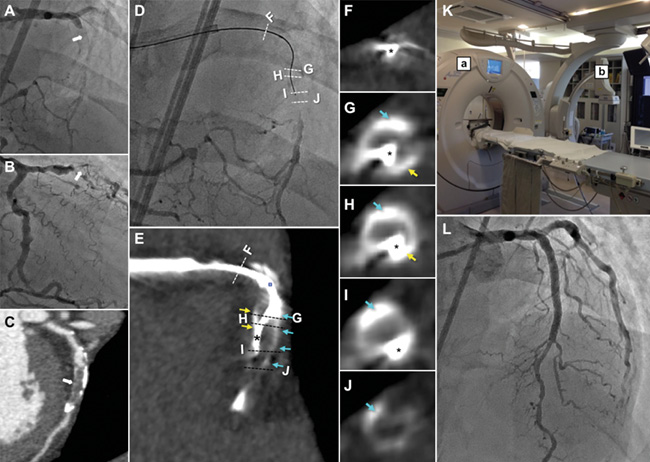
Figure 1. Coronary angiogram with bilateral injection (A & B) and pre-procedural curved multiplanar reformation image (C). White arrows demonstrate CTO of the LAD with severe calcification. When the guidewire reached the distal lesion of the CTO, just before the distal true lumen (D), an intraprocedural CCTA was performed on site without contrast injection (E). Matching cross-sectional CCTA images showed the location of the guidewire in the coronary artery including CTO segments (F-J). Cross-sectional CCTA images at the wire tip level clearly showed the guidewire inside the intimal plaque of the CTO (H & I). The asterisks and blue and yellow arrows indicate the guidewire and calcified plaques, respectively. The CCTA system in the catheterisation room (K) comprised a CT scanner (a) and a coronary angiography system (b). Final post-procedural angiogram after successful stent implantation (L).
A 55-year-old man diagnosed with chronic total occlusion (CTO) of the left anterior descending artery was admitted, and we attempted antegrade CTO intervention using bilateral femoral injection (Figure 1A-Figure 1C). When the guidewire was deemed to have reached the end of the distal CTO (Figure 1D), coronary computed tomographic angiography (CCTA) without contrast injection was performed. This involved a 640 multislice CT scanner applying double-slice technology (Aquilion ONE™; Toshiba Medical Systems, Otawara, Japan) and a coronary angiography system which allows a CT scan to be evaluated during intervention without the need to move the patient on the table (Figure 1E-Figure 1K, Moving image 1). CCTA clearly showed the location of the wire tip in intimal plaques, where the guidewire was slightly deviated but definitely differentiated from the calcified vessel wall (Figure 1G-Figure 1I). After correction of the direction, we confidently advanced the guidewire, successfully crossing the CTO lesion, and finished 3.0×38 mm stent implantation (Figure 1L). Total radiation dose was 33.34 mSv and the dose for CCTA was 1.55 mSv.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Real operation of the CCTA system.