The injection of contrast media within a CTO has been a valuable tool in the operator’s armamentarium for overcoming challenging procedural scenarios ever since the development of the contrast-guided subintimal tracking and re-entry (STAR) technique in 20082. This technique was based on the forceful injection (via an over-the-wire balloon) of a large amount of contrast media (3-4 ml) with the intention to hydraulically recanalise the occlusion. This is achieved by the creation of a tear in the flap separating the false and true lumen using dye injection. Since this approach was associated with extensive dissections and unpredictable true lumen re-entry, restenosis rates on follow-up were found to be high, and contrast-guided STAR was soon abandoned 3.
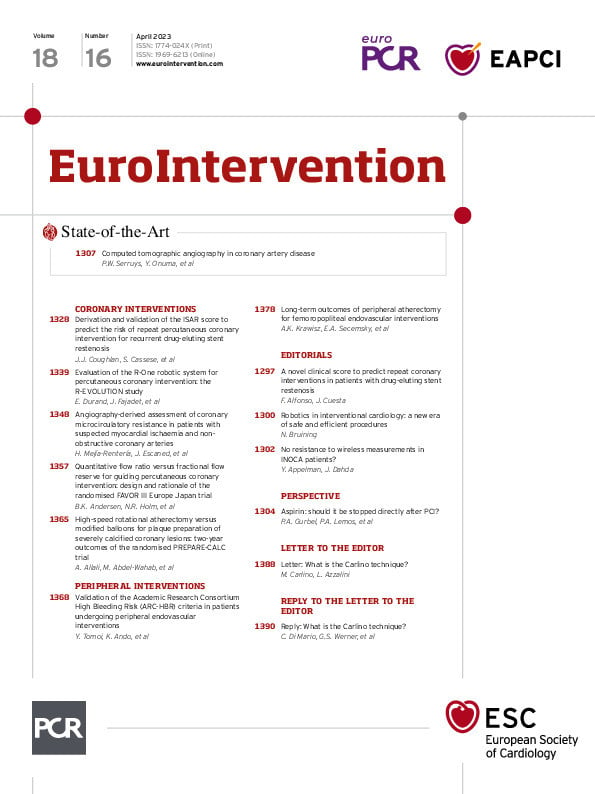
The disruptive idea of injecting contrast media into the occlusion had, however, been seeded in the CTO community, and the technical approach was improved and later refined in what is currently known as the “Carlino technique”4. Briefly, a small (<0.5 ml) volume of contrast is gently injected through a microcatheter with a two-pronged purpose (Figure 1A). First, if the microcatheter is in the intraplaque space, the contrast injection will follow the path of least resistance (i.e., loose tissue segments within the occlusion) and will modify plaque compliance by softening it, with the aim of making the subsequent wire/microcatheter advancement easier. This application of the Carlino technique is used in the context of an impenetrable proximal/distal cap or in difficult-to-negotiate (calcified) areas of the occlusion (Figure 1B). Secondly, if the microcatheter is located in the extraplaque space, 2 possible angiographic patterns can be recognised. A “storm cloud” appearance is indicative of a transient increase of wall permeability in a vascular structure that is too small to accommodate even a reduced volume of contrast (typically, a small branch) (Figure 1C). A “tubular” staining is, on the other hand, indicative of an accumulation of the contrast in a larger vessel, along subintimal planes (Figure 1D). In this context, the operator can judge where their gear is located and redirect (storm cloud dissection) or continue advancing it (tubular dissection). Importantly, and at variance with contrast-guided STAR, the injection force is tailored to the perception of resistance and visual feedback.
Although a clear distinction exists, in the authors’ eyes, between the rudimentary and now-abandoned contrast-guided STAR and the latest evolution of intraocclusional contrast injection, we have unfortunately witnessed confusion in the CTO community, with the concept of hydraulic dissection (the signature feature of contrast-guided STAR) being applied to the contemporary Carlino technique1. As previously described, the gentle injection of minimal amounts of contrast is not sufficient to cause hydraulic dissection and is aimed at modifying plaque compliance and/or providing topographic information with regards to equipment location within the vessel architecture.
The real-world use of the Carlino technique by “hybrid operators” and its integration within established crossing algorithms5 is a testimony to its usefulness and safety. We hope that the clarifications contained in the present manuscript will contribute to further disseminate good clinical practice in the field of CTO percutaneous coronary intervention.
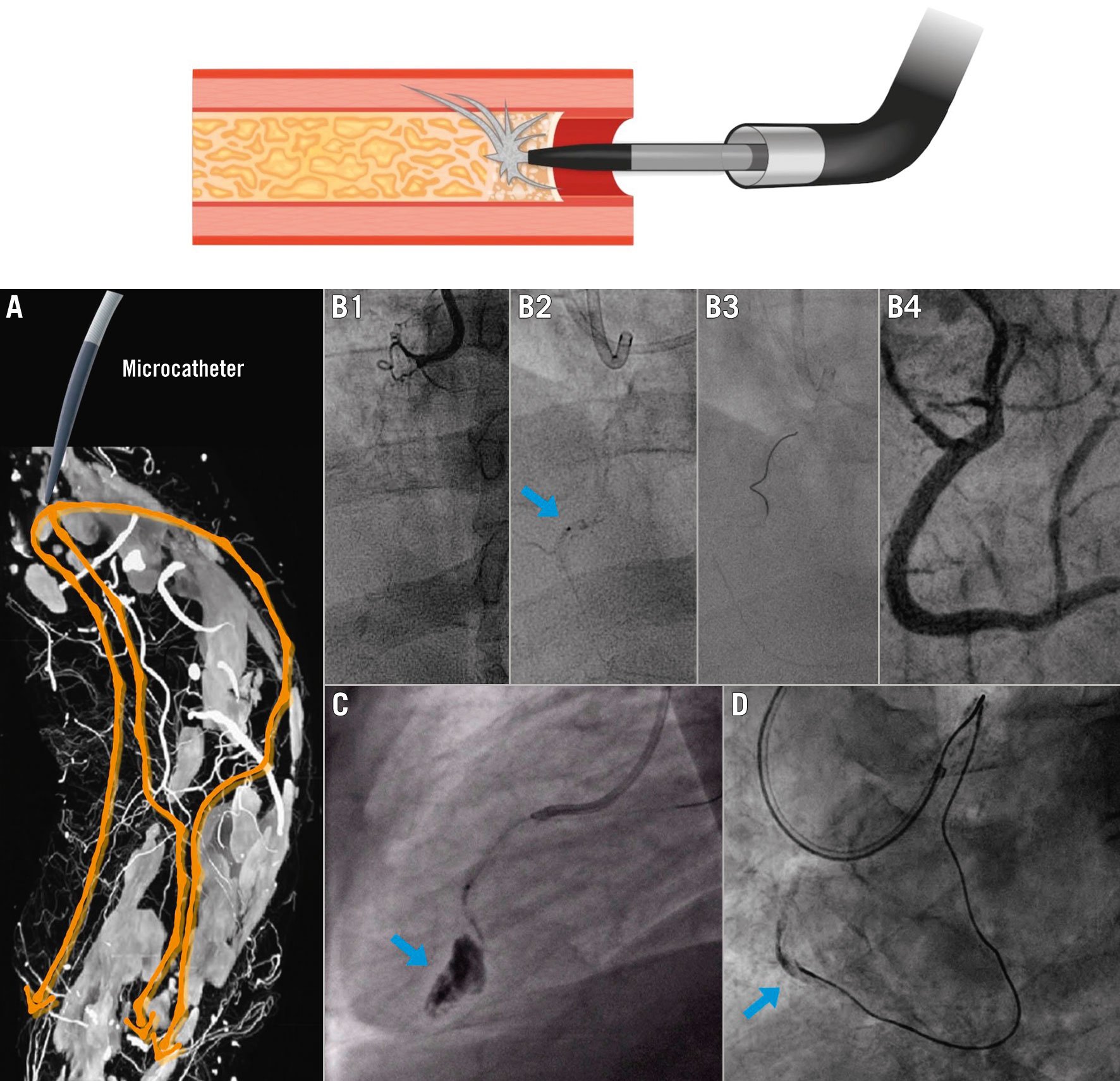
Figure 1. Applications of the Carlino technique. Top panel: a small amount of contrast media is injected through the microcatheter to modify and/or provide information about the occlusive plaque. A) A gentle injection of small amounts of contrast distributes along the paths of least resistance within the occlusion (arrows), represented by loose fibrous tissue. B1-B4) Use of the Carlino technique to modify plaque compliance: B1) Flush ostial right coronary artery (RCA) CTO. The retrograde approach is performed, and a high-tipload guidewire cannot negotiate an area of marked calcification in the mid-RCA. B2) The Carlino technique is performed (arrow), after which (B3) a low-tipload polymer-jacketed wire easily tracks trough the plaque and reaches the antegrade guide catheter. B4) Final result. C) Carlino technique in a small branch: “storm cloud” dissection (arrow). D) Carlino technique in a large vessel (RCA): “tubular” dissection (arrow). CTO: chronic total occlusion. Reproduced with permission from “A guide to mastering Antegrade CTO PCI Part 2” by James C. Spratt (https://books.apple.com/gb/book/a-guide-to-mastering-antegrade-cto-pci-part-2/id1474965405).
Conflict of interest statement
L. Azzalini received honoraria from Teleflex, Abiomed, Asahi Intecc, Philips, GE Healthcare, Abbott Vascular, and Cardiovascular Systems, Inc. The other author has no conflicts of interest to declare.