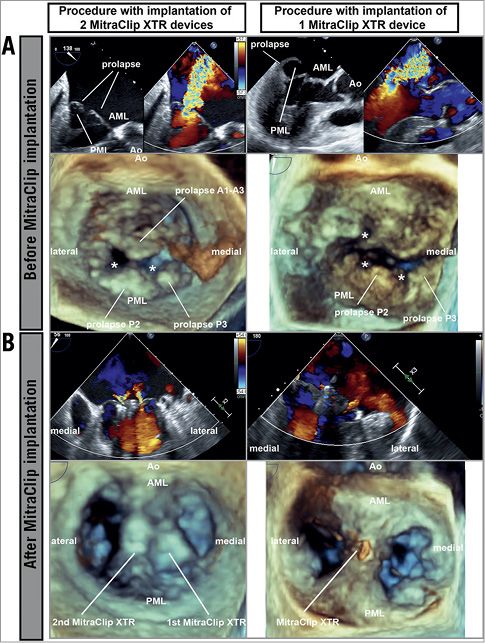
Figure 1. Transoesophageal echocardiography before and after MitraClip implantation. A) Before MitraClip implantation. B) After MitraClip implantation. * Structural defect. AML: anterior mitral leaflet; Ao: aortic valve; PML: posterior mitral leaflet
Various surgical strategies exist for Barlow’s disease (extensive mitral valve prolapse >1 segment, leaflet thickening)1. However, interventional therapy using the MitraClip® (Abbott Vascular, Santa Clara, CA, USA) in high-risk surgical candidates with Barlow’s disease is complex: either highly mobile leaflets lead to relevant residual mitral regurgitation (MR) or extensive grasping of redundant leaflet tissue might result in mitral stenosis2. In 2018 the MitraClip NTR and XTR (both Abbott Vascular) were launched, featuring technical modifications of the delivery catheter (shaft extension increased by 1.5 cm, more direct, predictable trajectory during positioning) and lock mechanism. In the MitraClip XTR, arm length has been increased from 9 mm to 12 mm and coaptation length and grasping is facilitated by two additional rows of frictional elements at the grippers. So far, the MitraClip XTR has been employed predominantly in functional MR and severely impaired left ventricular function3.
We used the MitraClip XTR in four patients with Barlow’s disease because of its increased coaptation length facilitating grasping of redundant tissue of prolapsing segments. All patients had severe MR (effective regurgitant orifice area of 0.6-2.2 cm2) with prolapse of >1 segment (6-13 mm above the annulus) (Figure 1A). The left atria were enlarged concomitant with severe MR, easing device positioning. Mitral annulus dilatation was not a prerequisite for the MitraClip XTR. By deployment of the MitraClip XTR at the main prolapse site, leaflet mobility was stabilised. Significant reduction to mild MR was achieved in one patient. In the other patients, a second MitraClip (NTR or XTR, depending on the length of the remaining leaflets) was placed at the centre of the remaining regurgitation to stabilise the leaflets further; this achieved sufficient MR reduction. No relevant transmitral gradients (mean pressure gradient 2-6 mmHg) occurred, even after implantation of a second MitraClip (Figure 1B).
Interventional treatment of Barlow’s disease is challenging due to the high mobility of the mitral leaflets; however, the latest MitraClip XTR renders the beneficial use of MitraClip devices possible.
Conflict of interest statement
The authors have no conflicts of interest to declare.