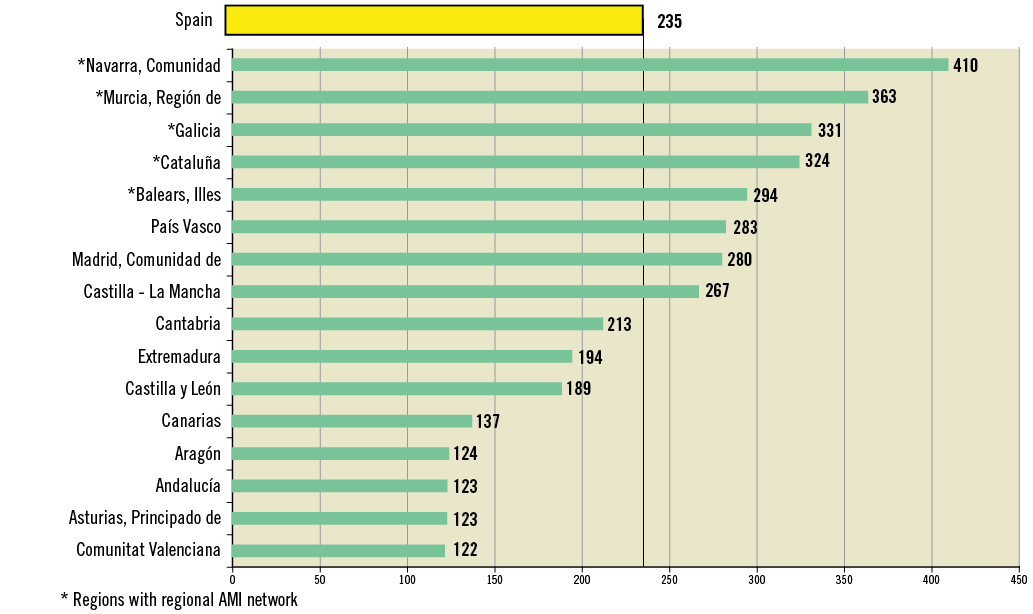
Figure 2. Primary Percutaneous Coronary Interventions per million inhabitants in the Spanish Regions, 2010.
In 2011, a SFL webpage was designed (htpp://stentforlife.secardiologia.es/). In addition, a special SFL supplement was published in the Spanish Journal of Cardiology. During the 2011 Congress of the Spanish Society of Cardiology, SFL sessions were conducted (one in conjunction with the Women in Innovation initiative) and press releases were issued. Catalonia will be the first region where a public awareness campaign will be conducted following the SFL strategy. The future goal is the development of STEMI networks in all regions of Spain.
Serbia
Since joining the Stent for Life initiative in August 2009, Serbia increased the annual number of PPCI from 230 procedures per million inhabitants in 2008 to 337 per million in 2009 and 440 per million in 2010. Preliminary data suggested an additional increase of 18% in PPCI procedures in 2011 (Figure 3). In addition, there was a notable decrease in the percentage of STEMI patients not receiving any reperfusion therapy from 2008-2009. Figures for 2010 are not yet available, but an additional decrease is expected. These improvements were accomplished by nine PCI centres (with a total of 18 catheterisation laboratories) scattered around Serbia. In December 2010, an additional PCI centre (in Valjevo) was opened, which is now performing more than 130 PPCI procedures per year.
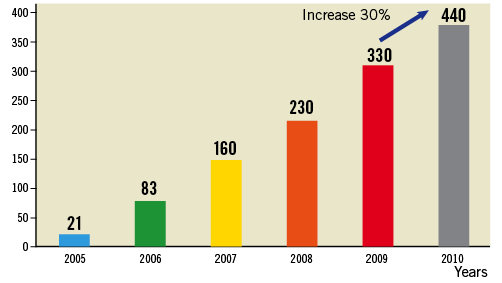
Figure 3. Increase in the numbers of primary percutaneous coronary intervention per million inhabitants from 2005-2010 in Serbia. Numbers are based on data from the National Statistics Serbia.
Serbia is working on establishing pre-hospital thrombolysis in areas where timely PPCI cannot be provided. National guidelines on the best therapy for ischaemic heart disease have been developed.
These activities were made possible by SFL stakeholders, the Serbian government, the medical society, the medical device and pharmaceutical industry and representatives of the press and media.
Turkey
In March 2010, the Ministry of Health and the Turkish Society of Cardiology (TSC) signed a protocol for a national PPCI programme. A pilot project with 18 regional STEMI networks was launched around the main invasive centres. This network formation resulted in an increase in the number of annual PPCI performed to 453 per million inhabitants in 2010 from 324 per million in 2009. Since 2007, there has been a rise in the numbers of PCI centres with new centres established in 29 different cities; 25 of these have performed PPCI for the last four years. There are now 207 PCI capable centres in Turkey shared among government hospitals, university hospitals and private hospitals. PPCI is performed 24/7 in 82 of these centres. In March 2011 the Ministry of Health declared PPCI as the first choice treatment for STEMI patients nationally, if transport time is less than 90 minutes.
One of the focus areas in Turkey was the organisation of the EMS. The number of general packet radio service (GPRS)-equipped ambulances has increased to 2,547, of which 913 have doctors on board, the remainder being staffed by paramedics and technicians. The average time from patient call to arrival is 12 minutes in cities. In selected SFL cities throughout the country, 112 ambulances bring the STEMI patients directly to the PCI centres. Since Turkey joined the SFL initiative, the number of PPCI performed has increased significantly in ten pilot cities and in 2010, 85% of STEMI patients were treated with PPCI. In addition, a STEMI network was created with collaboration between a number of invasive centres, non-invasive hospitals, ambulances and emergency systems.
Recently, local experienced cardiologists launched a programme educating ambulance doctors and emergency doctors. Turkey has also introduced a simulation course for young cardiologists to learn revascularisation techniques on mannequins programmed to exhibit ACS symptoms. In Turkey there is no nationwide public campaign to promote recognition of the symptoms of STEMI or to provide knowledge on PPCI. This is mainly due to the lack of complete PPCI organisation in many regions. However, local campaigns are running in two cities as a consequence of the SFL project, and a public mass media campaign will be undertaken.
The main barrier to PPCI implementation is the insufficient number of nurses and technicians for 24/7 PPCI treatment, especially in university hospitals. Furthermore, there is no additional payment for cardiologists performing PPCI. The main target for 2011 was to identify regions with an unmet need for PPCI and to invest in new catheterisation laboratories. The programme of simulation training in interventional cardiology for young cardiologists will continue.
TARGET COUNTRIES WHERE THE SFL INITIATIVE WAS LAUNCHED IN 2010
Egypt
In 2010, a National SFL Steering Committee and Task force were established. Meetings between key decision-makers throughout Egypt (e.g., leading interventional cardiologists, Minister of Health, ambulance service managers, medical device and pharmaceutical companies, as well telecommunication industry) took place to present the SFL initiative and secure ownership and financial support. Actions to unify the cost of PPCI in order to secure remuneration for the work are planned.
The two key areas of focus are medical education and the formation of a PPCI database. A questionnaire approved by the SFL European executive committee was distributed to all hospitals with PCI facilities in order to map the current situation in Egypt and set a baseline for further actions. A comprehensive and well-organised programme for guideline implementation and physician education was launched. The main target groups are cardiologists, interventional cardiologists and general practitioners. The programme activities were spread out over the whole country and ran from May-December 2011.
To review and increase the quality of care of the PCI hospitals in Egypt, a national audit committee was established. The committee will audit those PCI centres, which will apply for SFL pilot centre status. A media campaign was launched to increase disease awareness among the public. SFL information leaflets are available in physicians’ waiting rooms. Hospitals with PPCI facilities will be marked by SFL in the Yellow Pages in order to help patients to localise the relevant hospital. Transportation protocols are under preparation within hospitals, to increase the number of patients arriving at PPCI centres by ambulance.
Italy
The Italian Society of Interventional Cardiology (SICI-GISE) reported an average of 420 PPCI procedures per million inhabitants in 2009, an increase of 4.3% from 2008. Italy joined the SFL initiative in 2010, following the publication of results from a SICI-GISE nationwide registry, which showed that efficient STEMI networks cover approximately 50% of Italian regions (including Emilia-Romagna, Liguria, Lombardie and Tuscany). The primary goal is to implement and define tailored action programmes to ensure that the majority of STEMI patients have access to the life-saving indication of PPCI in target regions (Puglia, Campania, Sicily, Basilicata, and some areas of Piedmont and Veneto: approximately 19 million inhabitants). A 24/7 service for PPCI procedures at invasive facilities should be established to cover the need of the entire Italian STEMI population.
A kick-off meeting of SFL ITALIA was held in Rome in April 2010, involving around 100 key opinion leaders and health commission representatives from the target regions. Health plans, reimbursement methods and STEMI systems of care were analysed and mapped, barriers for PPCI use were identified and plans of action at a local level were designed.
In some target regions, a project for local STEMI network has officially been developed and organised through SFL ITALIA and is ready to be communicated. A cost-effectiveness analysis will be conducted in cooperation with Bocconi University, Milan in a benchmark region with a well-organised and established STEMI network, as well as in one of the SFL target regions with a newly developed STEMI organisation.
Romania
The Romanian SFL initiative is a collaboration between the Ministry of Health and the Romanian Society of Cardiology. Representatives from the Ministry of Health and the Romanian EMS are part of the SFL Romanian steering committee. In August 2010, a pilot project in five regional STEMI networks was launched (Bucharest, Cluj-Napoca, Targu-Mures, Iasi and Timisoara) incorporating approximately 50% of the Romanian population. A collaboration protocol was developed between invasive centres, ambulances, emergency systems and non-invasive hospitals in the STEMI networks. A campaign was launched to help the public recognise heart attack symptoms and act quickly. Consequently, in one year the number of PPCI increased from approximately 40 PPCI per million to 200 PPCI per million in the whole country.
In the Bucharest area the STEMI network (consisting of four invasive centres in a rotational 24/7 on-duty system) performed a total of 1,550 PPCI in a population of three million people (>500 PPCI per million) in 2010, almost reaching the SFL target. Mortality also decreased from 12% to 6.7% in the pilot regions. The proportion of reperfusion with PPCI increased from 5% in 2008 to 30% in 2011.
In Romania, a total of 11 hospitals perform PPCI 24/7. Six new invasive public hospitals do not perform PPCI at all because of a lack of trained interventional cardiologists. In 2010 an approved programme was launched to provide training and accreditation of interventional cardiologists.
A telemedicine system for ECG transmission from pre-hospital to emergency departments or integrated dispatching centres was implemented, with 800 ambulances with ECG monitoring and remote transmission up and running. Romania has a STEMI Registry (Ro-STEMI), with a good geographical coverage that has incorporated more than 20,000 patients since 1999, with data on STEMI treatment and mortality for the past 10 years. Data from Ro-STEMI showed that about 80% of STEMI patients arrive at hospital in ambulances, but more than a third of them are latecomers (>12 hours from the onset of symptoms) (http://www.cardioportal.ro).
The main barriers to implementation in Romania include poor reimbursement for PCI procedures, few catheterisation laboratories (only 16 public hospitals with invasive facilities), a low number of trained interventional cardiologists (only 35 with accreditation), poor road infrastructure, large rural areas with mountains (hard to access) and poor public awareness of AMI symptoms. Plans for 2011 involve inclusion of all STEMI patients and PPCI procedures in the Ro-STEMI Registry, continuation of the programme of institutional training in interventional cardiology for young cardiologists and definition of new regions with an unmet need for PPCI in order to invest in new catheterisation laboratory facilities. The efficiency of the system in terms of time-to-treatment and myocardial salvage will be determined based on data from the Ro-STEMI registry in the next period. Another public campaign was carried out in late 2011.
TARGET COUNTRIES WHERE THE SFL INITIATIVE WAS LAUNCHED IN 2011
Portugal
In Portugal there are 19 centres with PPCI capacity, 18 of these centres performing PPCI 24/7. The Portuguese Ministry of Health reported that on average 264 PPCI procedures per million inhabitants were performed in 2010. In Portugal there is an emergency number “112”, but on average only 23% of AMI patients are admitted to hospital by the EMS, with as few as 6% of patients using this service in some areas.
An SFL task force was created by the Ministry of Health has begun to identify barriers for PPCI network implementation at EMS and hospital level. The next step was to launch an appropriate action plan to overcome these barriers. This plan has two priorities; an operational PPCI transport network with strong communication with catheterisation laboratories, and education of the public to dial the emergency EMS number.
A new paradigm of pre-hospital transportation is currently being implemented to improve the operational network. All ambulances will be equipped with telemetry and facilities to transfer ECGs to the PCI centre so that the ambulance crew can contact the catheterisation laboratory directly. A campaign to educate the public to recognise AMI symptoms and to prompt them to call the EMS emergency number will soon be launched. This campaign has been prepared in partnership with an energy company with social responsibility concerns, which will give external visibility to the initiative. In addition, a group of volunteers will distribute leaflets with educational messages to all company desks throughout the country. Newsletters will be sent to customers of the energy company and the campaign will have media coverage to increase awareness in the population.
Comments
As seen from the progress reports, implementation processes vary between countries. One of the main goals of the SFL project is to reach the rate of 600 PPCI per million inhabitants per year. However, the incidence of STEMI may vary across Europe. Individual annual goals for PPCI numbers must therefore be set, and adjusted to the incidence of STEMI in each country and region. Increasing the overall number of patients receiving PPCI in Europe is important. However, focus should also be to optimise the quality of PPCI performance by shortening time delivery, and by establishing appropriate training of health care personnel. Furthermore, valid PPCI registries and improvement of public awareness are needed.
One of the main ideas of the SFL initiative was to recognise the importance of local community involvement when implementing new treatment strategies. Each country has different underlying financial, political, organisational and cultural bases, resulting in unique sets of challenges. Action plans should therefore be tailored to the needs and feasibility in each country.
Recent studies emphasise that PPCI is socio-economically cost-effective, regardless of the high costs to establish the technology12,13. Even if the higher initial implementation costs are not offset, the net effect may be justifiable if PPCI improves health outcomes. Additional studies are required to explore the economic consequences of PPCI treatment. Such data are important when discussing future implementation strategies with policy makers.
STENT FOR LIFE STRATEGY 2011
Support SFL implementation in the four newest countries: Egypt, Italy, Portugal and Romania;
Preparation and launching of public awareness campaigns in those countries and/or regions where an effective PPCI network is established;
Follow-up of the survey published in 2009 as a surveillance tool for the SLF progress/impact in the ESC member countries as well as in the 10 SFL countries. All ESC countries will once again be invited to answer questions on e.g., prevalence of reperfusion treatment, time delay in treatment and organisation of existing treatment. Data will be collected in 2011 and will be published in 2012.
Conclusion
Improving patient outcomes in STEMI is a critical goal, and continued efforts are needed to expand the delivery of PPCI rapidly and reliably in real-world settings. The SFL initiative provides tremendous added value to the practice of PPCI, both for the public and physicians. The barriers for implementation of PPCI vary from country to country and therefore action plans for implementation should be tailored to the specific national needs and current conditions.
Acknowledgements
The authors thank the national project managers from the following countries for their contributions and support:
Bulgaria: Project manager, Kiril Karamfilov;
Egypt: Prof. Mohamed Sobhy (country champion and President of the Egyptian Society of Cardiology); Dr. Ahmed El Shal (country project manager and ICOM Chairman); and all members of the Egyptian steering committee (from Egyptian universities centres and health authorities);
Italy: Project manager, Leonardo De Luca, Department of Cardiovascular Sciences, European Hospital, Rome, Italy;
Greece: George Parharidis (Professor of cardiology, President of the Hellenic Society of Cardiology); Lambros Michalis (Professor of cardiology, Chairman of the Hellenic Working Group of Hemodynamics and Interventional Cardiology); Dimitrios Alexopoulos (Professor of cardiology, member of the Hellenic SFL steering committee, PPCI Network of South Western Greece, Patras, Greece); John Nanas (Professor of cardiology, member of the Hellenic SFL steering committee, PPCI Network of Athens, Athens, Greece); and Georgios Papaioannou (MD, member of the Hellenic Working Group of Hemodynamics and Interventional Cardiology);
Portugal: Project Manager, Sofia de Mello. The steering committee of the Portuguese SFL project is formed by the following people: Hélder Pereira, SFL champion, President of Portuguese Association of Cardiovascular Interventions (APIC); Leitão Marques, former APIC President; Miguel Soares Oliveira, President of the Portuguese Medical Institute of Medical Emergency (INEM); Rui Ferreira, Health Ministry Cardiovascular Diseases Co-ordinator; and Dr. Carlos Aguiar, MD, member of the Portuguese Cardiology Society Direction;
Romania: Project manager, Dr. Ileana Penea. The steering committee of the Romanian SFL project is formed by the following persons: Dan Deleanu, SFL champion, president of RSC; Dragos Vinereanu, president of MoH Commission of Cardiology; Gabi Tatu-Chitoiu, vice-president of RSC and responsible with the Ro-STEMI Registry; Raed Arafat, secretary of state in the MoH and responsible with EMS in Romania; and Lucian Petrescu, head of invasive cardiology in Timisoara.
Spain: Project manager, Matias Feldman; Javier Goicolea (President of the Spanish Working Group on Interventional Cardiology); Carlos Macaya (President of the Spanish Society of Cardiology); Antonio Fernandez-Ortiz (Vice-President of the Spanish Working Group on Acute Cardiac Care);
Turkey: Prof. Dr. Ömer Kozan (President Elect of the TSC); Prof. Dr. Muzaffer Degertekin (President of TAPCI); Prof. Dr. Mehmet Aksoy (general secretary of the TSC); Prof. Dr. Engin Bozkurt (Board member of TAPCI); Dr. Orhan Koç (responsible for all Ministry of Health hospitals); Dr. Seracettin Çom (responsible for the emergency medical system); Dr. Umit Kervan (SFL representative of the Ministry of Health).
Conflict of interest statement
The authors have no conflict of interests to declare.
