Abstract
The Stent for Life Initiative was founded in September 2008 as a coalition of the European Society of Cardiology, European Association for Percutaneous Cardiovascular Interventions and Eucomed. The aim is to promote the life-saving indications for percutaneous coronary interventions – especially in all forms of acute myocardial infarction. This article describes how this initiative began.
Introduction
When the authors of this introduction finished their medical studies approximately 30 years ago, there was no effective treatment for acute myocardial infarction (besides DC countershock for ventricular fibrillation). This area of medicine has changed dramatically over these 30 years. The greatest change was the introduction of reperfusion therapy – the first truly active approach to acute myocardial infarction with ST-segment elevations (STEMI). Initially, thrombolysis was used as intracoronary infusion, later intravenously – which enabled its use in all hospitals and also in the pre-hospital setting.
The first three randomised trials1-3 had proved in 1993 that primary percutaneous coronary intervention (p-PCI) is superior to thrombolysis in the treatment of STEMI. Ten years elapsed before two larger multicentre randomised trials4,5 proved that p-PCI is also the best reperfusion strategy for distant patients, who need to be transferred from the nearest small hospital to a tertiary PCI centre. The first guidelines defining p-PCI as the default reperfusion strategy were published by the Czech Society of Cardiology in 20026, followed by the European Society of Cardiology7 and the American College of Cardiology/American Heart Association8.
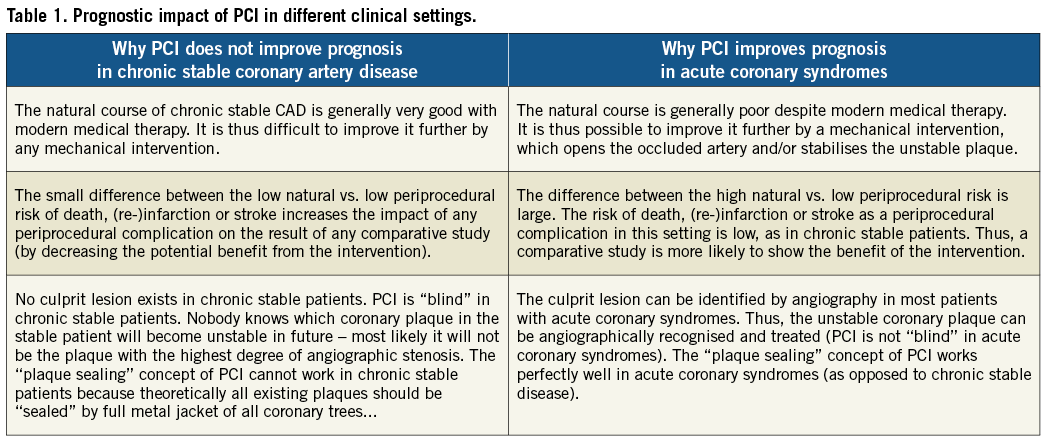
Simultaneously, evidence has been accumulating, showing the suboptimal implementation of emergent PCI for acute coronary syndromes9,10. On the other hand, the widespread use of PCI for chronic stable coronary artery disease had limited or no influence on mortality. The COURAGE11 and MASS II12 trials versus acute coronary syndromes trials have helped to evaluate the role PCI should have in modern cardiology. PCI does not improve prognosis in chronic stable coronary artery disease because the natural course is generally very good and because no culprit lesion exists in chronic stable patients. On the other hand, PCI improves prognosis in acute coronary syndromes because the culprit lesion can be identified by angiography in most patients. PCI centres should focus their resources (both human and financial) mainly on the treatment of acute coronary syndromes13. Unfortunately, PCI was used far more in symptomatic indications (without significant impact on mortality) than in prognostic indications (where it significantly improves patient outcomes).
This problem was discussed by William Wijns and Petr Widimsky in June 2008 during the ESC Board meeting in London (Table 1) and the idea for a pan-European project supporting the use of PCI in prognostic indications (i.e., in acute coronary syndromes) emerged. Thus, in 2008, the European Association for Percutaneous Cardiovascular Interventions (EAPCI) and EuroPCR together with the Working Group on Acute Cardiac Care of the European Society of Cardiology (ESC) decided to support the widespread use of acute PCI, and launched the Stent for Life (SFL) Initiative on September 13, 200814. From the very beginning, this initiative was supported by several industry partners – their current list can be seen on the official Stent for Life website www.stentforlife.com .
The first step was to review the current situation in reperfusion treatment of acute myocardial infarction in Europe. The survey, based on data from 30 countries collected in 2007, revealed extremely large differences in the implementation of reperfusion therapies among European countries15.
The second step to change the reperfusion to primary PCI followed immediately. The situation was improving quickly in many countries. In some of these, such as the United Kingdom and Slovakia, this was enabled mainly by strategic and financial support from local governments, whereas in other countries (Bulgaria, Egypt, France, Greece, Italy, Portugal, Romania, Serbia, Spain and Turkey) this was greatly facilitated by national SFL groups. Thus, now – less then four years after SFL initiation – primary PCI is already the dominant reperfusion therapy for STEMI in the majority of European countries.
Thus, the question now is: has the SFL Initiative already achieved its goals? Or are we just midway with a lot of work still ahead? We have to wait for the detailed analysis of the second European SFL survey, performed in 2011, with results becoming available late 2012. Irrespective of these results, we strongly believe that the Stent for Life Initiative should not only continue but probably even grow. After the “quantitative” phase (aimed at increasing primary angioplasty use for reperfusion therapy of STEMI) the SFL Initiative should focus on the “qualitative” parameters. Our aim should be to record systematically and to shorten the time delays, to continue to facilitate the evolution of effective regional STEMI networks. We should open the STEMI networks for other critical situations in acute myocardial infarction (AMI) (ST-depression myocardial infarction with ongoing ischaemia, AMI with acute heart failure, etc.), to facilitate implementation of new technologies and medications as sufficient evidence has been collected to prove the benefit of these new strategies for patients with AMI. We believe that the Stent for Life Initiative is here to stay for the benefit of all European patients with AMI.
Conflict of interest statement
The authors have no conflicts of interest to declare.