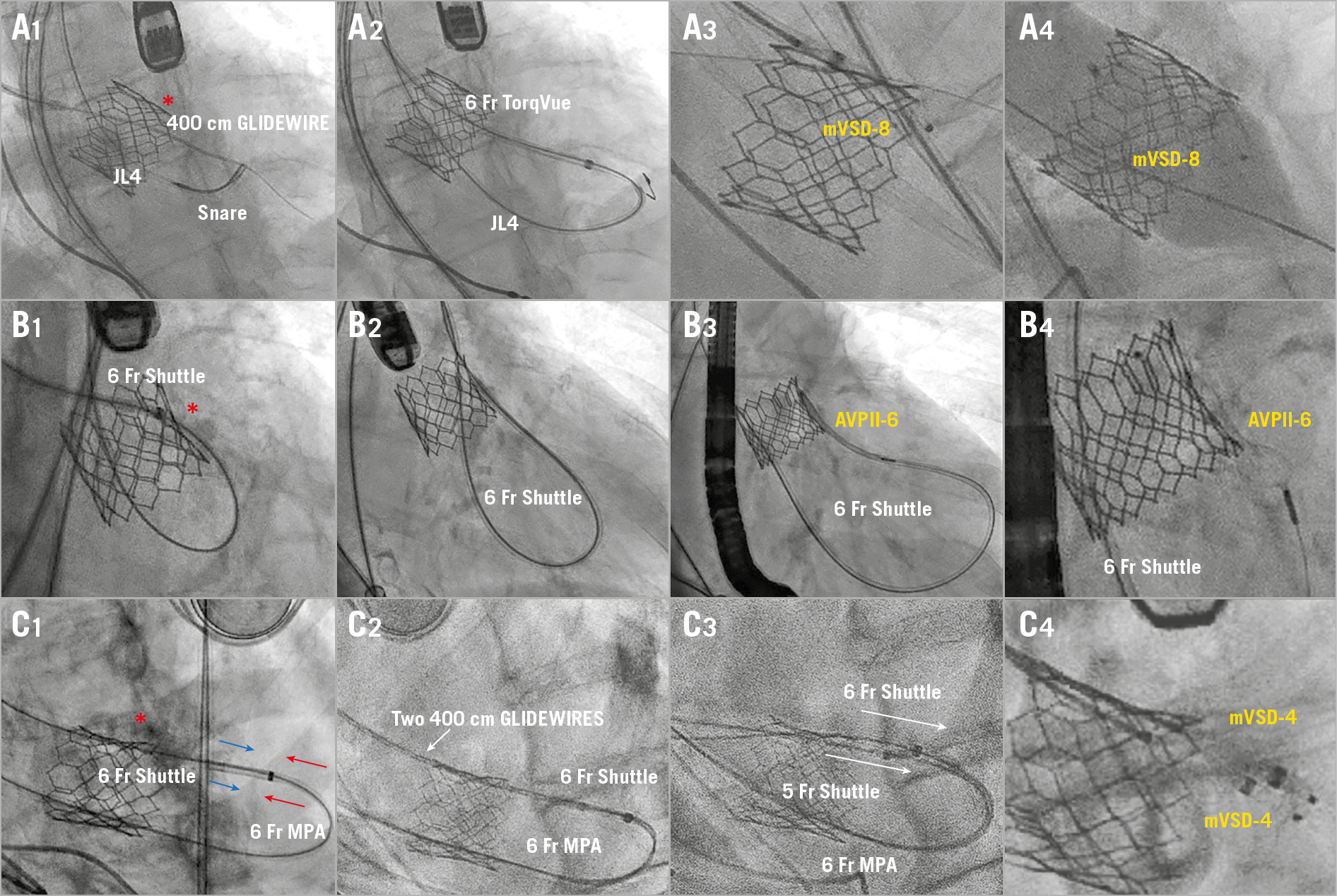
Figure 1. Fluoroscopic images illustrating three “retro-antegrade” cases of post-TAVR PVL closure (*=calcium).
Paravalvular leak (PVL) post transcatheter aortic valve replacement (TAVR) is challenging to close due to the presence of the transcatheter valve frame and calcium along the leak. We adopted the “retro-antegrade” approach to facilitate catheter and device delivery in closing three SAPIEN 3 (Edwards Lifesciences, Irvine, CA, USA) PVLs 3 months, 5 months and 1 month post TAVR, respectively, due to bulky left ventricular outflow tract (LVOT) calcium. Single arterial access for a 14 Fr DrySeal sheath (W. L. Gore & Associates, Inc., Flagstaff, AZ, USA) was used in all patients.
In patient A, the PVL was crossed retrogradely with a 400 cm 0.035” stiff-angled GLIDEWIRE® (Terumo Corp., Tokyo, Japan) within a 6 Fr Launcher® EBU 3.75 guide catheter (Medtronic, Minneapolis, MN, USA). Due to difficulty in catheter delivery, an arterial-arterial (A-A) rail was created by snaring the GLIDEWIRE in the LVOT into a JL4 guide catheter through the centre of the valve and externalised (Figure 1A1). A 6 Fr AMPLATZER™ TorqVue™ sheath (Abbott Vascular, Santa Clara, CA, USA) crossed the leak with the A-A rail support, and an 8 mm Amplatzer™ muscular VSD occluder (mVSD-8; Abbott Vascular) was deployed, improving the PVL to moderate (Figure 1A2, Figure 1A3). Finally, the valve was post-dilated with a 26 mm TRUE® balloon (Bard Peripheral Vascular, Tempe, AZ, USA), eliminating the residual PVL by conforming the occluder device to the leak (Figure 1A4, Moving image 1, Moving image 2).
In patient B, multiple catheters failed to cross retrogradely despite A-A rail support as above (Figure 1B1); therefore, a 5 Fr Shuttle sheath (Cook Medical, Bloomington, IN, USA) was advanced over the externalised wire retrogradely through the valve centrally and antegradely through the leak (Figure 1B2). A 6 mm AMPLAZTER™ Vascular Plug II (AVPII-6; Abbott Vascular) was deployed, reducing the PVL to trivial (Figure 1B2, Figure 1B3, Figure 1B4, Moving image 3, Moving image 4).
In patient C, two devices were planned due to crescent-shaped PVL. After A-A rail formation as above, a 6 Fr Shuttle sheath was advanced across the defect and a 6 Fr MPA guide catheter was advanced centrally through the valve and telescoped into the sheath (Figure 1C1). Then, another 400 cm 0.035” GLIDEWIRE was sent through the catheters to establish two A-A rails (Figure 1C2). Afterwards, a 6 Fr and a 5 Fr shuttle sheath were delivered retrogradely through the PVL with rail support, to facilitate subsequent simultaneous implantation of two 4 mm Amplatzer muscular VSD occluders (mVSD-4), reducing PVL to mild (Figure 1C3, Figure 1C4, Moving image 5, Moving image 6).
The illustrated “retro-antegrade” approach can facilitate catheter delivery across post-TAVR PVL and hence expand occluder device choices and optimise occlusion results. Balanced push-and-pull force is needed while manipulating the A-A rail to avoid the risk of valve embolisation.
Conflict of interest statement
M.H. Eng is a proctor for Edwards Lifesciences. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Baseline and post PVL closure.
Moving image 2. Transoesophageal echocardiograms for each of the three patients.
Moving image 3. Baseline and post PVL closure.
Moving image 4. Transoesophageal echocardiograms for each of the three patients.
Moving image 5. Baseline and post PVL closure.
Moving image 6. Transoesophageal echocardiograms for each of the three patients.