Abstract
Background: In-stent restenosis (ISR), especially for neoatherosclerosis, is still a major problem of percutaneous coronary intervention (PCI) even in the drug-eluting stent (DES) era.
Aims: The purpose of this study was to investigate the impact of neoatherosclerosis on prognosis after PCI for ISR.
Methods: Between March 2009 and December 2017, 313 ISR lesions in patients undergoing an OCT-guided PCI in five hospitals were retrospectively enrolled. Neoatherosclerosis was defined as a lipid neointima or calcified neointima. We examined the association between neoatherosclerosis and the clinically driven target lesion revascularisation (CD-TLR) rates.
Results: In 313 ISR lesions, 64 lesions (20.4%) had bare metal stents and 241 lesions (77.0%) had drug-eluting stents (DES). Among them, 47.0% of lesions (147 lesions) had neoatherosclerosis. A multivariate logistic regression analysis demonstrated that eGFR (odds ratio [OR] 0.986, 95% confidence interval [CI]: 0.974-0.998; p=0.023), the time from PCI to the ISR (OR 1.13, 95% CI: 1.06-1.22; p<0.001) and DES-ISR (OR 2.48, 95% CI: 1.18-5.43; p=0.019) were independent predictors for neoatherosclerosis. A multivariate regression analysis demonstrated that neoatherosclerosis was an independent predictor of CD-TLR.
Conclusions: In this multicentre ISR registry, OCT imaging demonstrated that eGFR, the time from PCI to the ISR and DES-ISR were independent predictors for neoatherosclerosis and that neoatherosclerosis in ISR lesions had a worse impact on the CD-TLR rate.
Introduction
Drug-eluting stents (DES) have demonstrated superiority over bare metal stents (BMS). This has led to the near elimination of BMS from routine clinical practice1,2. However, in-stent restenosis (ISR) is still a major problem of percutaneous coronary intervention (PCI), especially for neoatherosclerosis, even in the DES era3. In fact, despite the better clinical outcomes with new-generation durable polymer DES, a pathological study demonstrated that the frequency of neoatherosclerosis was similar between the newer- and first-generation DES4. Moreover, a pathological study showed that neoatherosclerosis was associated with ISR in both BMS and DES implantation and it has been consistently correlated with late thrombotic events post stent implantation4. On the other hand, an assessment of the neointimal characteristics, especially of neoatherosclerosis, using optical coherence tomography (OCT), is important for clarifying the pathophysiology of ISR lesions. A few reports demonstrated the impact of neoatherosclerosis on clinical outcome5,6, though there are no data on the influence of neoatherosclerosis after PCI to the ISR. The purpose of this study was to investigate the influence of neoatherosclerosis on clinical outcome using plain old balloon angioplasty (POBA), DES and drug-coated balloons (DCB).
Methods
PATIENT POPULATION
This study was a multicentre, retrospective observational study. Between March 2009 and December 2017, ISR lesions undergoing an OCT-guided PCI in five different hospitals in Japan were retrospectively enrolled. The study exclusion criteria were haemodynamic instability, age less than 18 years, and a life expectancy of less than six months due to a non-cardiac condition. After excluding cases with incomplete OCT data and poor OCT quality, 313 ISR lesions in 311 patients were enrolled. This study was approved by the institutional review board of each participating institution with a waiver of the requirement for informed consent.
QUANTITATIVE CORONARY ANALYSES
Detailed methods are provided in Supplementary Appendix 1.
OCT IMAGE ACQUISITION
Detailed methods are provided in Supplementary Appendix 2.
OCT IMAGE ANALYSIS
The OCT analyses were performed using dedicated software with an automated contour-detection algorithm (Off-line Review Software, version E.0.2; Abbott Vascular, Santa Clara, CA, USA). All cross-sectional images were initially screened by a quality assessment and excluded from the analysis if any portion of the stent was out of the screen, a side branch occupied >45% of the cross-section, or the image was of poor quality caused by residual blood, artefact, or reverberations. A qualitative image assessment was performed for every frame, whereas quantitative measurements were performed every 1 mm along the entire stented segment. For the morphometric analysis, the standard definitions of the cross-sectional area measurement were applied as previously reported7. The stent, lumen, and neointimal hyperplasia cross-sectional areas were measured at 1.0 mm axial increments throughout the entire length of the stent. The proximal and distal references were measured at the site with the largest lumen within 5 mm proximal and distal to the stented segment. The neointima was defined as the tissue between the luminal contour and stent contour and estimated in all frames in the stent. A homogenous neointima was identified as having signal-rich regions with low attenuation. A calcified neointima had a well-delineated, signal-poor region with sharp borders. A lipid neointima was defined as having signal-poor regions with diffuse borders and a high attenuation8. Neoatherosclerosis was defined as a lipid or calcified neointima (Figure 1),8. In the lipid neointimas, the fibrous cap thickness was computed as the mean of three evenly distributed measurements along the fibrous cap8. A thin-cap fibroatheroma (TCFA) neointima was defined as a lipid neointima with a fibrous cap thickness of ≤65 µm at the thinnest part. Inter- and intra-observer variabilities were k=0.93 and k=0.93 for neoatherosclerosis, k=0.93 and k=0.86 for lipid neointima, and k=0.81 and k=0.81 for calcified neointima.
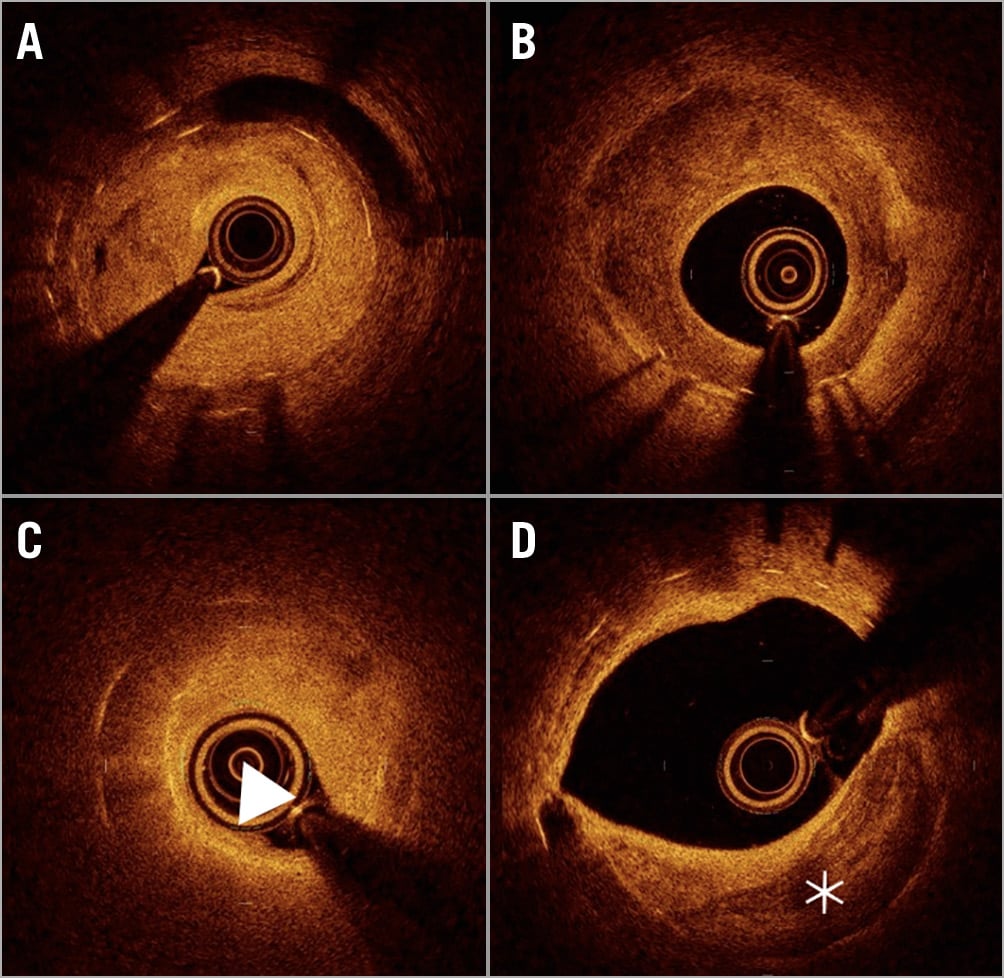
Figure 1. Representative optical coherence tomography image. A) Homogenous neointima. B) Heterogenous neointima. C) Lipid neointima (arrow). D) Calcified neointima (asterisk).
OUTCOME MEASURES
The clinical outcome data were obtained by reviewing the outpatient records for death, myocardial infarction, and target lesion revascularisation (TLR). The primary outcome was clinically driven target lesion revascularisation (CD-TLR). CD-TLR was defined as any revascularisation procedure of the target lesion in the presence of angiographic restenosis and signs or symptoms of ischaemia9. The secondary outcomes were CD-TLR in the DCB cohort, all-cause death, cardiac death, and target vessel myocardial infarction in the entire cohort.
STATISTICAL ANALYSIS
Data are presented as values and percentages, means±SD, or medians and interquartile ranges (IQR; Q1, Q3). Continuous variables were compared between the groups using the unpaired t-test or Mann-Whitney U test, based on the data distribution. Categorical variables were compared between the two groups with the chi-square test or Fisher’s exact test, as appropriate. Multiple lesions within the same patient were assumed to be independent of each other. First, multivariate logistic regression analysis was performed to determine the association of baseline characteristics with neoatherosclerosis. Age, sex, hypertension, current smoking, diabetes and haemoglobin A1c levels >7.0%, estimated glomerular filtration rate (eGFR, 1 mL/min/1.73 m2), >70 mg/dL of low-density lipoprotein (LDL) cholesterol, type of previous stent (BMS or DES), stent length and neointimal thickness were chosen as variables according to a previous report10. Results of the model are presented as the odds ratio (OR) and 95% confidence interval (CI).
Subsequently, the Kaplan-Meier method was used to estimate the cumulative probability of freedom from CD-TLR. A multivariable Cox proportional hazards regression model was used to evaluate the effect of neoatherosclerosis while adjusting for covariates including age, sex, current smoking, diabetes, eGFR (1 mL/min/1.73 m2), LDL cholesterol, type of previous stent, lesion length, and PCI strategy (POBA, or DES implantation). Results of the model are presented as the hazard ratio (HR) and 95% CI. Since a CD-TLR is a recurrent event, the Prentice, Williams and Peterson gap time (PWP-GT) model was also used to estimate the effect of neoatherosclerosis on CD-TLR while controlling for the above covariates11. The above analyses were also performed in the DCB cohort. All tests were two-sided with a 5% significance level. The statistical analyses were performed with R software, version 3.6.1 (R Foundation for Statistical Computing, Vienna, Austria; http://www.r-project.org).
Results
CLINICAL, LESION CHARACTERISTICS AND QCA
A total of 313 lesions (311 patients) with ISR were included (Figure 2). The baseline patient and lesion characteristics are shown in Table 1 and Table 2. In 313 ISR lesions, 64 lesions (20.4%) had bare metal stents and 241 lesions (77.0%) had drug-eluting stents (DES). Among 241 DES, 73 lesions had first-generation DES and 168 lesions had new-generation DES. In terms of the treatment strategy, DCB was performed in 62.2% of lesions, while DES were implanted in 16.7% of lesions.
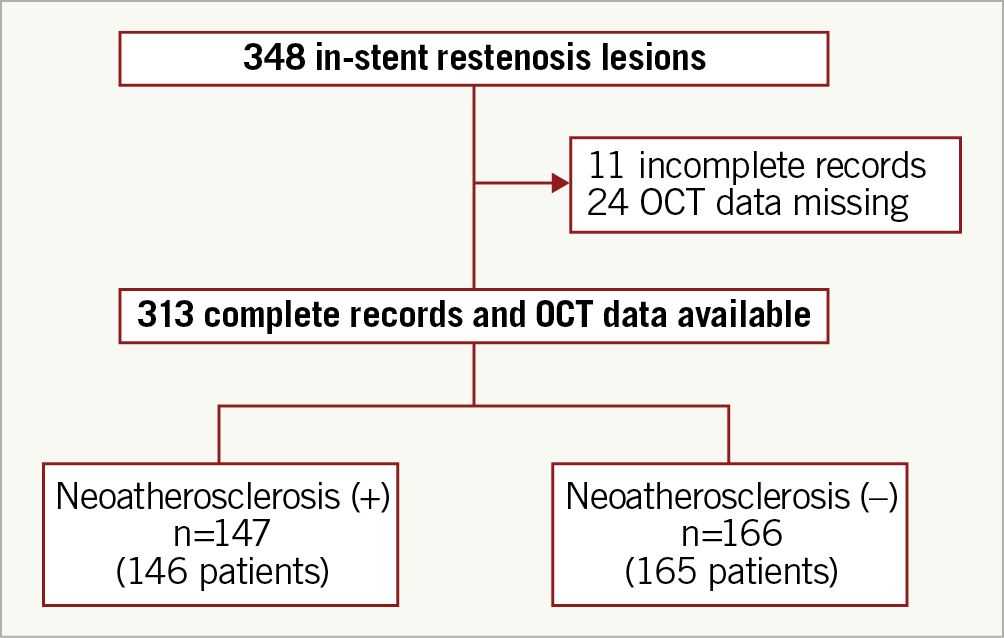
Figure 2. Flow diagram of the study. DCB: drug-coated balloon; DES: drug-eluting stent; OCT: optical coherence tomography; POBA: plain old balloon angioplasty
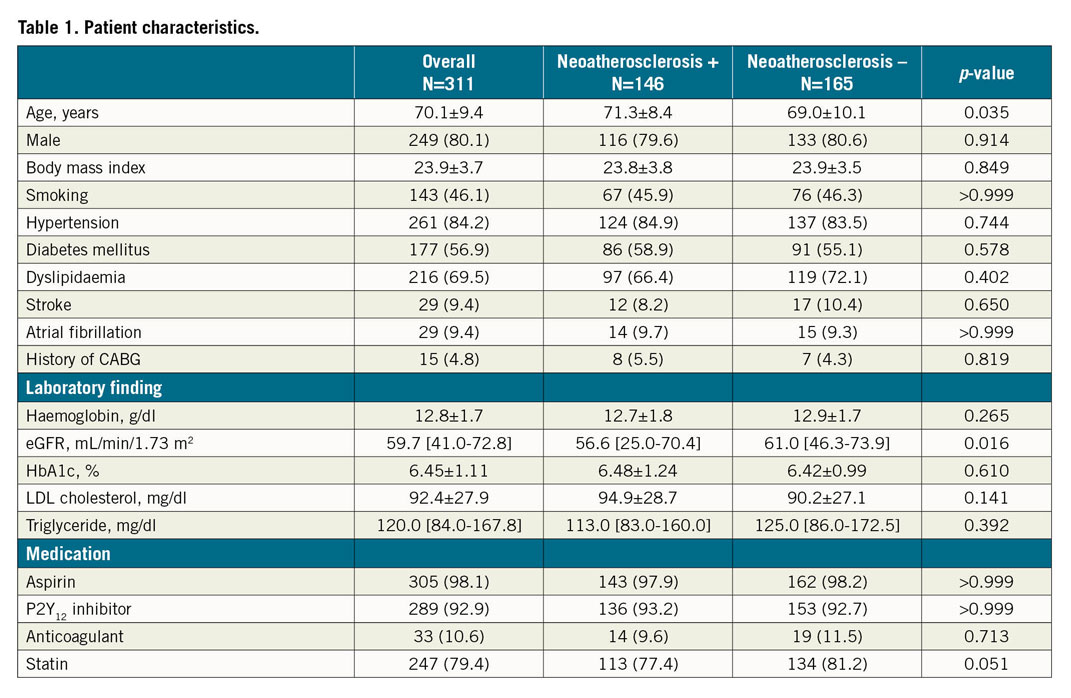
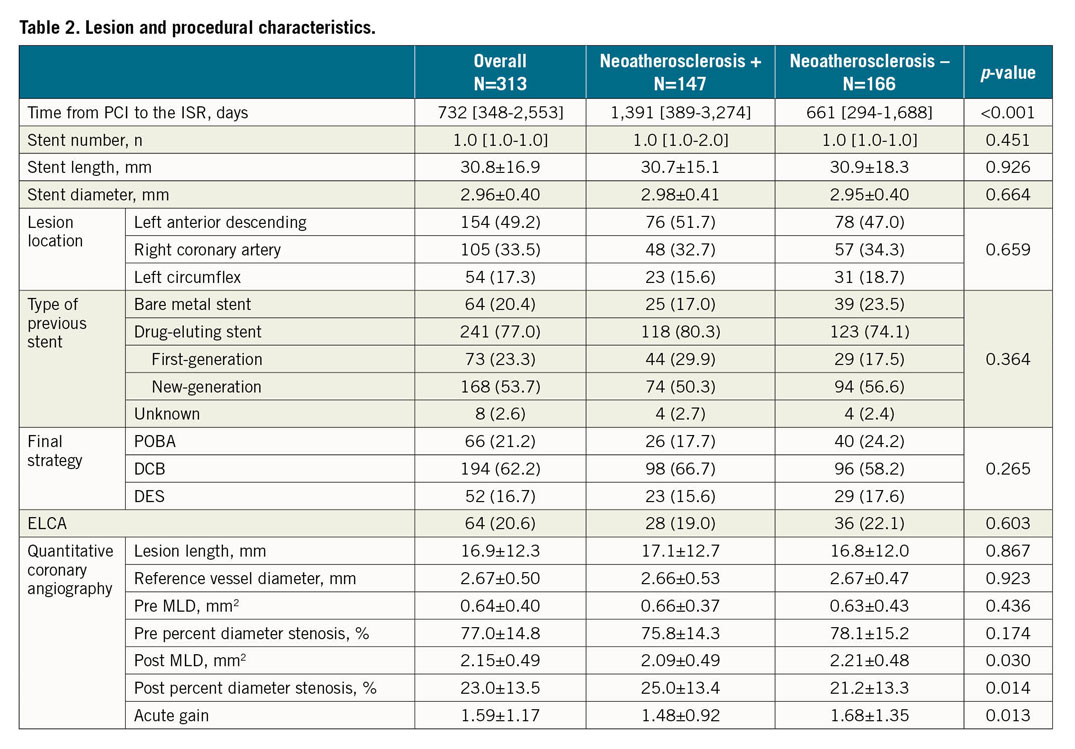
One hundred and forty-seven lesions (47%) had neoatherosclerosis in all lesions. Patients with neoatherosclerosis were significantly older compared to those without neoatherosclerosis (71.3±8.4 vs 69.0±10.1 years, p=0.035). The eGFR was significantly lower in the lesions with neoatherosclerosis (56.6 [25.0-70.4] vs 61.0 [46.3-73.9], p=0.016). The LDL-cholesterol level was higher in the neoatherosclerosis group, though it did not reach statistical significance (94.9±28.7 vs 90.2±27.1 mg/dl, p=0.141). The time from the index stent implantation to the ISR was significantly longer in the lesions with neoatherosclerosis (1,391 [389-3,274] vs 661 [294-1,688] days, p<0.001). The QCA analysis demonstrated that the post-PCI MLD and acute gain were significantly smaller in the neoatherosclerosis group (Table 3).
OCT FINDINGS
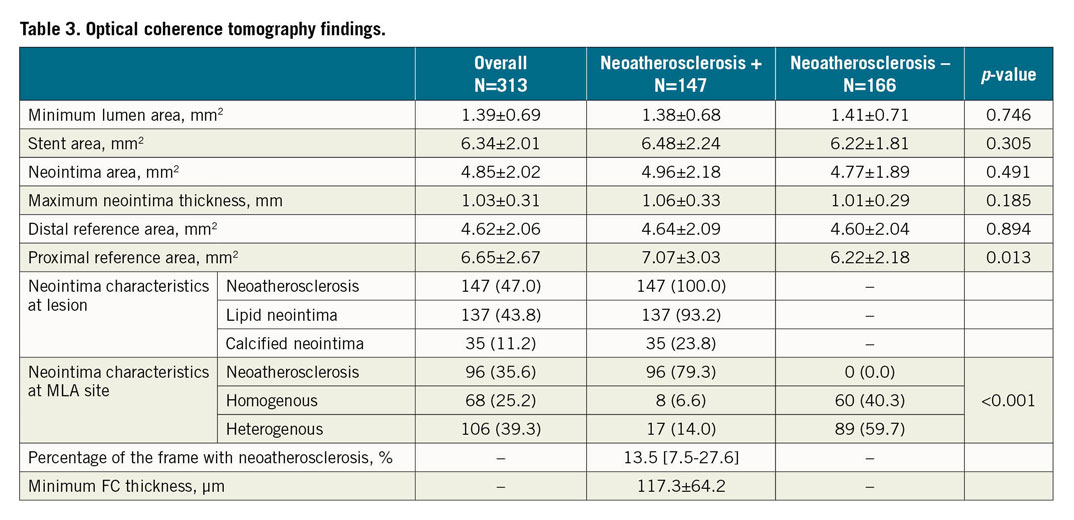
Details of the OCT findings are shown in Table 3. There were no significant differences in the minimum lumen area, stent area, and neointima area between the two groups. The proximal reference area was significantly greater in the lesions with neoatherosclerosis than in those without neoatherosclerosis. Lipid neointima and calcified neointima were detected in 93.2% and 23.8% of the lesions with neoatherosclerosis, respectively (Table 3). The minimum fibrous cap thickness and percentage of frames (longitudinal extension) with neoatherosclerosis in the entire stent segment were 117.3±64.2 µm and 13.5 [7.5-27.6] %, respectively.
PREDICTORS FOR NEOATHEROSCLEROSIS
In univariate logistic regression analysis, age, eGFR and the time from PCI to ISR were significantly associated with neoatherosclerosis (Table 4). Multivariate logistic regression analysis demonstrated that eGFR (OR 0.986, 95% CI: 0.974-0.998; p=0.023), the time from PCI to the ISR (OR 1.13, 95% CI: 1.06-1.22; p<0.001) and DES-ISR (OR 2.48, 95% CI: 1.18-5.43; p=0.019) were independent predictors for neoatherosclerosis (Supplementary Table 1).
CLINICAL OUTCOMES
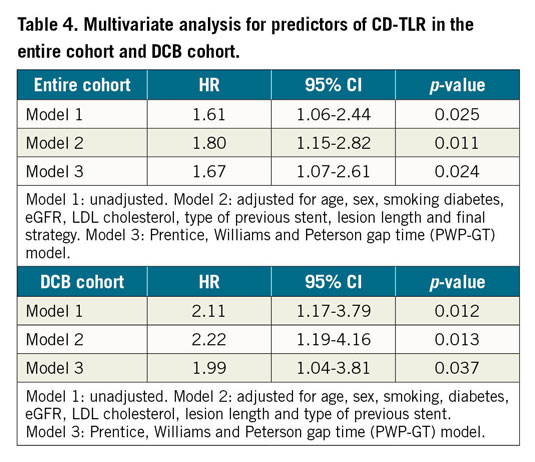
The mean follow-up period was 828.4±417.3 days. A Kaplan-Meier analysis demonstrated that the freedom from CD-TLR rate at three years was significantly lower in lesions with neoatherosclerosis than in those without (58.3% [95% CI: 49.2%-69.0%] vs 70.4% [95% CI: 62.5%-79.4%], p=0.024) (Figure 3). Multivariate analysis using the Cox proportional hazards model showed that neoatherosclerosis was an independent predictor of CD-TLR (HR 1.80, 95% CI: 1.15-2.82, p=0.011) (Table 4, Supplementary Table 2). There was no significant difference in the incidence of all-cause death, cardiac death, and target vessel myocardial infarction between patients with and without neoatherosclerosis (Supplementary Table 3).
![Figure 3. Kaplan-Meier analysis. The freedom from CD-TLR rate at two years was significantly lower in lesions with neoatherosclerosis than in those without (62.9% [95% CI: 54.5-72.6%] vs 77.9% [95% CI: 71.3-85.1%], p=0.024).](https://eurointervention.pcronline.com/storage/issues/EIJ192/086_EIJ-D-20-00539_Nakamura_192/medias/222200/03_Nakamura_192.png)
Figure 3. Kaplan-Meier analysis. The freedom from CD-TLR rate at two years was significantly lower in lesions with neoatherosclerosis than in those without (62.9% [95% CI: 54.5-72.6%] vs 77.9% [95% CI: 71.3-85.1%], p=0.024).
Taking into account the effect of the treatment strategy on CD-TLR, we investigated the impact of neoatherosclerosis on the CD-TLR for each strategy. The freedom from CD-TLR rate at three years was significantly lower in the cases with neoatherosclerosis (62.0% [95% CI: 51.8-74.3%] vs 77.2% [95% CI: 67.9-87.8%], p=0.011) (Figure 4) for the DCB cohort. It was lower in the cases with neoatherosclerosis for POBA (35.7% [95% CI: 20.0-63.6%] vs 65.0% [95% CI: 50.7-83.2%], p=0.040) (Figure 4), while there was no significant difference for DES (68.0% [95% CI: 38.0-100.0%] vs 62.6% [95% CI: 42.3-92.7%], p=0.300) (Figure 4). Similar to the entire cohort, in the DCB treatment group all multivariate models showed that neoatherosclerosis was an independent predictor of CD-TLR (HR 2.22, 95% CI: 1.19-4.16, p=0.013) (Table 4).
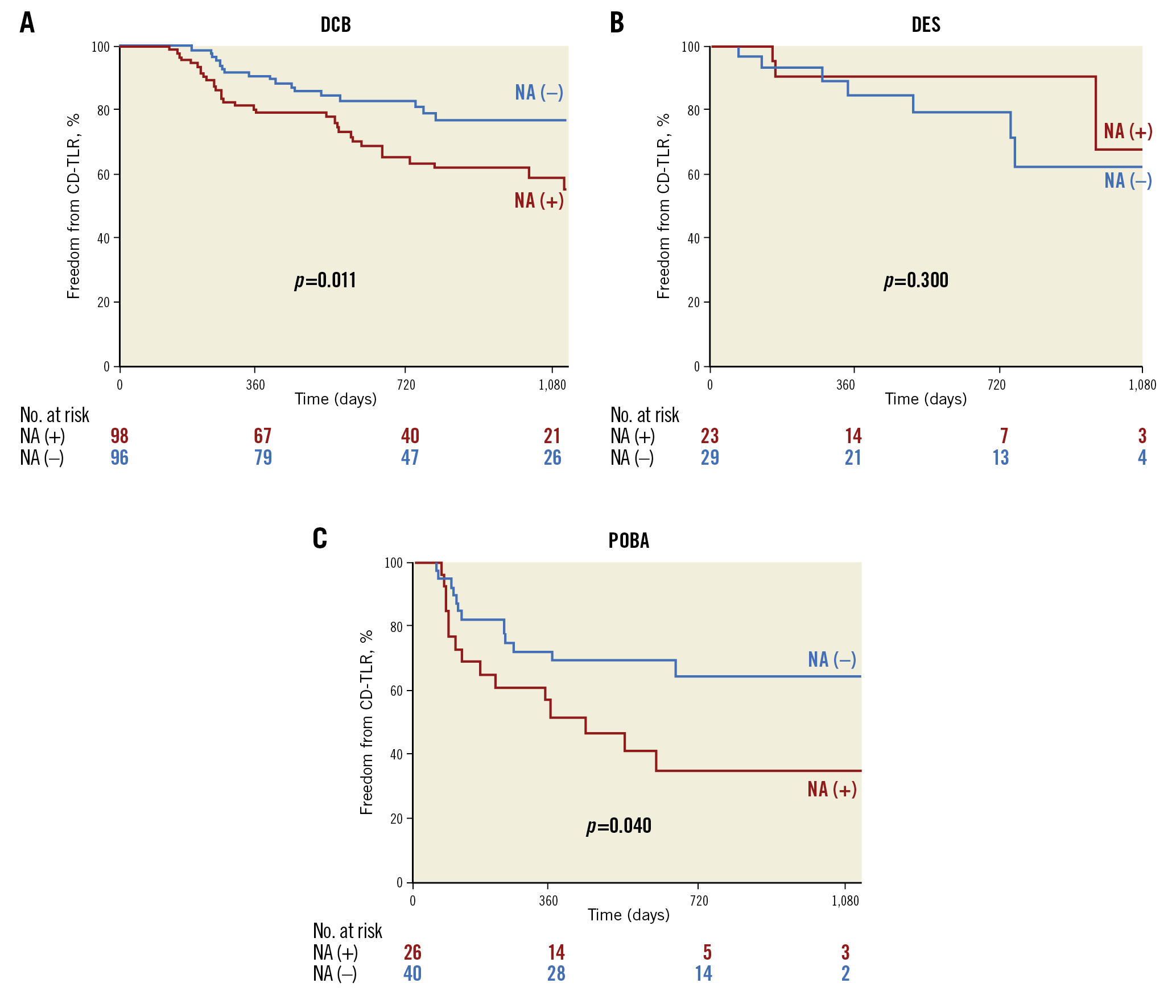
Figure 4. Kaplan-Meier curves for clinically driven target lesion revascularisation (CD-TLR) in each treatment. A) Freedom from CD-TLR at three years was significantly lower in lesions with neoatherosclerosis than in those without in the DCB treatment group. B) There was no significant difference for DES. C) The freedom from CD-TLR rate at three years was lower in cases with neoatherosclerosis for the POBA treatment group.
Among lesions with neoatherosclerosis, there was no significant difference in the freedom from CD-TLR rate between lesions with lipid neointima, calcified neointima and both lipid and calcified neointima (Supplementary Figure 1).
Discussion
This multicentre study had the largest population to date with ISR analysed by OCT. Its major findings were as follows: (1) the frequency of neoatherosclerosis was around 50% in ISR lesions; (2) multivariate logistic regression analysis demonstrated that eGFR, the time from PCI to the ISR and DES-ISR were independent predictors for neoatherosclerosis; and (3) neoatherosclerosis was an independent predictor of a CD-TLR both in the entire cohort and in the DCB treatment group.
FREQUENCY OF NEOATHEROSCLEROSIS
The evolution of DES, especially the introduction of newer-generation DES, has dramatically decreased the incidence of thrombotic events due to improvements in drug concentration and polymer design, simultaneously with maintaining a low rate of restenosis. Nevertheless, late stent failure remains a concern even with the use of newer DES, since clinical trials have shown that there is an increase in the cumulative incidence of TLR over time in all generations of DES12. In fact, despite the better clinical outcomes with newer-generation durable polymer DES, a pathological study demonstrated that the frequency of neoatherosclerosis was similar between the newer- and first-generation DES4. Moreover, a pathological study showed that neoatherosclerosis was associated with ISR in both BMS and DES implantation13, and it has been consistently correlated with late thrombotic events post stent implantation13,14. Yonetsu et al assessed 179 stents (mean duration 26.9 months, DES 59%) and reported OCT-detected neoatherosclerosis (lipid-laden neointima and/or calcification within the neointima) in 84 lesions (47%)15. Moreover. the prevalence of neoatherosclerosis in first-generation DES with restenosis beyond three years was 78% (7 of 9 lesions) at autopsy16. These results were compatible with the results of the current study.
FACTORS ASSOCIATED WITH NEOATHEROSCLEROSIS
Multivariate logistic regression analysis demonstrated that eGFR, the time from PCI to the ISR and DES use were associated with neoatherosclerosis. Several OCT studies have shown that neoatherosclerosis occurs regardless of the type of stent and polymer and is more dependent on the vulnerable plaque under the stent 5. One paper demonstrated that chronic kidney disease, a >70 mg/dL level of low-density cholesterol during the follow-up OCT, and the stent age were all independent predictors of neoatherosclerosis 17. As possible mechanisms, previous studies have shown that oxidative stress and inflammation might mediate the observed high frequency of cardiovascular disease in patients with chronic kidney disease 18. These mechanisms could also cause neoatherosclerotic changes in the stent.
In the present study, DES-ISR was associated more with neoatherosclerosis compared with BMS-ISR. This difference might be because of the difference in the mechanism of neoatherosclerosis between DES and BMS. In-stent neoatherosclerosis occurs in the years after stent implantation and more rapidly in DES when compared with BMS5. One histological paper demonstrated that accelerated neoatherosclerosis after DES implantation is probably a direct consequence of delayed vascular healing and inflammation caused by the antiproliferative drugs and polymers.
IMPACT OF NEOATHEROSCLEROSIS ON CLINICAL OUTCOMES
Previous reports in relation to OCT in PCI have suggested that the ISR and TLR rates of lesions with a homogeneous structure were significantly higher in the POBA group than in the DCB and DES groups, whereas there were no differences in the ISR and TLR rates among the three groups in lesions with a heterogeneous structure 19. There have been a few reports that have demonstrated the impact of neoatherosclerosis on clinical outcomes5,6. Kuroda et al demonstrated that neoatherosclerosis impacts on clinical outcome6. However, in that study, cases of neoatherosclerosis without ISR were enrolled and, moreover, PCI was not performed in any cases. The therapeutic strategy for ISR remains a challenge and there is no current consensus on how to treat ISR. However, finding an accurate diagnosis according to the characteristics of ISR is important for an appropriate therapy. The present findings might help to decide the strategy for ISR. Freedom from TLR after a DCB procedure was significantly lower in cases with neoatherosclerosis. Further improvement of DCB and DES is necessary for ISR treatment, especially for neoatherosclerosis.
Limitations
First, this was a non-randomised observational study. Second, there were no serial OCT data at the time of stent implantation. Third, qualitative definitions of tissue structure and tissue backscatter have some limitations. Tissue structure and backscatter are influenced by intima thickness and the position of the OCT catheter relative to the vessel wall. Fourth, there are no control data of OCT imaging without restenosis in the stent. Fifth, small-sized balloons which were used to predilate lesions might have affected the OCT analysis, though the incidence of cases with predilatation before OCT imaging was 22.0%. Sixth, this study included only patients with ISR undergoing OCT-guided PCI; therefore, there was possible selection bias.
Conclusions
In the multicentre ISR registry, OCT imaging demonstrated that eGFR, the time from PCI to the ISR and DES-ISR were independent predictors for neoatherosclerosis and that neoatherosclerosis in ISR lesions had a worse impact on the CD-TLR rate.
|
Impact on daily practice Despite better clinical outcomes with newer-generation durable polymer DES, a pathological study demonstrated that the frequency of neoatherosclerosis was similar between the newer- and first-generation DES. In this multicentre ISR registry, a multivariate logistic regression analysis demonstrated that eGFR, the time from PCI to the ISR and DES-ISR were independent predictors for neoatherosclerosis and multivariate regression analysis demonstrated that neoatherosclerosis was an independent predictor of CD-TLR. We should take into account additional strategies such as laser atherectomy. Also, further improvement of DCB and DES is probably necessary for the treatment of ISR. |
Acknowledgements
The authors thank John Martin for his linguistic assistance with this manuscript.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.