Primary mural aortic thrombus in a non-aneurysmal aorta is a rare entity and an uncommon cause of peripheral arterial embolisation1. This case report describes a minimally invasive, catheter-based treatment of a large symptomatic aortic thrombus located in the aortic arch using a transcatheter thrombus aspiration system followed by implantation of an endovascular thoracic stent graft in a patient not suitable for conventional surgery.
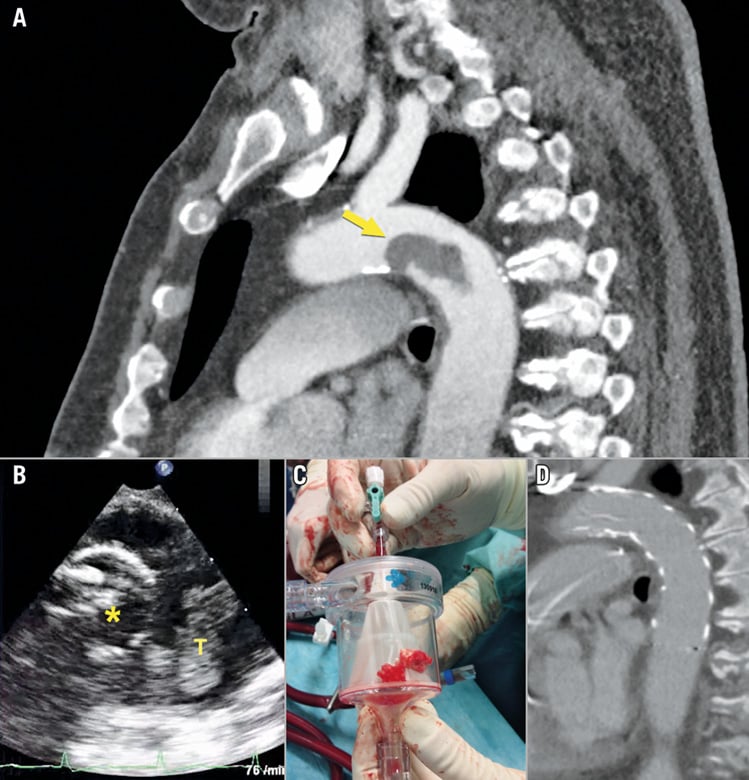
A 70-year-old obese male patient with past medical history of smoking, chronic obstructive pulmonary disease, hypertensive heart disease and insulin-dependent diabetes was transferred to our hospital with abdominal pain, dyspnoea and systemic inflammatory response syndrome (SIRS). A subsequent computed tomographic angiography (CTA) of the aorta and a transoesophageal echocardiography (TEE) revealed a large floating pedunculated thrombus based on the inner curve of the aortic arch, most likely due to an underlying penetrating atherosclerotic ulcer (PAU) (Panel A, Moving image 1). There was also evidence of multiple peripheral embolisation (spleen, celiac trunk, kidney). Conventional open thrombectomy or implantation of an intravascular stent graft was considered too dangerous due to the thrombus location and the existing comorbidities.
Since all conventional treatment options in this case were deemed unsuitable we decided to apply a thrombus aspiration strategy utilising the AngioVac catheter system (AngioDynamics, Latham, NY, USA) as an off-label use.
Right common femoral artery (CFA) and left common femoral vein (CFV) were exposed after surgical cut-down. The AngioVac system was connected to an extracorporeal bypass circuit (iLA activve®; Novalung, Heilbronn, Germany) operated by an adjustable centrifugal non-occlusive pump and the AngioVac cannula (22 Fr angled tip [20°]; 26 Fr introducer sheath) serving as the inflow and the cannula in the CFV (22 Fr) as the outflow.
Under angiographic and TEE guidance the AngioVac cannula was advanced distal to the thrombus (Panel B; AngioVac catheter [*], thrombus [T]). Several cycles of the AngioVac system were performed with significant removal of thrombus. However, due to the dense structure, the thrombus could only be removed after applying a snaring device (GooseNeck®; Medtronic, Minneapolis, MN, USA) via a 6 Fr sheath (left CFA) to cut the thrombus in smaller pieces with the AngioVac system still operating distal to the thrombus to evacuate the mobile remnants (Panel C, Moving image 2). Eventually the whole thrombus could be removed successfully except for a small peduncle. The underlying PAU was then covered with an endovascular stent graft (Valiant™ Captivia™; Medtronic) (Panel D).
The postoperative course was uneventful and a six-month follow-up including a CTA of the aorta revealed an unremarkable stent graft without evidence of endoleak and no proof of remaining thrombus.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Transoesophageal echocardiography showing the pedunculated floating thrombus located in the aortic arch.
Moving image 2. Transoesophageal echocardiography showing the AngioVac catheter during thrombus suction process.
Supplementary data
To read the full content of this article, please download the PDF.
Transoesophageal echocardiography showing the pedunculated floating thrombus located in the aortic arch.
Transoesophageal echocardiography showing the AngioVac catheter during thrombus suction process.