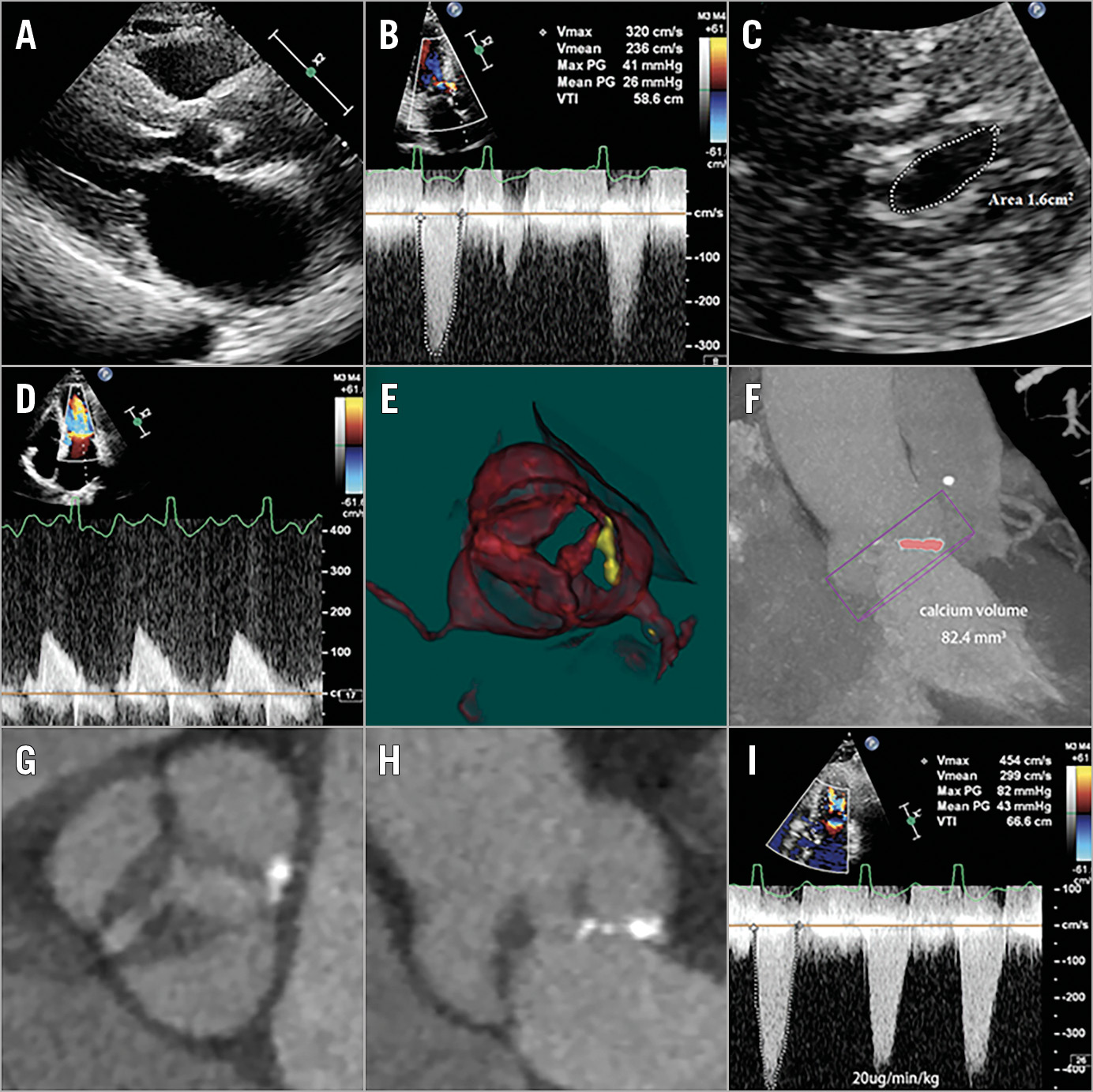
Figure 1. Echocardiography before and after DSE and fluoroscopic images. A) Transthoracic echocardiography suggesting a hypertrophied, small ventricle. B) Continuous wave Doppler echocardiogram showing moderate aortic stenosis (mean pressure gradient 26 mmHg, peak jet velocity 3.2 m/s). C) & D) Echocardiogram showing mild mitral stenosis. E) & F) Computed tomography showing a low calcium burden (calcium volume: 82.4 mm3) with significantly thickened leaflets (G & H). I) Peak jet velocity and mean pressure gradient increased to 4.5 m/s and 43 mmHg, respectively after DSE. DSE: dobutamine stress echocardiography
A 71-year-old male was admitted to our hospital for chest distress and dyspnoea. Transthoracic echocardiography (TTE) revealed concomitant aortic and mitral stenosis with significant thickening of both valves, suggesting rheumatic heart disease. The left ventricle was small and severely hypertrophied (Figure 1A). Haemodynamic measurements (ejection fraction [EF] 69%, stroke volume index 24.17 ml/m2, mean pressure gradient 26 mmHg, peak jet velocity 3.2 m/s, effective valve orifice area 0.7 cm2) (Figure 1B) suggested low-flow, low-gradient aortic stenosis (LFLG-AS) with preserved EF. There was also mild aortic regurgitation and mild mitral stenosis (MS) (Figure 1C, Figure 1D). The patient’s symptoms were mismatched with his AS severity as assessed by the mean gradient, but otherwise unexplainable. Despite the low calcium burden (calcium volume: 82.4 mm3) detected on contrast computed tomography with the threshold set at 850 HU (Figure 1E, Figure 1F), severe AS was considered very likely based on clinical background and imaging data available. Thus, a low-dose dobutamine stress echocardiography (DSE) was performed1 (Figure 1G, Figure 1H), which confirmed severe AS (Figure 1I). The patient ultimately underwent transcatheter aortic valve replacement and experienced profound symptom improvement.
Typically, AS is characterised by calcific degeneration. Therefore, calcium scoring is of critical importance in the assessment of AS severity in the entity of LFLG-AS with preserved EF according to current guidelines2. However, rheumatic AS featuring diffuse fibrosis and commissural fusion is not rare in developing countries. In this paper, we demonstrated an example of “paradoxically” severe LFLG-AS in the presence of only mild valve calcium. The case suggested that the absence of severe valve calcium could not exclude severe AS in the entity of LFLG-AS with preserved EF, where DSE could be helpful. Patients with this entity could suffer from severe AS and require timely interventions.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.