![]()
Abstract
The Israel Heart Society is a member of the European Society of Cardiology, and the Israeli Working Group of Interventional Cardiology is an active participant in EAPCI. The aim of this manuscript is to provide a snapshot of cardiac interventions performed in the State of Israel during the period 2010-2015. Data for this manuscript were collected via collaboration with the National Diseases Registries Unit of the Israel Center for Disease Control.
During the survey period, the Israeli population increased by 7% but only one additional hospital with an active cardiac catheterisation laboratory was opened. The vast majority of the percutaneous procedures are performed in public hospital settings. Total coronary angiography procedures remained stable throughout the survey period, and the percentage of PCI out of total coronary angiography procedures remained approximately 50% throughout the survey period. More than 90% of the PCI procedures were performed using stent deployment, and the use of drug-eluting stents increased significantly during the survey period from 46% in 2010 to 92% in 2015. The number of TAVI procedures increased dramatically, by more than sixfold, from 130 procedures in 2010 to 851 procedures in 2015 (with 130 implants/million population at Q4 of 2015).
The vast majority of interventional cardiology procedures are funded by the governmental healthcare providers, and all the citizens of the country have access to the most advanced cardiac interventions. If corrected for the increase in the population, the volumes of coronary interventions are decreasing throughout the country. However, structural heart disease interventions, and specifically valvular interventions, are growing rapidly and this trend is expected to continue in the near future.
Demographics and organisation
The State of Israel has had a National Health Insurance Law since 1995 with universal entitlement to a basic package of healthcare. There are almost 8,500,000 citizens in the State of Israel, with a mean life expectancy of 81.6 years (84.1 for women, and 80.3 for men), but only 10.3% of them are 65 y/o or older. The gross national product of Israel is 297 billion US $, and the average monthly income of a household is about 3,100 US $. Core healthcare benefits in Israel are funded through general revenue taxation combined with an additional income-based tax collected for the sole purpose of funding healthcare. The pooled contributions with a supplemental governmental budget are distributed nationally to four competing sickness plans or funds that organise, manage, and procure healthcare for their members. The sickness plans must accept all applicants who want to join or switch from their current plan. Similarly, participating healthcare providers must accept all patients, in accordance with the plan’s provisions.
Hospital care is mostly provided by public hospitals. Very few privately owned hospitals, or non-governmental but not for profit hospitals operate in Israel. The sickness plans cover all hospitalisation costs and any required in-hospital or elective ambulatory procedures carried out at public or private hospitals. Citizens are able to extend the public basic health insurance by purchasing second and/or third tier complementary insurance. These insurance extensions cover certain new and expensive medications, the privilege to undergo surgeries and interventions at private hospitals, and the ability to choose the operator who will perform the procedure. Accordingly, the majority of cardiac interventions are performed at public hospitals.
Currently, there is no national registry for cardiac interventions in Israel. This registry is presently being built, with the cooperation of the Israeli Society of Cardiac Surgery. There is an active transcatheter aortic valve implantation (TAVI) multicentre registry that collects TAVI data from four major medical centres for academic purposes.
All procedures performed are reported to the Ministry of Health by ICD-9 codes for reimbursement purposes. Data for this manuscript were collected via multiple national sources of information: collaboration with the National Diseases Registries Unit of the Israel Center for Disease Control and directly from the interventional cardiology units around the country.
During the survey period, the Israeli population increased by 7%, from 7.69 to 8.29 million citizens, but the number of active cathlabs increased only from 32 in 2010 to 35 in 2015. The vast majority of percutaneous procedures are performed in public hospital settings and, accordingly, most of the cardiac catheterisation laboratories are operated in public hospitals (32 of 35 cathlabs). Despite the fact that travel distances in Israel are small, due to the recognition of the importance of timely reperfusion for ST-elevation myocardial infarction, most hospitals run 24/7 primary PCI programmes (22 of 24 hospitals) and, accordingly, rates of thrombolytic therapy for ST-elevation acute myocardial infarction in recent years have dropped to nearly zero.
Interestingly, only half of the medical centres which operate a cardiac catheterisation laboratory have an on-site cardiac surgery service (13 of 24 hospitals). This has implications for structural procedures and especially valve interventions which will be discussed below. In Israel, hospitals without an on-site cardiac surgery service are allowed to perform all coronary interventions at the discretion of the performing physician.
Coronary interventions
Total coronary angiography procedures remained stable throughout the survey period (Table 1), and the percentage of PCI out of total coronary angiography procedures remained approximately 50% throughout the survey period. However, when corrected for the population growth (7% during the survey period), there was a small constant decrease in total coronary angiography and PCI rates during 2010-2015. More than 90% of the PCI procedures were performed using a stent, and the use of drug-eluting stents (DES) has increased significantly during the survey period from 46% in 2010 to 92% in 2015 (Table 1).
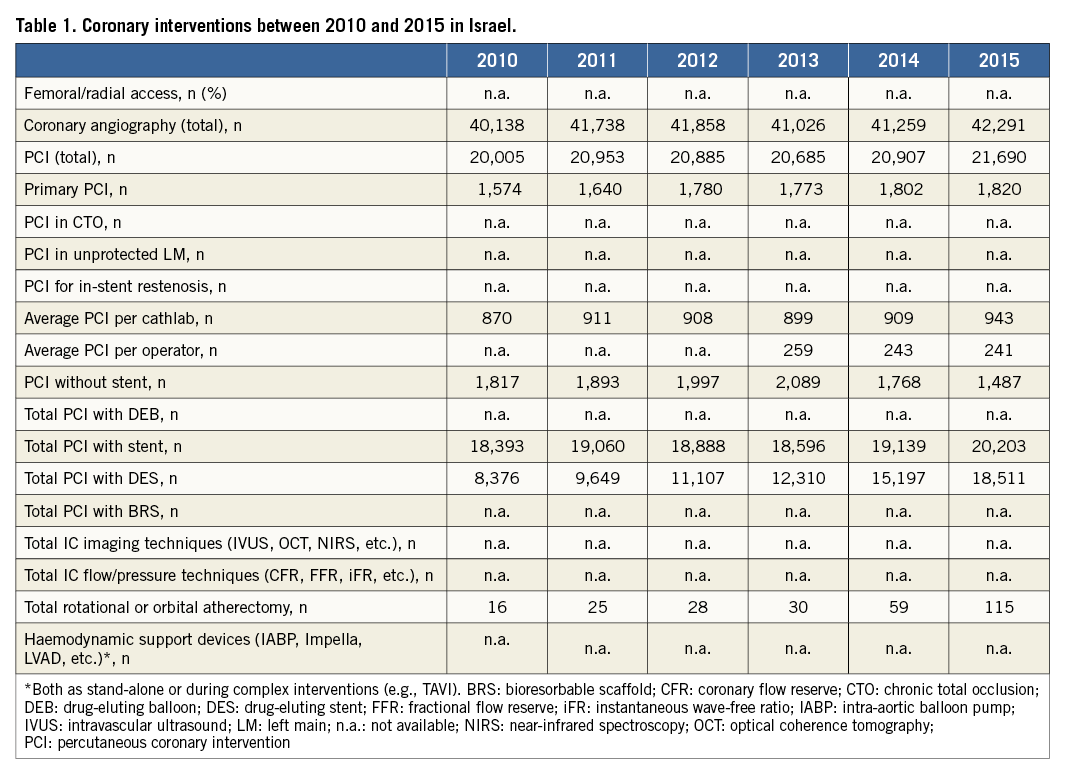
These findings indicate that between 2010 and 2015, if corrected for the increase in the population, the volumes of coronary interventions decreased throughout the country. However, the ratio remained relatively stable, with half of the diagnostic angiographies continuing to percutaneous coronary intervention (PCI). Of these PCI procedures, over 90% utilised a stent. This trend was the result of ample literature supporting the use of new-generation DES in all PCI indications including, among others, ST-elevation myocardial infarction and saphenous vein grafts1-3. This coincides with similar trends in other countries4-6. The fact that DES were utilised in no more than 72.3% of PCI in 2014 warrants further exploration since most recent reports indicate a higher rate of usage.
Since the introduction of PCI in the late 1970s, a constant increase in the number of coronary angiographies and coronary interventions has been recorded. This trend was scrutinised by professional societies due to reported inappropriateness in about one out of six patients7,8. Thus, “appropriate use criteria” (AUC) for PCI were published as consensus documents by most of the relevant US professional societies9. The implementation of these AUC was translated into a decrease in the number of PCI performed in the USA in recent years7,10. As opposed to US data, emerging data from Europe have demonstrated a constant increase in PCI volume4,7,11. In the OECD report, most of the significant increase in PCI rates was attributed to the increasing availability of coronary revascularisation services in developing countries, while a smaller increase in PCI rates was recorded in countries with an established coronary revascularisation programme. Thus, due to the fact that Israel has a longstanding coronary revascularisation programme, no significant increase in the number of procedures performed was expected. Further, Israel in general adopts the recommendations of both European and US professional societies. This adoption of both guidelines, which may conflict in their recommendations, might explain the constant number of procedures reported in this data set. The fact that the number of coronary interventions in Israel remained fairly constant should be further explored. Adjustment for age and indication for procedures (stable angina versus acute coronary syndrome) might shed some light regarding various trends in revascularisation in the relevant subpopulation.
Structural heart interventions
Transcatheter aortic valve implantation (TAVI) procedures in Israel are currently performed only in hospitals with on-site cardiac surgery services, but the vast majority of TAVI procedures are performed in the cardiac catheterisation laboratories by interventional cardiologists. Cardiac surgeons participate in procedures performed by alternative access (i.e., transapical, transaxillary or direct aortic), usually in hybrid rooms. The number of TAVI procedures increased dramatically, by more than sixfold, from 130 procedures in 2010 to 851 procedures in 2015. The vast majority of TAVI procedures are performed via the transfemoral approach (Table 2). In Israel most of the procedures are performed with conscious sedation and complete percutaneous transfemoral access without surgical cut-down.
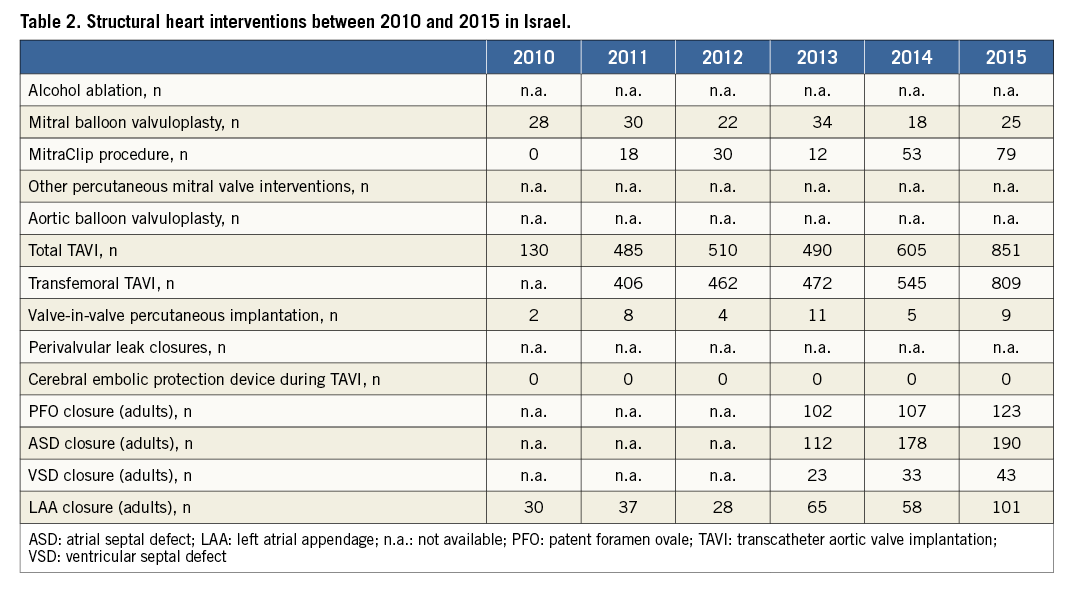
The performance of MitraClip® (Abbott Vascular, Santa Clara, CA, USA) procedures in Israel started at the beginning of 2011, and remained small in numbers until the end of 2013, when the procedure gained reimbursement by the healthcare system in the country. Since then, the procedure has been growing, and more and more operators participate in these procedures.
Other structural heart disease percutaneous interventions have increased throughout the survey period. The most rapidly growing intervention is left atrial appendage occlusion (LAAO). LAAO was performed in 30 patients in 2010, but with accumulating data the procedure is now being performed more frequently, reaching 100 procedures in 2015 (Table 2). This procedure is usually performed in collaboration with the electrophysiology specialists, but the extent of this collaboration varies with different hospitals. With the improved safety of LAAO, this procedure is now also being performed in hospitals without on-site cardiac surgery services.
There is no doubt that by far the most dramatic change in the interventional procedures in Israel during this period, similar to what happened during the same period in Europe as well as in the USA, concerns the interventional treatments for structural heart disease, of which TAVI represents the greatest change. It was started in the four largest interventional centres in Israel in September 2008, and was growing slowly until the beginning of 2010, when the TAVI procedure gained reimbursement by the Israel healthcare system. Since then, due to operators’ growing experience, device improvement, and the indication creep towards patients in intermediate operative risk for aortic valve replacement, the volume of these procedures has undergone an exponential increase, from 130 in 2010 to more than 850 in 2015 (Table 2). The increase in MitraClip procedures in Israel was very slight until the end of 2013, when the procedure started its reimbursement era. There is no doubt that the penetration of these structural heart disease interventions is promising, as a result of the growing numbers of interventional cardiologists in Israel, as in the rest of the world, who are capable of performing the procedures, the growing number of centres adopting the procedures (including those with no cardiac surgery on-site), and, mainly, the robust support in the literature of the true clinical benefit for selected patients of these procedures.
Conflict of interest statement
The authors have no conflicts of interest to declare.
