![]()
Abstract
Interventional cardiology procedures are constantly increasing in numbers and in quality, especially in developing countries such as Egypt. The numbers and types of procedure now available have driven development in the field and in its accompanying services. The aim of this short report is to present a review of the development of interventional cardiology in Egypt during the period 2010-2015 and the demographic, economic and educational factors that have affected this process. We collected and analysed data provided by different centres and from the distributors of intervention tools for the years 2010 to 2015. Analysis of these data showed a steady growth of primary PCI, amounting to a threefold increase over the six-year period. There are increasing numbers of PCI-capable centres, especially in Cairo. Almost 55,000 PCIs are performed yearly in Egypt utilising around 100,000 stents; the percentage of drug-eluting stents (DES) used has increased to 65-70% (90% in private and insured patients). Structural intervention is growing fast for congenital heart disease, and balloon mitral valvuloplasty has become the default strategy. The numbers of TAVI and EVAR are also increasing, although cost remains the greatest challenge. These changes can be attributed to the increasing numbers of ischaemic heart disease patients over the last 25 years, involving improved education and awareness, patients presenting at a younger age, and improved practice in intervention. In Egypt, there has been a steady growth in PCI and intervention tools which has been faster in coronary and congenital heart disease than in structural heart disease during the period from 2010 to 2015.
Introduction
Heart disease is a leading cause of hospitalisation and death all over the world. Coronary angioplasty is a procedure that has revolutionised the treatment of ischaemic heart disease. More comprehensive management of cardiovascular health problems could bring substantial improvements to long-term clinical outcomes. Access to healthcare, prompt and accurate diagnosis, and the selection of appropriate therapy are all key determinants of outcome in patients with coronary disease.
Demographics and social factors
Egypt is one of the oldest countries in the world and has demonstrated a very rich history among ancient civilisations for its humanity. The remaining old Egyptian precious monuments reveal a unique administrative system which progressed across decades, where health was an integral part.
Presently, Egypt is considered a lower middle-income country as defined by the World Bank. About 43.5% of the population live in urban areas. The population pyramid of Egypt is typical for developing countries, with a vast proportion of the population below the age of 40 years.
In 2014, the total expenditure on health was 5.6% of the general domestic product1. Inequalities in the provision of health services present a great problem due to geographic and demographic diversities and the socioeconomic distribution of the population across the country. This is reflected in discrepancies in epidemiologic data about the different health problems, especially cardiovascular diseases2.
The majority of citizens are free to select the site and level of healthcare they prefer, according to available resources. A great part of the population is covered by health insurance including those of school age. Governmental hospitals, public health centres and university hospitals (18 faculties of medicine across the country) are the major sources of healthcare services with reduced fees. The private sector covers 10-15% of services, a considerable part of healthcare regarding procedures such as cardiac interventions.
In many instances, the government pays for those who cannot afford to cover the expenses of medical care through a special system of social welfare support2.
Coronary interventions
Some peculiarities of coronary artery disease patterns stand out in Egyptian patients. These include a younger age at presentation, a high incidence of two- and three-vessel disease, diffuse involvement, distal disease and a significant left ventricular dysfunction at presentation3-5.
Until now, no unified nationwide registry has been established to demonstrate the accurate figures of cardiac procedures; however, the COMBATMI conducted by the National Heart Institute in collaboration with cardiology departments in Ain Shams and Cairo universities undertook a registry for ACS patients in three phases – 2007, 2010 and 2013. It revealed that, as in many developing countries, the age of the patients was much younger and the prevalence of risk factors such as smoking, hypertension, and dyslipidaemia was high, in addition to delay in patients’ approach to cardiac centres in ACS. Analysis of registered data showed increasing use of invasive procedures by PCI over the years as shown in Figure 1. In addition, focusing on temporal changes in STEMI management, primary PCIs showed a threefold increase over the six-year period (Figure 2)6.
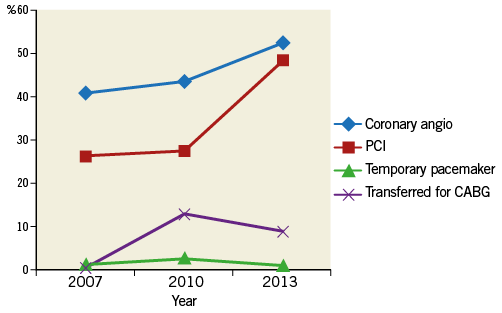
Figure 1. Temporal changes in the use of in-hospital invasive procedures in ACS patients.
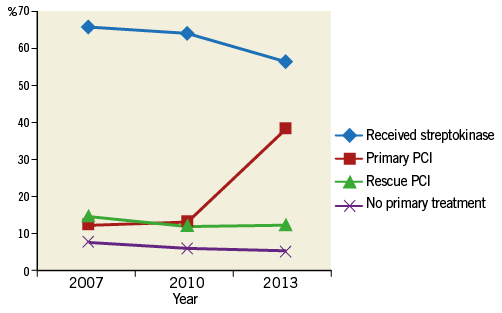
Figure 2. The increasing use of primary PCIs in STEMI management.
Cardiologists receive special training through internship and they should register for a postgraduate programme leading to a diploma or master’s degree at a university. Consultant cardiologists should have a doctor’s degree or an equivalent national or international fellowship.
Secondary prevention of cardiovascular disease is carried out by specialists. The Egyptian Society of Cardiology, which is collaborating effectively with both the European Society of Cardiology and the American College of Cardiology, has a great impact on updating and promoting the standard scientific practice of clinical and preventive cardiology among physicians.
There are increasing numbers of PCI-capable centres, especially in Cairo, Alexandria and other big cities across Upper and Lower Egypt.
The improved medical and interventional management of ACS patients was initiated by several tertiary centres such as university hospitals, and by the National Heart Institute.
The all-year round conferences, including the COMBATMI conference dedicated to ACS and ischaemic heart disease, initiated in 2007, the continuous medical education, and the advent of the Egyptian Fellowship of Interventional Cardiology that started in 2013, have all led to the improvement and better management of cases of ACS and those presenting for elective PCI. In the tertiary centres, the percentage of angioplasties for ACS as part of the total number has markedly increased, reaching nearly 50% in certain centres.
Egypt is also an active participant in the “Stent for Life” project, and this has greatly increased the frequency of primary PCI. The implementation of the “Stent for Life” proposal has led to a paradigm shift in the management of acute ST-segment elevation myocardial infarction. With five pilot centres (and now expanding), it has helped to implement an improved system of transport and communication between hospitals, and a quick transfer of the patient to the cathlab7.
This progress has resulted in the number of coronary care units and catheter units increasing to one cathlab per 950,000 population.
The classic femoral artery approach is still the most commonly used, mainly due to the classic training and due to the more expensive radial artery sheaths. The radial approach is now steadily becoming popular in Egypt, especially in the private sector where expenses are not a huge worry. However, this is also being seen in some university hospitals and the National Heart Institute, which will help the rapid turnover of patients in these high-volume centres.
The approval of health insurance to provide drug-eluting stents (DES) has been a game changer. Over the past one and a half years, the usage of bare metal stents for insured patients of the Ministry of Health has dropped dramatically. The introduction of DES for those who qualify, e.g., diabetics, post coronary bypass, long lesions, and in-stent restenosis, has provided an alternative means of management, other than coronary artery bypass, or even medical treatment in certain cases.
No cost-effectiveness studies have been conducted as yet, but long-term follow-up will show the cost-effectiveness of this approach to a wide spectrum of patients.
The Ministry of Health also recently approved, on a smaller scale, the usage of DES for those not insured. Due to the huge population and the prevalence of a high proportion of uninsured patients, the outcome of this initiative will take some time to impact on the health of a large proportion of the population.
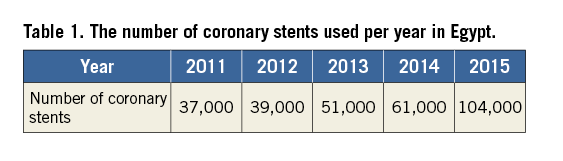
The total number of stents used has risen overall, but what is striking is the usage of DES. As compared to 2010 when DES constituted 35 percent of total stent usage in private and 10% in public hospitals, the numbers in 2015 are a phenomenal 70 percent (70,000 DES and 34,000 BMS) (Table 1). These data were obtained from the industry, as in Egypt we do not have a nationwide system for the calculation of the equipment used.
The private sector constitutes approximately 45% of the angioplasties performed in Egypt, and it accounts for more than 60% of the DES used.
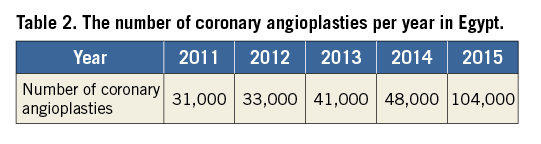
The estimated number of angioplasties performed in Egypt in 2015 is just over 55,000. This is more than twice the figure in 2013, when the number of angioplasties was approximately 20,000. There is a projected increase of 20-25% with the active participation of the Ministry of Health offering an improved medical and interventional service to the population (Table 2).
This has been accompanied by a decrease in the cost of the intervention, mainly due to the increase in the number of procedures being reflected in the cost of the equipment.
Structural heart interventions
Egypt was one of the leading countries in percutaneous mitral commissurotomy (PMC), thousands of procedures having been performed since 1992. The number of mitral valvuloplasties has decreased over the past decade. This was mainly due to improvement in patient education and rapid control of throat infections.
Transcatheter aortic valve implantation (TAVI) started in Egypt in 2013. The number has slowly increased in a few centres to a total number of 150 procedures carried out all over the country. The number is relatively low due to high cost, the greater prevalence of rheumatic rather than degenerative calcific aortic valve disease, and the still growing experience of this procedure. However, as this procedure is making gains in terms of preference and the operators are gaining more experience, more and more cases are being conducted, and this led to the first valve conference in 2016.
Other structural interventions such as ASD, VSD, PDA closure, and for vascular malformation have developed and are routinely carried out by paediatric interventional cardiologists.
Conclusion
Coronary artery disease has reached epidemic proportions in the Middle East, especially in Egypt, in recent years. Unhealthy dietary habits, sedentary lifestyle, atherogenic dyslipidaemia and a high incidence of smoking and diabetes have largely been responsible.
At the same time, however, better medical facilities have been introduced and coronary interventions are being performed all over the country. Growing expertise coupled with greater awareness and better affordability amongst patients will have a positive impact in the future. The Egyptian Society of Cardiology is also engaging in several educational ongoing and future projects for the education and implementation of best medical practice in all patients including PCI patients.
Conflict of interest statement
The authors have no conflicts of interest to declare.
