![]()
Abstract
The aim of this report is to analyse trends in Italian cathlab activity between 2010 and 2015. Data were obtained from the national database of the Italian Society of Interventional Cardiology (GISE), which includes 97% of Italian cardiac catheterisation laboratories. The number of percutaneous coronary interventions (PCI) has remained relatively stable in the past five years. We have observed a significant increase in the number of primary PCI (pPCI) from 471.5 to 557.5 per million inhabitants with a consequent reduction of rescue primary PCI/fibrinolysis. One of the possible explanations for this might be the extensive networking for primary PCI and the adoption of Stent for Life initiatives in five regions. There has been a notably increased use of drug-eluting stents and, despite the fact that the introduction of bioabsorbable vascular scaffolds is recent, there is a slight, progressively positive trend. Invasive physiologic evaluation of coronary stenosis has markedly increased. Radial artery access has become the default option for PCI and for pPCI. In the last five years, TAVI procedures have doubled in number, while MitraClip and mitral repair procedures have shown a fivefold increase. Left atrial appendage (LAA) occlusion procedures have more than doubled in four years.
Demographics and organisation
The data presented are representative of the Italian cathlab activity of the last five years. The current national profile is that 1,021 operators work in 271 accredited cathlabs accounting for more than 300×103 procedures/year performed on a population of about 60×106 inhabitants. The Italian National Registry of Interventional Cardiology is managed by the Italian Society of Interventional Cardiology (GISE) under a strict procedure of data collection, validation, audit and publication1,2. Participation in the Registry is voluntary, with all procedures carried out in each centre registered in the database. GISE began collecting data of cathlab activities in 1981 using a paper-based registry. An electronic registry was launched in 2004 and has since been actively used. Cathlab managers are provided with a secure and private profile to enter or upload data activity at specified time intervals, as well as to review historical data. Data collection by this registry covers 97% of all Italian cathlabs. The Registry contains over 300 fields, organised in a relational database, which are regularly updated by GISE to account for recent innovations or new data to be collected.
From a technical point of view, the system contains a number of innovative features:
– Upload and verification. The Registry allows on-line verification of data consistency and completeness, with output issued back to the sender.
– Data coherence. The Registry implements a number of automatic rules for checking coherence of data entered. This greatly simplifies the audit process and turns out to be very useful, especially in the case of manually entered data that are typically error-prone. Additionally, users benefit from tool tips and on-line explanations in any field. Automatic calculations are also available, ensuring data consistency.
– Trends monitor. Each of the main fields contains reference to the previous year’s activity. Users and administrators can immediately recognise differences and deviations. Deviations that exceed a certain threshold in a specific field are pointed out to the user and generate an alert, again simplifying the audit process.
– Secure access. Users are granted a secure and private profile to enter or upload activity data, as well as to review their historical data. Special profiles are granted to administrators able to combine and review data both by single cathlab or by region.
All of the data are analysed by an independent CRO, and published annually in Giornale Italiano di Cardiologia Invasiva (GISE’s journal) and on the Society’s public platform website.
In the future, our first goal would be to complete the list of queries proposed by the EAPCI organisation. Another aim for the future is that, in order to render data management as complete as possible, as many cathlabs as possible keep the data entry up to date. In keeping with the aim of making data entry and access easier for both cathlabs and database administrators, another goal would be to consolidate collaboration with regional authorities. This would allow a concrete link between local databases and the diagnosis-related groups (DRG) system of the National Health Service, thus providing the basis for setting up automatic follow-ups based on a patient’s discharge from hospital.
DATA QUALITY CONTROL
The quality of the data in the database is controlled by means of on-site monitoring of 10% (from 2010 to 2013) and 20% (from 2014-2015) of randomly selected laboratories every year. The source data are verified by independent monitors who check the consistency between the declared data and the original source documentation. In the small percentage of centres which undergo an audit, we have found some inconsistencies that were, in all cases, data entry errors and none that had any direct impact on the final result. Such a thorough check, both automatically by default corrections of the system as well as double-checked by the auditors, underlines the high performance of the database software.
Coronary interventions
Numbers of coronary angiographies (CAG), percutaneous coronary interventions (PCI) and primary percutaneous coronary interventions (pPCI) in 2010-2015 are presented in Figure 1. The number of coronary angiographies and PCI has remained stable in the last five years2. This indicates optimal balancing between patient need and health system offer. The ratio between PCI and CAG has only slightly increased, perhaps indicating the possibility of better patient selection based on clinical indication. The notably increased number of multivessel PCI is likely to be motivated by the recognition of the prognostic importance of complete (functional) revascularisation, as well as possibly being linked to the increasing number of centres and operators dedicated to the treatment and recognition of the importance of chronic total occlusion.
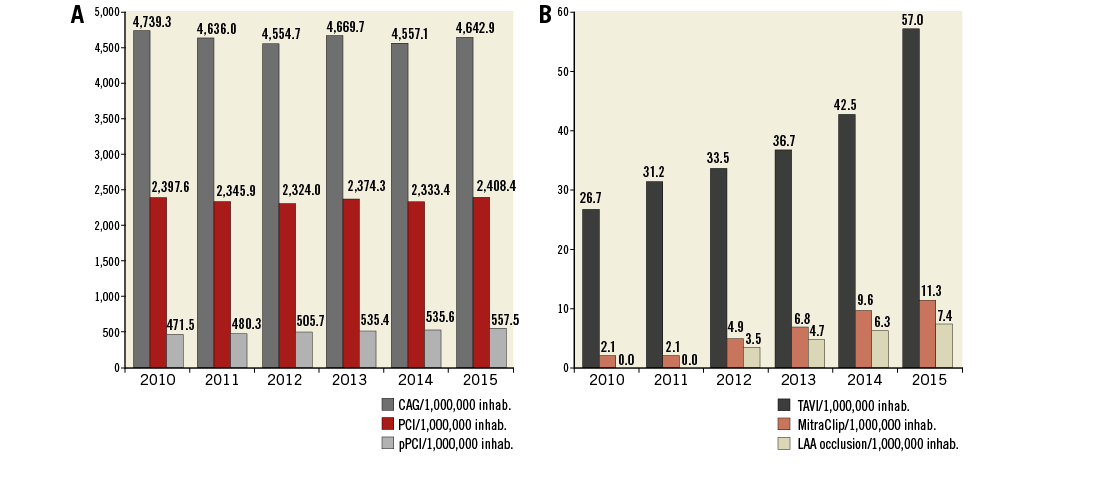
Figure 1. Trend of coronary and structural interventions per 1,000,000 inhabitants in the last five years. A) Coronary interventions per 1 million inhabitants in Italy, 2010-2015. B) TAVI implantations, MitraClip implantations and left atrial appendage occlusion procedures per 1 million population in Italy, 2010-2015. CAG: coronary angiography; PCI: percutaneous coronary intervention; pPCI: primary percutaneous coronary intervention
The number of pPCI has gone up by 15% in the last five years, increasing from 471.5 to 557.5 (p<0.001) per million inhabitants, approaching the target proposed by the 2014 European Society of Cardiology guidelines3 of 600 pPCI per million inhabitants, with a dramatic reduction of fibrinolysis procedures and rescue PCI (Table 1). Two possible main players may have impacted on this improvement of the clinical practice. First is the systematic diffusion and improvement in STEMI network organisation (Figure 2), and the adoption of Stent for Life initiatives in five target regions. Specifically, in the five target regions (Piedmont, Veneto, Sicily, Puglia, Campania) between 2010 and 2015, we observed the following increases: 24% in Piedmont, 14% in Veneto, 27% in Sicily, 28% in Puglia and 38% in Campania (national increase 15%). Two of these regions (Piedmont and Sicily) exceeded the target of 600 pPCI per million inhabitants. Second, in 2008 there was still a large number of areas lacking any sort of network for the management of STEMI patients. Figure 2 highlights the increase in both the size of the networks as well as the number of networks available nationally in 2013.
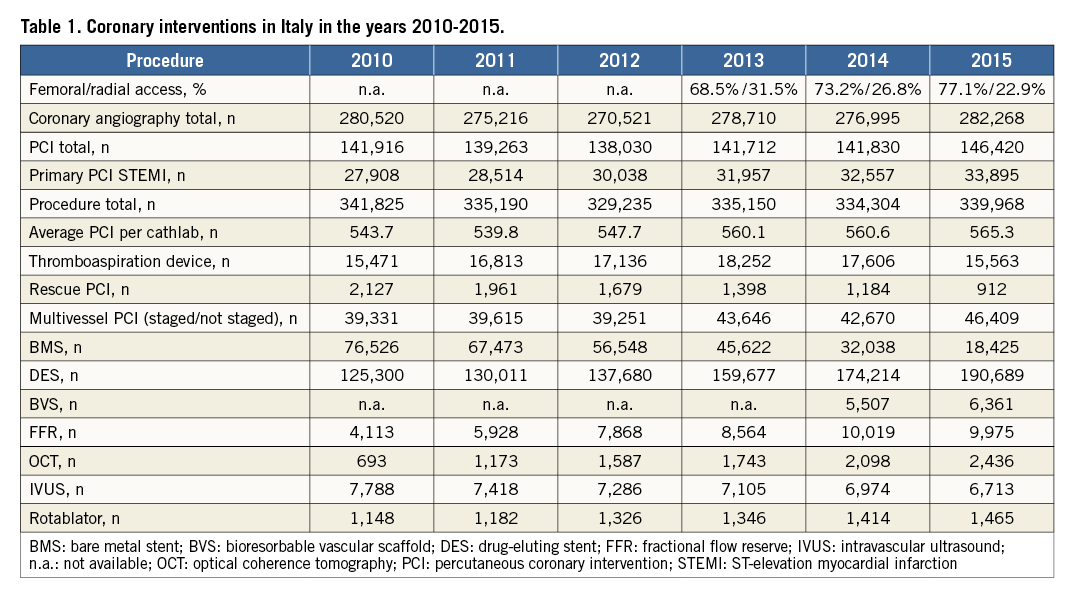
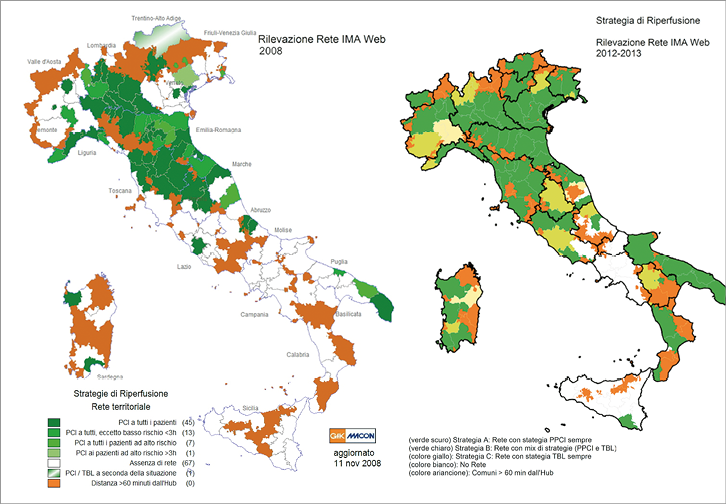
Figure 2. The development of the STEMI network in Italy between 2008 and 2013. This image compares the development and the diffusion of the nationwide STEMI networks in Italy between 2008 and 2013. The dark green sections depict the areas in which the networks are implemented and where pPCI is the preferred therapy. The two maps highlight the increase in the size of the networks as well as the number of networks available nationally. The orange areas are of note as, given the complex territories, these are areas in which the hub is more than an hour away (usually mountainous or very rural areas). The white areas have significantly decreased in the timescale represented in the two maps. These areas represent the territories and regions in which no network or any sort of organised coordination has been established. At present this is limited to southern areas. The data were extracted from the RETE IMA Web, which is one of the GISE strategic projects. The first edition was in 2008, with a second evaluation in 2013.
From a procedural point of view, we should underline some other technical aspects. While the percentage of pPCI increased by 17.7% from 2010 to 2015, the number of procedures performed using a thrombus aspiration device levelled off between 2010 and 2013, and even started declining in 2014. This phenomenon has possibly been driven by the hazy data published, which in turn may have had a confounding effect on operators. The use of drug-eluting stents increased markedly (p<0.001) thanks to the positive feedback in the literature, with a consequent parallel reduction in bare metal stent use (p<0.001). Bioabsorbable vascular scaffolds were introduced in Italy in 2014, and the two years of data observed have shown a slight positive trend. Physiologic evaluation by fractional flow reserve (FFR) has more than doubled, despite the fact that it is underused. One possible explanation is the absence of dedicated reimbursement. Intravascular ultrasound imaging use has slightly decreased, in favour of a significant increase in optical coherence tomography (OCT) (Table 1). As in the case of FFR, there is no dedicated reimbursement programme for these imaging techniques.
In the past five years, the radial approach has become the go-to technique for coronary PCI and pPCI, and has been used in 77.1% of procedures.
Structural heart interventions
Figure 1B provides data on structural heart interventions, which are summarised in Table 2.
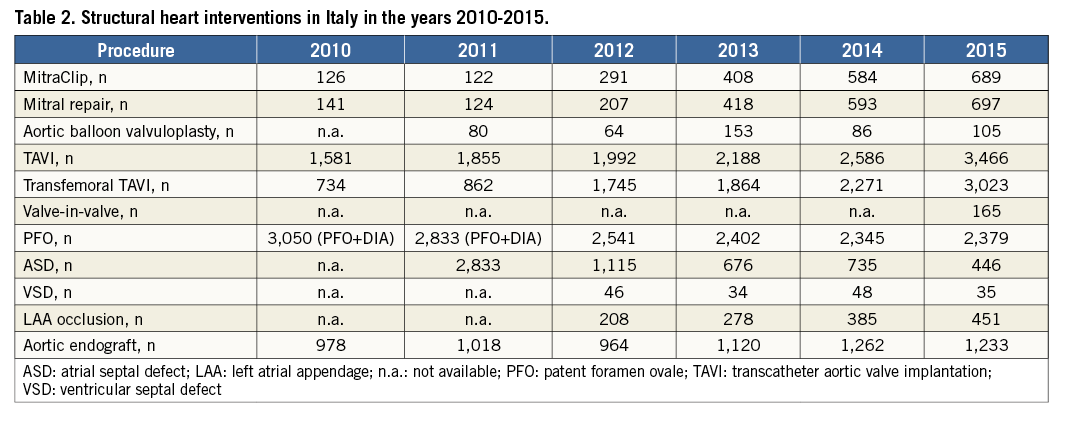
Transcatheter aortic valve implantation (TAVI) procedures have doubled from 2010 to 2015, increasing from 26.7 to 57 per million inhabitants (p<0.001), the vast majority being carried out via a transfemoral approach. The number of 57 TAVI procedures per million inhabitants is in line with other Western European country averages. Despite the positive trend of this structural interventional procedure, it appears underused on the basis of the theoretical necessity4,5. It must be emphasised that some heterogeneity exists on a regional basis. Due to health organisational constraints and costs, some Italian regions offer easier access to TAVI than others.
In 2015 the number of TAVI procedures in previous biological valve prostheses (“valve-in-valve” percutaneous procedures) was collected in the GISE database. It is quite probable that the number of these procedures will grow significantly in the near future.
The number of MitraClip® (Abbott Vascular, Santa Clara, CA, USA) procedures has shown a fivefold increase in the last five years, rising from 2.1 to 11.3 per million inhabitants.
The number of left atrial appendage (LAA) occlusion procedures has shown a slight increase in the last four years. Nevertheless, the number of LAAO procedures appears significantly low in relation to potential candidates.
It should be underlined that, at present, there is no dedicated reimbursement for these procedures provided by the Italian National Health System (SNN).
We should highlight that collaboration between GISE and policy makers has led to a steady and progressive reduction in the cathlabs at low activity volume that perform fewer than 400 PCI/year from 37% in 2011 to 26% in 2015. This work is ongoing.
Conclusion
Over the last five years, cathlab activity in Italy has consistently increased with a marked improvement in the technology applied. The notable increase of pPCI is probably due to the effort to improve cathlab organisation and to enhance the diffusion and efficiency of the territorial network for STEMI management (e.g., the RETE IMA Web project). The impressive diffusion of transcatheter strategies for the treatment of structural heart disease reflects the technological evolution and results in more opportunities to treat complex patients with high surgical risk.
Each individual national database in Europe, such as the national database of the Italian Society of Interventional Cardiology (GISE), remains an irreplaceable tool to evaluate and interpret the direction of interventional cardiology in Europe.
Conflict of interest statement
S. Berti is a proctor for St. Jude Medical and Edwards Lifesciences. The other authors have no conflicts of interest to declare.
