![]()
Abstract
Since 1990 The Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology has presented a yearly report on the data collected in the National Registry, with online support since 2010. The Steering Committee has analysed all data provided voluntarily by institutions, which consisted of a total of anywhere between 105 and 113 hospitals. Medical care was provided to a population of 46.8 million inhabitants in 2015.
During this period, diagnostic procedures increased progressively from 2010, reaching a maximum of 145,836 in 2015, 86% (125,484) corresponding to coronary angiograms. This means a ratio of 3,127 diagnostic studies per million inhabitants and 2,746 coronary angiograms per million inhabitants. Total percutaneous coronary interventions have increased to 67,671 procedures, with a ratio of 1,466 per million inhabitants where 18,418 were carried out during the acute phase of myocardial infarction (21.7%). Radial access has been successfully implemented in up to 73.8% of diagnostic procedures and 76.1% of percutaneous interventions.
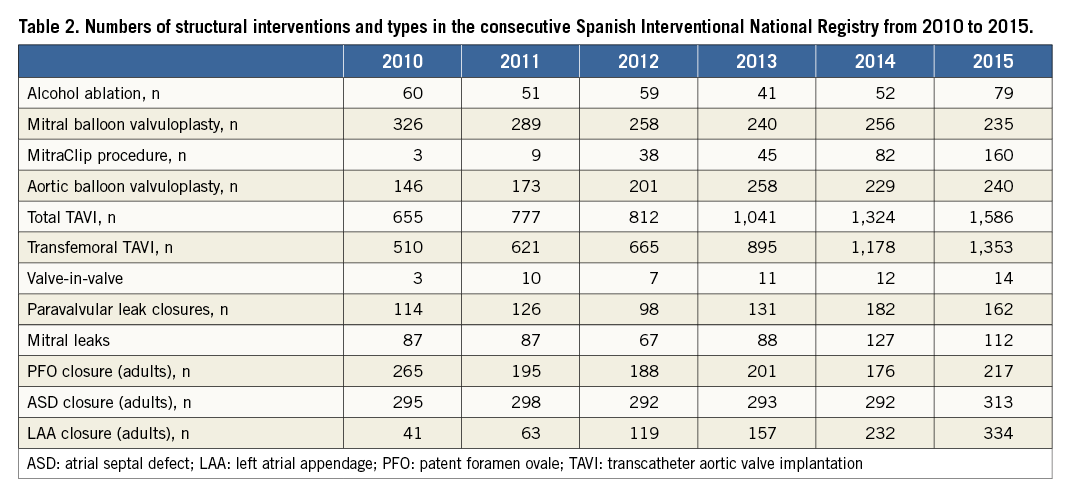
Concerning structural interventions such as septal defects, valve interventions and closure of left atrial appendage, these have had a marked evolution over time, with a total of 1,586 TAVI and 334 LAA closure procedures performed in 2015.
Demographics and organisation
The Spanish Society of Cardiology Working Group on Cardiac Catheterization and Interventional Cardiology started the National Registry in 1990 which has been voluntarily completed by interventional cardiologists from all of the 17 Spanish autonomous communities. Results are published during the annual meeting organised by the Working Group. From 2010 the register offered online support through the website to all participants to incorporate data from their annual healthcare activity, but without audit. The results of the analysis, after they have been automatically collected and error-checked by Working Group dedicated personnel, are available at the corresponding section of the Working Group on Interventional Cardiology within the website of the Spanish Society of Cardiology (www.secardiologia.com).
The public presentation during the annual meeting of the Working Group and the interaction with all the members, especially the person responsible for its future publication, works as a self-control mechanism and data are in fact checked again before publication. There is no specific cross-analysis with other databases. Most of the main variables are compared among the 17 different autonomous communities and, during a period of two months, the members of the committee of the Working Group (four people) review all data and make enquiries to participants about discordant numbers before publication. Each centre can then always review its own data using the personal password used to complete the database and request correction(s) during this period. Definitive results are published in a special issue of the Revista Española de Cardiología1.
The register includes different variables such as the number and type of interventions performed in most of the Spanish public hospitals or private centres and the number of people forming the staff of the cathlabs.
The intrinsic and fast evolution of the techniques and devices used in interventional cardiology has been followed by small changes in the number and type of variables collected.
The numbers referring to the total Spanish population in the National Registry as well as all comparisons carried out between communities are based on the total estimated population up to 1 January of each year from the Instituto Nacional de Estadística. The Spanish population to 1 January 2016 has been estimated to be 46,624,382 inhabitants.
During this period between 106 and 113 centres completed the official file. From the 77 public health hospitals developing interventional cardiology, 76 of them completed the data during this complete six-year period. Despite the fact that we do not have exact data about the total number of cathlabs not reporting in Spain, we know that more than 85% of the total interventional activity in cardiology takes place in public hospitals (Table 1).
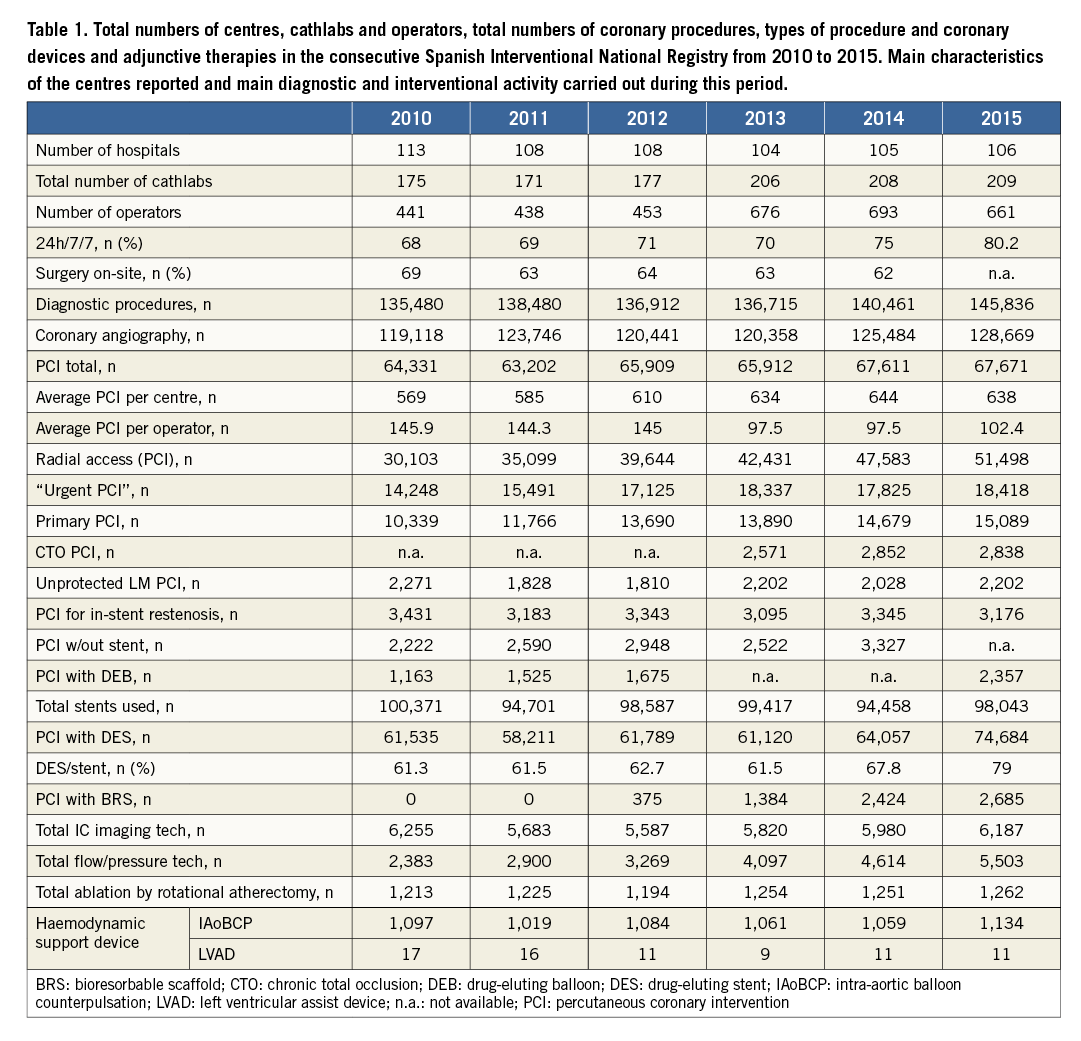
In 2015, a total of 209 cathlabs in 106 centres participated in the registry: 22 were hybrid rooms and 55 (26.3%) shared healthcare activity with other specialties. In 2015, 64 centres (60%) performed more than 1,000 diagnostic procedures. The mean value of PCI per centre was 638 with a bimodal distribution when we consider PCI volume per centre (Figure 1). The mean value of PCI per operator was 102.4.
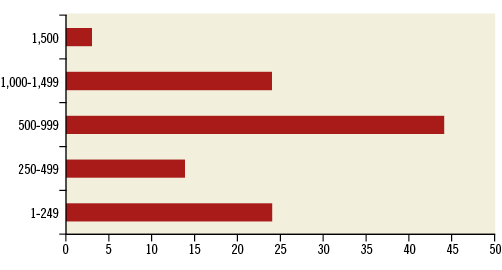
Figure 1. Number of centres reporting their activity during 2015 according to the total number of PCI per year.
At the end of this period, a total of 661 physicians were reported as working in these 106 cathlabs, with 425 (64.2%) having the Spanish Accreditation in Interventional Cardiology. Since 2005, accreditation has been driven by the members of the current and immediately previous Working Group. There is a formal statement from the Sociedad Española de Cardiología with the specific requisites established to become an accredited Spanish interventional cardiologist. Once the candidate submits all the data, the members of the Accreditation Committee which meets at least every six months evaluate both initial candidates and also the re-accreditation process. Concurrently, there is a progressive adoption of the ESC/EAPCI eLearning programme. This same Accreditation Committee evaluates hospitals as Accreditation Centres which permits Interventional Fellowship formation under the auspices of the Working Group.
In 2015, a total of 508 specialised nurses and 94 X-ray technicians were also reported. During this period, we noticed a clear increase in the total number of cathlabs without an increase in the total number of centres participating in the registry. This matched the increasing ratio of cases per centre (from 569 to 638) and also the progressive decrease of cases per operator ratio. The total number of operators experienced a rapid increase of more than 50% over the six years. Data showing the availability of operators 24 hours a day during the whole week in the centres reporting to the registry demonstrate a progressive rise from 60 to 80% at the end of the period studied.
The results of the procedures reported in the registry during this period of six years about types of coronary intervention and structural intervention are reported in Table 1 and Table 2, respectively.
Coronary interventions
TOTAL DIAGNOSTIC PROCEDURES
The period analysed showed a progressive increase in coronary procedures during the last two years despite the fact that the steady marked increase in total diagnostic procedures clearly ended after 20072. Radial access was progressively implemented during the study period from 56.6% in 2010 to 73.8% at the end of 2015 (Figure 2).
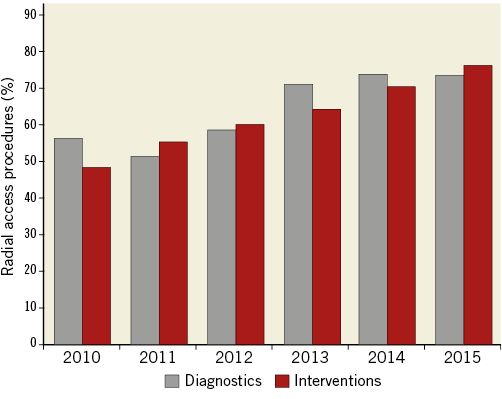
Figure 2. Proportion of procedures performed by radial access, diagnostic and interventional, in the consecutive Spanish Interventional National Registry from 2010 to 2015.
TOTAL CORONARY INTERVENTIONS
The gradual increase of coronary studies and interventions reported up to 20072 has changed little during the last six years, increasing up to 67,671 procedures in 20151. This occurred mainly due to the progressive increase of PCI during the acute phase of MI and especially because of an increase in primary PCI. We want to mention that to date there are specific, but different, programmes of primary PCI in 14 of the 17 Spanish autonomous communities, all of them supported by the Stent for Life Initiative in Europe3. Surprisingly, there was no important increase in complex PCI during this period, complex procedures being those corresponding to chronic total occlusion PCI and unprotected left main angioplasty. This could be due to its restricted definition in our registry (bifurcation lesions or debulking techniques for example are not included), to reporting bias, and also because the main increase in activity has been driven by acute PCI that generally involves non-complex PCI. Table 1 reveals no increase in restenosis cases treated by PCI in spite of the constant evolution of total PCI procedures. Therapeutic procedures also showed a positive progression of radial access, up to 76% of the total number of PCI cases in 2015.
STENTS AND CORONARY DEVICES
In Spain in 2010, more than 100 thousand stents were delivered for the first time; however, this number was not reached in any of the following years, probably due to the lower number of stents used per patient (1.6 in 2010 to 1.4 in 2014)2.
The number of drug-eluting stents (DES) was nearly 80% in 2015, being 7.5% higher than we observed in 2010. Bioresorbable scaffolds (BRS) began being used in 2012, and their use progressively increased during the study period, although this corresponds to only 3.9% of all coronary stents used in 2015. It is important to state that 80% of the stents registered are from Public Health Insurance. The Spanish National Health System does not have a reimbursement system, as it is funded by the national tax system. Spain is administratively divided into 17 autonomous communities. All of these communities have their own budget for health purposes and activities, and a portion of these budgets is dedicated for hospital practices. This includes stents but also TAVI or adjunctive techniques such as imaging or functional assessment tools.
ADJUNCTIVE TECHNIQUES DURING CORONARY INTERVENTIONS
The steady state detected in the use of imaging techniques during PCI in fact conceals two opposite trends: an important decrease in the use of intravascular ultrasound (IVUS) from 5,748 procedures in 2010 to 3,641 in 2015, and the use of optical coherence tomography (OCT) with a clear increase from 507 cases in 2010 to 2,546 in 2015. Another marked increase has been experienced by flow or functional intracoronary techniques as is shown by the 130% increase from 2,383 procedures in 2010 to 5,503 in 2015.
Use of drug-eluting balloons (DEB) also showed a progressive increase, probably due to the growing evidence especially in the treatment of in-stent restenosis. This is probably what has led to higher numbers of PCI without stent(s) at the end of the period, despite these types of procedure still representing less than 5% of the total in Spain.
Other coronary techniques, such as rotational atherectomy, ventricular assist devices and intra-aortic balloon counterpulsation (IAoBCP), did not show noticeable changes during this period.
Structural heart interventions
Some techniques have struggled to grow and spread in our daily practice in Spain (Table 2). This area of interventional cardiology shows a plateau concerning numbers of alcohol ablations (around 60 per year), whereas other percutaneous treatment techniques such as TAVI have rocketed in the last six years. In the last year, 1,586 TAVI implantations were carried out, resulting in a ratio of 34 procedures per million inhabitants, still far less in comparison to leading European countries4. As an example, in 2015 most of the cases (73.2%) were performed in inoperable or very high surgical risk patients. In 2015 the access mainly used was femoral (85%), and procedural success without major complications during hospitalisation was reported in 74% of the cases (the need for a pacemaker during this period was 10.9%).
The volume of aortic valvuloplasty practically doubled, achieving similar values to mitral valvuloplasty in 2015, being 240-250 cases per year. Another valve disease which showed a progressive increase in its percutaneous approach was paravalvular leak. In fact, total numbers showed a 40% increase after six years in this technically demanding approach. An increase in the number of paravalvular mitral leaks treated is the main cause of its relative increase (Table 2).
In relation to techniques that use closure devices, in Spain there has been a constant use of atrial septal devices at around 300 cases per year and also patent foramen ovale devices at around 200 cases per year to treat congenital defects in adults. Of note, experience with other closure devices was different, as shown for left atrial appendage (LAA) closure which revealed a constant growth during this period and especially during the last two years. This last progression was in fact very similar to the one shown by the MitraClip (Abbott Vascular, Santa Clara, CA, USA ) procedure in our country that finally exceeded 150 cases per year in 2015.
Conclusion
ORGANISATION
Since 1990 the Spanish Working Group has worked to create an Annual Registry that is voluntarily completed by participants, representing most of the interventional cardiology activity in Spain. Thanks to these continuous data over 25 years, their analysis probably represents the evolution of interventional cardiology and its implementation in Spain. This last six-year period shows a clear increase in the number of cathlabs and also the number of physicians which has led to a lower ratio of cases per operator. This was probably due to the need for 24h/7d coverage as primary PCI programmes have developed and have stressed weekly staff planning to the utmost.
CORONARY PROCEDURES
From the numbers of different coronary procedures analysed throughout this period, one can assume that in 2010 in Spain technical development had already probably been achieved as complex procedures have not changed significantly. Conversely, the increase in coronary angiograms and primary PCI shows that there was still room for coronary interventions in the acute MI setting. This specific scenario has probably influenced some of the trends during these six years. For instance, a high ratio of DES took more time to be achieved than in other similar countries3, complex PCI did not show a special increase, and the stent per case ratio experienced a progressive decline2. Also, the increase in the use of the radial access can be clearly related to the group where more evidence has emerged, namely acute coronary syndrome (ACS).
Lower stent thrombosis rates, new stent platforms and the advent of bioresorbable scaffolds (BRS), though still in small numbers, have probably influenced the change from IVUS to OCT use as an adjunctive imaging technique. Also, evidence concerning functional lesion assessment has led to fractional flow reserve (FFR) being progressively adopted as the tool to decide or address treatment during PCI.
STRUCTURAL INTERVENTIONS
Despite some structural interventions starting more than 30 years ago, the emergence of structural percutaneous treatment has increased in recent years. This explains why some “old” but useful techniques such as alcohol ablation remain very stable in terms of the number of procedures per year, while the new ones such as TAVI follow a logarithmic progression. In between lie other procedures that have experienced a second youth such as aortic valvuloplasty. TAVI programmes have very probably led to the relative increase of this technique, almost abandoned in previous years. In Spain, probably as a consequence of economic restrictions suffered during this period, some of these advances have been delayed or decreased compared to other European countries. However, increasing evidence, clinical success and especially a decrease in the rate of complications have led to the progressive adoption of TAVI, closure of mitral paravalvular leaks and LAA closure5.
Limitations
As is usual in this kind of investigation, this survey has important limitations, which should be taken into account when interpreting the results. First of all, the registry, despite being completed by most of the high-volume centres, was not completed by all. Therefore, the results are partly representative of the whole collective. Also, we should not forget that there was no audit process to avoid bias and that the completion process was voluntary.
Acknowledgements
The authors would like to express their gratitude to all the physicians who voluntarily completed the National Registry during this period. Moreover, the authors would like to thank especially all the successive Working Groups on Interventional Cardiology for providing and publishing the registry.
Conflict of interest statement
The authors have no conflicts of interest to declare.
