
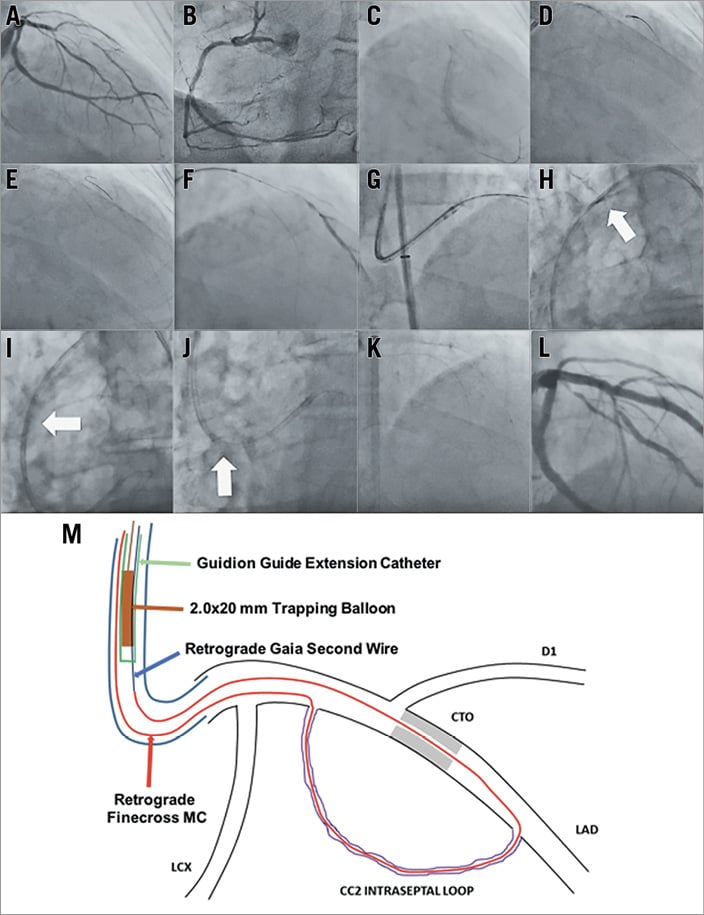
A 70-year-old man with a history of hypertension and dyslipidaemia presented with Canadian Cardiovascular Society (CCS) class III angina of six-month duration. Coronary angiography revealed a CTO of the left anterior descending artery (LAD) without interventional collaterals from the right coronary artery (RCA) (Panel A, Panel B, Moving image 1, Moving image 2). The J-CTO score was 2 (lesion length 20 mm, blunt stump) and the distal LAD filled by well-developed ipsilateral septal collateral channels. Myocardial perfusion imaging confirmed viability and clinically significant ischaemia in the LAD territory and the patient was scheduled for CTO recanalisation. A single guiding catheter transfemoral approach was used with an 8 Fr EBU 4.0 guiding catheter (GC) (Launcher®; Medtronic, Minneapolis, MN, USA). Selective contrast injection through a Finecross® microcatheter (Terumo Corp., Tokyo, Japan) delineated the course of a CC21 septal collateral (Panel C, Moving image 3). A Fielder FC wire (Asahi Intecc, Aichi, Japan) was advanced to the distal true lumen and the Finecross followed (Panel D, Panel E, Moving image 4, Moving image 5). Retrograde wiring with Gaia Second and Gaia Third (Asahi Intecc) wires proved unsuccessful. The CTO was then approached antegradely and a 5 Fr Guidion (IMDS, Roden, the Netherlands) guide extension catheter (GEC) was advanced through the 8 Fr EBU to optimise support. Antegrade advancement of a Gaia Second guidewire supported by a Finecross microcatheter failed to re-enter into the distal true lumen (Panel F, Moving image 6). Eventually, a retrograde Gaia Second guidewire crossed the occlusion entering the aorta and was then advanced inside the EBU (Panel G, Moving image 7). However, the retrograde Finecross microcatheter could not be advanced further through the occlusion to facilitate wire externalisation. The potential solutions to overcome this problem would be the following. 1) Use of a new or another type of microcatheter retrogradely. 2) Rendezvous or tip-in technique inside the GC. In this case a microcatheter is advanced antegradely inside the GC and the retrograde wire is steered inside its lumen. The antegrade microcatheter is then advanced to the distal true lumen over the retrograde wire, the retrograde wire and microcatheter are retrieved and a wire is advanced antegradely to enable procedure completion. 3) Trapping technique with a second GC placed into the same occluded artery ostium (ping-pong technique); the retrograde wire is advanced inside this second GC that contains no other material and therefore trapping can be performed enabling retrograde microcatheter advancement and wire externalisation2. The availability of the unique 4 in 5 Fr Guidion GEC challenged us to pursue a novel technique. We proceeded by advancing the retrograde wire inside the lumen of the Guidion (Panel H, Moving image 8). A 2.0×20 mm balloon was then advanced inside the Guidion and inflated to 8 atm trapping the retrograde wire (Panel I, Moving image 9). The Finecross could then be advanced inside the GC, facilitating RG3 wire (Asahi Intecc) externalisation and uneventful completion of the procedure (Panel J, Panel K, Panel L, Moving image 10, Moving image 11, Moving image 12).
To the best of our knowledge, this is the first description of a case involving single GC retrograde CTO recanalisation and trapping technique. Our technique (schematically illustrated in Panel M) is feasible and easy to use, requires single arterial access and provides one more tool in the armamentarium of CTO operators.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1 (linked to panel A). Diagnostic moving image, left system.
Moving image 2 (linked to panel B). Diagnostic moving image, right coronary artery.
Moving image 3 (linked to panel C). Selective contrast injection to delineate the course of septal collaterals providing the distality of the occluded LAD.
Moving image 4 (linked to panel D). Retrograde wire advanced to the distal true lumen, Finecross MC follows.
Moving image 5 (linked to panel E). Finecross MC advanced to the distal cap.
Moving image 6 (linked to panel F). Antegrade Gaia Second supported by Finecross MC; Guidion guide extension catheter for support optimisation; retrograde selective contrast injection reveals antegrade wire subintimal position.
Moving image 7 (linked to panel G). Retrograde wire entering the aorta and advanced inside the guiding catheter.
Moving image 8 (linked to panel H). Retrograde wire advanced inside the lumen of the guide extension catheter to facilitate “modified rendezvous technique”.
Moving image 9 (linked to panel I). Trapping balloon inside guide extension catheter facilitated Finecross advancement inside the guiding catheter.
Moving image 10 (linked to panel J). Finecross MC advanced inside EBU guiding catheter.
Moving image 11 (linked to panel K). RG3 wire externalised; Finecross MC advanced antegradely to facilitate wire exchange.
Moving image 12 (linked to panel L). Final angiographic result after stent implantation and post-dilatation with 4.0×10 mm NC balloon.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1 (linked to panel A). Diagnostic moving image, left system.
Moving image 10 (linked to panel J). Finecross MC advanced inside EBU guiding catheter.
Moving image 11 (linked to panel K). RG3 wire externalised; Finecross MC advanced antegradely to facilitate wire exchange.
Moving image 12 (linked to panel L). Final angiographic result after stent implantation and post-dilatation with 4.0×10 mm NC balloon.
Moving image 2 (linked to panel B). Diagnostic moving image, right coronary artery.
Moving image 3 (linked to panel C). Selective contrast injection to delineate the course of septal collaterals providing the distality of the occluded LAD.
Moving image 4 (linked to panel D). Retrograde wire advanced to the distal true lumen, Finecross MC follows.
Moving image 5 (linked to panel E). Finecross MC advanced to the distal cap.
Moving image 6 (linked to panel F). Antegrade Gaia Second supported by Finecross MC; Guidion guide extension catheter for support optimisation; retrograde selective contrast injection reveals antegrade wire subintimal position.
Moving image 7 (linked to panel G). Retrograde wire entering the aorta and advanced inside the guiding catheter.
Moving image 8 (linked to panel H). Retrograde wire advanced inside the lumen of the guide extension catheter to facilitate “modified rendezvous technique”.
Moving image 9 (linked to panel I). Trapping balloon inside guide extension catheter facilitated Finecross advancement inside the guiding catheter.
