![]()
Abstract
For the last five years, invasive cardiology in Poland has developed extensively. Currently, 98% of the 161 Polish cathlabs operate in 24/7 mode, 37 of them supported by cardiac surgery departments on-site. A certification curriculum for interventional cardiology operators is supported by dedicated workshops and scientific meetings during national conferences. The rise in the number of coronary angiographies and PCIs was paralleled by an increased use of drug-eluting stents, bioresorbable vascular scaffolds and physiologic assessment of coronary arteries. Radial artery access has become the default option for PCI. A rapid adoption of the EAPCI Stent for Life Initiative resulted in a significant increase in primary PCIs. Unlike coronary interventions, structural heart interventions have evolved unevenly, despite the solid network of Heart Teams set up in the 21 most experienced centres. Left atrial appendage closure is offered in an increasing number of cathlabs. MitraClip therapy remains largely underused (1 procedure/million population/year). Despite the slow growth of TAVI since 2008, the current annual number of 17.1 TAVI procedures per million population is incomparable with countries in Western Europe. A recently introduced EAPCI Valve for Life campaign was followed by a 42.6% annual increase in TAVI procedures and an improvement in patients’ access to therapy in life-saving indications.
Demographics and organisation
Poland is the 6th most populated country in the European Union with 38,437,239 inhabitants. There are currently 161 invasive cardiology centres in service, equally distributed throughout the country. Ninety-eight percent of them operate on a 24/7 basis, 37 with the cardiac surgery back-up present on-site. The number of cardiac catheterisation labs per 1 million population is well in line with the recommendations of the European Society of Cardiology1. In 2013 the Association of Cardiovascular Interventions of the Polish Cardiac Society (ACVI) introduced a certification programme for interventional cardiologists, recognising 630 percutaneous coronary intervention (PCI) operators and 129 coronary angiography specialists by 2016. The vast majority are board-certified cardiology specialists. The certification curriculum includes annual participation in at least two accredited scientific meetings: The New Frontiers in Interventional Cardiology Workshop in Krakow (NFIC, www.nfic.pl) and the Warsaw Course on Cardiovascular Interventions (WCCI, www.wcci.pl), hosting distinguished speakers in interventional cardiology and attracting participants from Europe, the USA, Asia and the Middle East.
Interventional cardiology procedures are documented in two national registries: 1) a web-based ORPKI Registry, operated by the Jagiellonian University Medical College in Krakow and the ACVI, collecting data on elective and acute percutaneous coronary and non-coronary procedures, and 2) the PL-ACS Registry administered by the Silesian Center for Heart Diseases in Zabrze, which focuses strictly on acute coronary syndromes treated both conservatively and invasively. All coronary angiography and PCI procedures should be reported in the ORPKI Registry. Procedural details such as lesion location, type of stent or use of additional devices, pharmacotherapy as well as time delays in ACS patients are noted.
An obligatory national health insurance covers interventional cardiology treatment in Poland without patient co-payment. The Polish National Health Fund reimburses procedural and hospitalisation costs to public and private hospitals based on the system of diagnosis-related groups (DRG). The reimbursement scheme for the treatment of acute coronary syndromes is unlimited, while compensation for elective cardiology procedures is contract-dependent and varies between centres. The latter scheme also applies to coronary imaging and physiologic assessment modalities (IVUS, FFR) and structural procedures. Notably, the allowed number of transcatheter aortic valve implantations and percutaneous mitral valve repairs (MitraClip®; Abbott Vascular, Santa Clara, CA, USA) is regulated yearly by the Ministry of Health.
Website of the Association of Cardiovascular Interventions of the Polish Cardiac Society: http://www.aisn.pl/
Coronary interventions
The number of coronary angiographies and percutaneous coronary interventions (PCI) has been rising since 2010 (Table 1). Following the rapid adoption of the European Association of Percutaneous Coronary Interventions (EAPCI) Stent for Life Initiative in Poland since 2008, the number of patients with ST-segment elevation myocardial infarction (STEMI) treated with primary PCI rose steeply, positioning Poland among leaders in EU countries2. Similar trends have been observed for the treatment of NSTE acute coronary syndromes (Figure 1). In accordance with current guidelines and recommendations, the majority of PCI procedures are now performed through the radial artery, a notable change from femoral access practices in 2010. In a similar pattern, widespread implementation of drug-eluting stents (currently >90% of PCIs), bioresorbable vascular scaffolds (almost 2,000 patients treated in 2015) and physiologic coronary flow assessment (FFR) has occurred since 2010. The use of drug-eluting balloons, intravascular imaging (IVUS, OCT) and rotational atherectomy remains too low. The issue is being addressed by ACVI with the organisation of dedicated workshops and educative meetings. In 2015, the number of coronary angiographies and PCI procedures per 1 million inhabitants in Poland was 5,756 and 3,244, respectively.
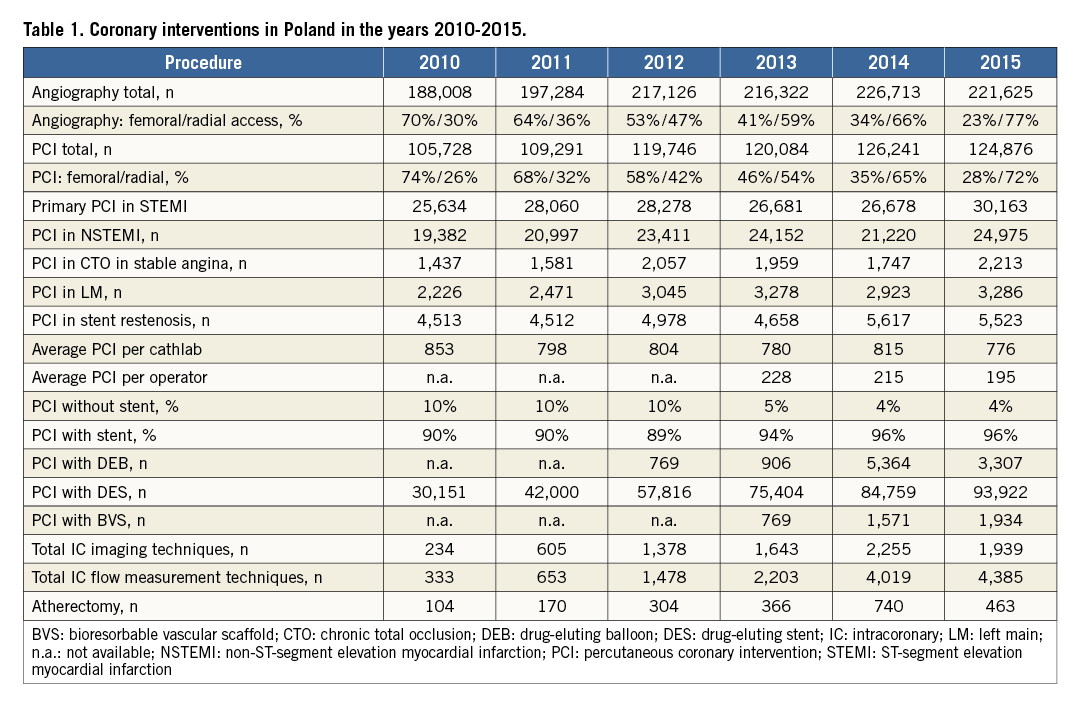
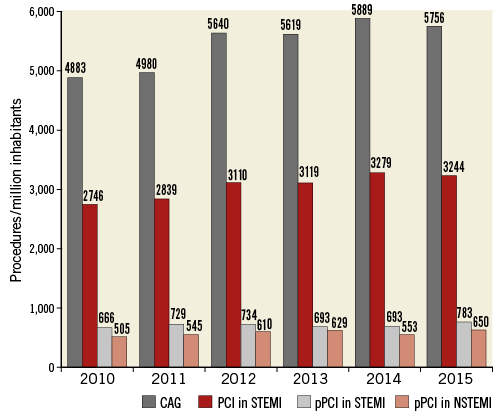
Figure 1. Coronary interventions per 1 million inhabitants in Poland in the years 2010-2015. CAG: coronary angiography; PCI: percutaneous coronary intervention; pPCI: primary percutaneous coronary intervention
Structural heart interventions
The organisation of Polish centres built around transcatheter valve therapy adheres to current guidelines and recommendations, with Heart Teams, interventional cardiology and cardiac surgery departments established in all of them3. The number of patients treated with the MitraClip Percutaneous Mitral Valve Repair System (Abbott Vascular) has been unsatisfactory, with a minimal increase in the past five years (Table 2). Despite a positive growth of transcatheter aortic valve implantation (TAVI) from 2010 to 2015, the latest annual number of 17.1 TAVI procedures per million population in Poland is ten times lower than in Germany and half of the Western European average reported in 20114. Possible causes of such disparity include low health spend, high cost of the procedure relative to the GDP per capita, taxation system and the strategy of restrictive reimbursement of the Polish National Health Fund with a limited annual number of TAVI procedures. The reimbursement is directed to cardiac surgery departments only, although implantations involve both invasive cardiologists and cardiac surgeons. The recent study of 21 Polish TAVI centres reported patient referral and waiting lists far exceeding the allowed treatment quotas in 20155. Based on reports of TAVI development in Poland, the EAPCI introduced the Valve for Life Initiative in Poland in 2015 “to enhance awareness concerning inequality of patient access to the life-saving indications of TAVI therapy […] with the goal of increasing the treatment of severe valvular heart disease by 20% by 2020”6. As a result of a vigorous, nationwide Valve for Life campaign, the number of patients treated with TAVI increased by 42.6% in 2015 in comparison to 2014 (Figure 2)5.

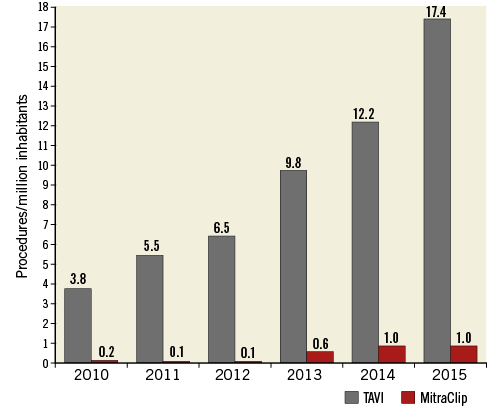
Figure 2. TAVI and MitraClip implantations per 1 million population in Poland, in the years 2010-2015.
The rates of percutaneous closure of atrial septal defects, patent foramen ovale and ventricular septal defects have remained stable during the past five years. The number of patients treated with the closure of paravalvular leaks is steadily increasing, with three invasive cardiology centres involved. The experience with left atrial appendage closure is growing exponentially, although the total number of procedures remains low.
Conclusion
The strong set-up of 161 invasive cardiology centres, certification curriculum, ACVI-mediated education and rapid adoption of EAPCI Stent for Life Initiative have allowed the steady increase and improvement of percutaneous coronary interventions. However, despite a solid network of Heart Teams across Poland, structural heart interventions have developed unevenly. The observed impact of the EAPCI Valve for Life campaign on TAVI rates in Poland points to the need for further co-ordinated action to facilitate patient access to life-saving therapies.
Acknowledgements
The authors would like to thank Ms Agnieszka Lenik, ACVI, for her valuable help in data mining and presentation.
Conflict of interest statement
The authors have no conflicts of interest to declare.
