A 34-month-old boy (16.4 kg) presented with a myocardial bridge in the whole region of the left anterior descending (LAD) artery which was detected after repeated cardiac decompensation. Angiography demonstrated an imposing constriction of the left anterior descending artery in systole (Figure 1A, Figure 1B). Echocardiography confirmed dyskinesia of the moderately dilated left ventricle apical and basolateral, as well as mild mitral valve regurgitation (Figure 1C). Ejection fraction was 24%. The patient developed fever on the admission day and was operated on urgently due to new cardiac decompensation with elevation of cardiac enzymes. The LAD was covered with 14 mm thick muscle and a radical 6 cm-long myotomy of the ventral and lateral part of the LAD was performed (Figure 1D). Blood cardioplegia was applied intermittently to control bleeding points and the course of the LAD. The distal 3 cm of the LAD took its course intracavitary in the right ventricle. Postoperative echocardiography showed an excellent result with diminished mitral valve insufficiency and improvement of the left ventricle function.
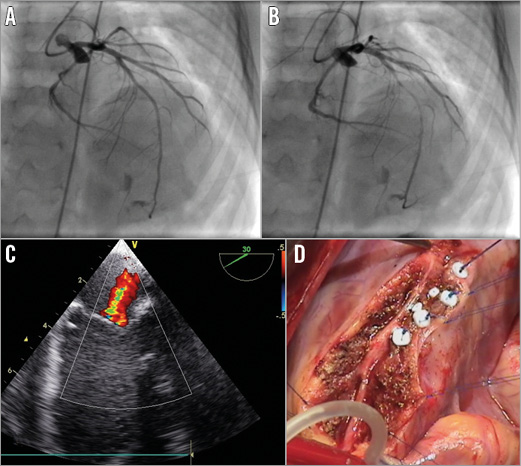
Figure 1. Preoperative and intraoperative images. Angiography of the left coronary system in the diastolic (A) and systolic (B) phase in LAO. The left anterior descending artery is squeezed in the middle part for approximately 5 cm, with reduced flow as the ventricle contracts. Preoperative echocardiography demonstrating mild mitral valve regurgitation (C). Intraoperative picture after excision of the myocardial bridge and closure of the right ventricle cavity with pledgets (D).
A myocardial bridge compromising the coronary artery and producing ischaemia and symptoms in children is an uncommon but critical situation. Our case describes a pronounced case of a myocardial bridge which was successfully treated with a radical myotomy and extrication of the LAD.
Conflict of interest statement
The authors have no conflicts of interest to declare.
