Abstract
Aims: Radiation exposure and prolonged procedure time continue to limit the complexity of CTO-PCI procedures attempted. This study aimed to assess the impact of radiation dose-limiting equipment on radiation dosage and fluoroscopic time in chronic total occlusion (CTO) percutaneous coronary interventions (PCI).
Methods and results: Retrospective clinical and dosimetric data from diagnostic catheterisations (DXC) and CTO-PCI procedures performed on one of three variants of interventional fluoroscopic equipment were collected. Fluoroscopic time, air kerma, kerma area product and contrast utilisation were stratified by procedure type and compared among equipment types. To standardise comparisons among equipment configurations, an efficiency index (EI) was calculated. In total, 2,947 DXC and 276 CTO-PCI procedures were studied. For DXC, radiation dose (AK) decreased by 45% (despite modest increases in fluoroscopic time [FT]) between the reference (REF) and moderately dose-optimised (ECO) machines. A further 20% decrease in AK was observed on the highly dose-optimised machine (CLA). For CTO-PCI, AK declined by almost half (48%), despite a 76% increase in FT and higher procedural success rates (69.8% versus 83.0%) between REF and CLA.
Conclusions: Novel dose-optimised fluoroscopic equipment allows longer FT with a decrease in radiation dose to both patient and operator. This should allow operators to undertake increasingly longer and more complex procedures and reduce operators’ lifetime irradiation.
Abbreviations
AK: air kerma
BSA: body surface area
BMI: body mass index
CLA: AlluraClarity FD20 system
CTO: chronic total occlusion
CVOL: contrast volume
DXC: diagnostic cardiac catheterisation
ECO: Allura Xper FD20 system
EI: efficiency index
FT: fluoroscopic time
Gy: gray
KAP: kerma area product
mGy: milligray
PCI: percutaneous coronary intervention
REF: Allura Xper FD10 system
RSI: radiation-induced skin injury
Introduction
Percutaneous coronary intervention (PCI) in chronic total occlusions (CTO) is associated with longer fluoroscopic times and increased radiation dosage to both the patient and operator1. Though fluoroscopic time, contrast use, and radiation exposure in CTO interventions decrease with commensurate increases in operator experience2, prolonged procedure time and radiation exposure remain salient issues.
Accurate assessment of radiation use transcends fluoroscopic time (FT), which fails to consider cine-acquisition imaging, patient size, X-ray-beam filter use, collimation and table/image receptor positioning. Two standard radiation dosage parameters are kerma area product (KAP) and air kerma (AK). KAP monitors the potential for patient stochastic radiation effects and is a surrogate for operator radiation exposure3. AK monitors overall cumulative X-ray energy delivery to an interventional reference point and estimates the likelihood of radiation-induced skin injury (RSI)4. Below 5 Gy, clinically significant RSI is unlikely, whereas, at exposures greater than 10 Gy, surgical intervention may be necessary5.
Optimising radiation management requires continuous attention to operator education, fluoroscopic maintenance, system configuration, and technological advances. One such advance is the Philips AlluraClarity FD20 (CLA; Philips Healthcare, Amsterdam, the Netherlands), a novel imaging platform utilising advanced image processing hardware that may allow substantial patient and operator dose reduction.
This paper examines fluoroscopic radiation dose variation and contrast media utilisation during diagnostic cardiac catheterisations (DXC) and CTO-PCI performed on three fluoroscopic equipment configurations at a high-volume, quaternary care PCI centre.
Methods
Clinical and dosimetric data for DXC and CTO procedures, performed between 2012 and 2014 on three different fluoroscopic configurations, were retrospectively reviewed. Key equipment parameters are outlined in Table 1.
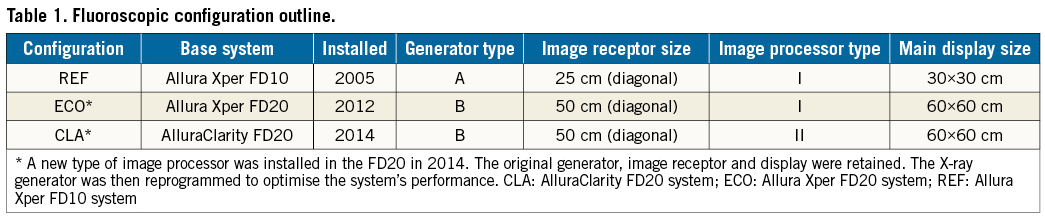
All systems were manufactured and maintained by Philips Healthcare to as close to “state-of-the-art performance” as possible. The Allura Xper FD10 X-ray system (REF; Philips Healthcare) was state of the art when it was installed in 2005. In 2012, the installation of the Allura Xper FD20 X-ray system (ECO; Philips Healthcare) allowed progressively lower procedural fluoroscopic and cine dose rates than those possible on the FD10. The FD20 image processor was upgraded two years later (with generator reprogramming) to create a third configuration, AlluraClarity FD20 (CLA).
Operators were free to select any clinically available dose rate and frame rate before or during any procedure (default frame rate for CTO-PCI of 7.5 frames/s was used). Integrated dosimeters monitored AK and KAP, calibrated biannually (correction factors 0.89-1.08 over the study). All rooms were equipped with standard operator scatter-reduction technologies.
Operator and procedural scheduling was determined by laboratory workflow and physician preference. Effectively, DXC were randomly distributed among all procedure rooms and operators. As operators became aware of inter-equipment differences, CTO-PCI procedures were scheduled almost exclusively in labs with dose-efficient equipment.
The Japanese Chronic Total Occlusion score (J-CTO score) predicts the probability of wiring a given CTO within 30 minutes6. High J-CTO scores and the use of retrograde recanalisation techniques predict longer procedure times and indicate complex lesion subsets7; these factors were used herein to denote procedural complexity. Procedural success was defined as successful CTO recanalisation with TIMI 3 flow in the target vessel at the conclusion of the procedure.
STATISTICAL ANALYSIS
Descriptive data are presented as frequencies and percentages for categorical variables, or as median and interquartile value ranges and median±standard deviations (SD) for continuous variables. Statistical significance was set at p<0.05.
Normality of distributions was established using the Shapiro-Wilk test. For normally distributed data, the ANOVA F-test for multiple comparisons was used to detect differences between group means. For non-normally distributed data, the Mann-Whitney U test or the Kruskal-Wallis test was used to detect differences between group medians. Finally, a post hoc Tukey’s test on the log-transformed outcome was utilised for pairwise comparisons. The median difference and the median percent change of pairwise configurations were calculated for each outcome. The Kruskal-Wallis test was then used to determine whether a significant difference existed between pairwise configurations. Using the Bonferroni correction method, the significant level of comparisons between configuration medians was set at p<0.05/3=0.017.
Efficiency indices (EI) and the mean differences of pairwise configurations were calculated for each procedure. The Student’s t-test was used to detect differences between pairwise configurations.
All statistical analyses were conducted using SAS software, version 9.3 (SAS Institute, Cary, NC, USA).
ETHICS AND FUNDING
This study was approved by the local institutional review board. The study was funded in part by Philips Healthcare. However, the evaluation protocol, investigation, data analysis, and preparation of the manuscript were performed entirely by the authors with no input from the study sponsor.
Results
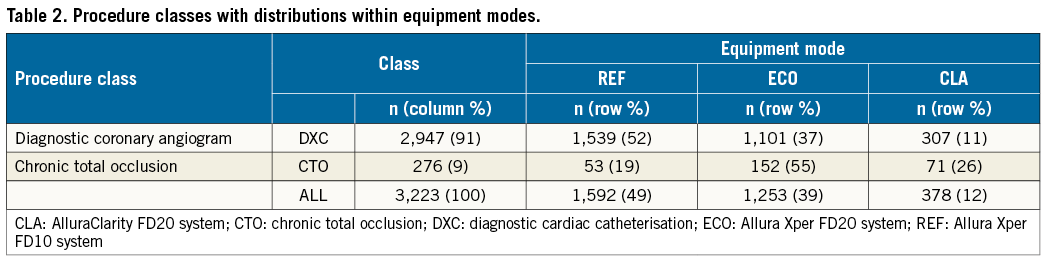
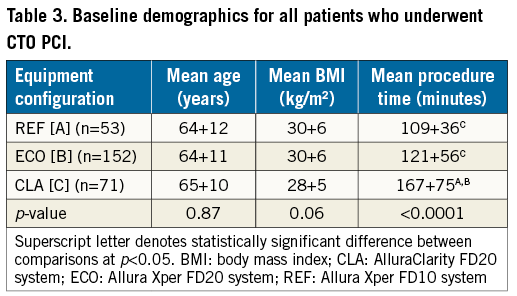
Data from 2,947 diagnostic coronary angiograms and 276 CTO-PCI procedures were analysed. Forty-eight percent of DXC were performed using one of the two radiation dose-optimising configurations (ECO or CLA). Eighty-one percent of CTOs were performed using an optimising configuration (Table 2). For CTO cases, demographic characteristics (including age and BMI) were similar, regardless of equipment configuration (Table 3).
DIAGNOSTIC CORONARY ANGIOGRAMS
Summary statistics for DXC are shown in Table 4. Radiation use, expressed as median AK, declined by 45% when going from REF to ECO. There was a further decline of 20% between ECO and CLA. The overall decline (REF to CLA) was 56%. All of these differences were highly significant (p<0.0001). Median KAP also declined as follows: REF to ECO 34%, ECO to CLA 15%, and REF to CLA 44% (p<0.0001 for all comparisons). Median FT increased significantly, by 7% between REF and ECO (p<0.001) and by 19% between REF and CLA (p=0.002).
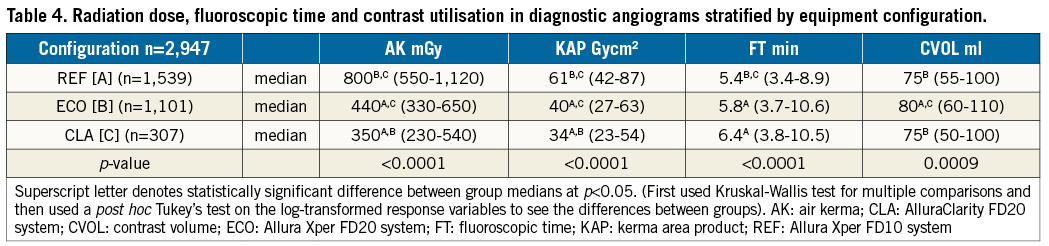
Contrast use increased by 7% going from REF to ECO (p<0.001), was unchanged for REF to CLA (p=0.46), and actually declined by 6% from ECO to CLA (p<0.001). Of note, contrast use decreased from ECO to CLA despite an increase in FT between these configurations.
CHRONIC TOTAL OCCLUSIONS
Summary statistics for CTOs are shown in Table 5 and Figure 1. Radiation use (median AK) declined 43% between REF and ECO (p<0.001), an additional 9% between ECO and CLA (p=0.2) and 48% between REF and CLA (p<0.001). Corresponding KAP declines were: REF to ECO 23% (p=0.01), ECO to CLA 6% (p=0.43) and REF to CLA 28% (p=0.01).
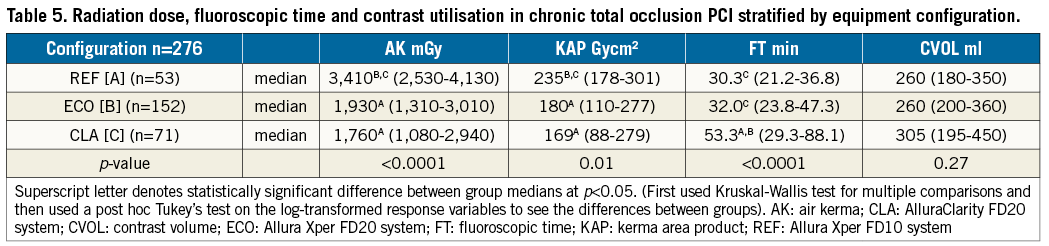
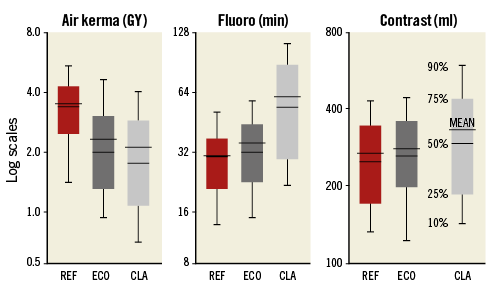
Figure 1. Graphical representation of mean, median, and percentile values for AK, FT and contrast volume (CVOL) among all three fluoroscopic machines for CTO-PCI. REF: Allura Xper FD10 system; ECO: Allura Xper FD20 system; CLA: AlluraClarity FD20 system
With respect to FT, despite an increase of 23 minutes between REF and CLA (p<0.001), a highly significant decrease of 48% in AK was observed. When comparing FT to cine run time (FT/CR) among the equipment modes, a significant difference between mean FT/CRs was also noted. Mean FT/CR ranks for CLA and ECO were 139.1 and 140.9 versus only 108.1 for REF (H=7.48, df 2, p=0.02), indicating relatively higher use of fluoroscopy versus cine acquisition in both dose-optimised rooms.
No significant difference in contrast use among any of the three configurations was observed.
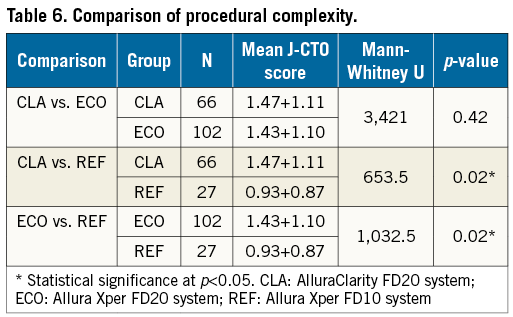
Procedural complexity was higher in CLA cases; retrograde techniques were used in 36% of CLA cases compared to only 12% in ECO and 0% in REF. Significantly higher J-CTO scores in CLA and ECO cases were also observed (Table 6). Despite higher complexity, there was a trend towards higher procedural success, going from REF (69.8%) or ECO (68.5%) to CLA (83%) (p=0.05), and a decrease in cases with total AK over 5 Gy (15% for REF versus 7% for ECO and only 4% for CLA, p=0.08).
EFFICIENCY INDEX
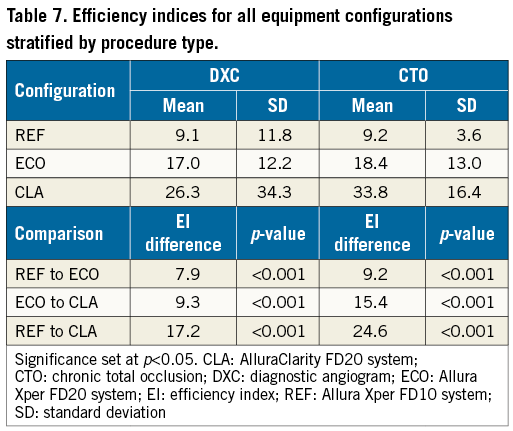
An efficiency index (EI) was calculated using clinical data from each procedure. This metric is the fluoroscopic time used for acomplete procedure divided by the total procedural AK (fluoro+cine). Thus, the EI is defined as:
![]()
It is the analogue of computing the average “miles-per-gallon” after a trip. A higher EI indicates equipment that highly optimises radiation dosage and thus maximises safe procedural time. EIs for the three equipment configurations, stratified by procedure class, are shown in Table 7.
Discussion
Our study evaluated the effect of radiation dose-reducing fluoroscopic technologies on key parameters during diagnostic coronary angiography and coronary CTO interventional procedures. The results of our study suggest that this technology successfully lowers radiation dose, despite longer FT.
Diagnostic coronary angiograms are amongst the most common procedures performed in today’s catheterisation labs, capturing similar information regardless of the site at which they are performed. As such, the DXC is used to determine national and international radiation reference levels4,8-16. In DXCs, we demonstrated highly significant AK and KAP reductions of 45% and 34%, respectively, between the REF and ECO configurations, and additional 20% and 15% reductions between ECO and CLA (p<0.001). The reductions with ECO and CLA occurred despite slightly longer fluoroscopic times, confirming that FT is not a reliable indicator of the radiation dose delivered during DXC. Further, though FT was somewhat longer using ECO and CLA versus REF, only minimal variation in contrast use was observed. Hence, it is possible that, although DXC procedure times may be slightly longer with the use of dose-optimised fluoroscopic equipment (total increase in FT of 1.0 minutes between REF and CLA), the additional FT may be due to other aspects of the procedure (e.g., arterial access, wire navigation, catheter manipulation, etc.) and not from poor coronary visualisation.
CTOs are identified in up to 30% of all patients with coronary artery disease17. Still, despite the body of evidence suggesting the clinical benefits of successful CTO-PCI18-21, these procedures represent only 3.8% of the total PCI volume performed in the USA22, with national success rates of only 58%. Contemporary data from expert US centres23,24 have shown success rates of 80-90% with acceptable complication rates (1-3%)24,25. CTO-PCI procedures are longer, require more contrast than standard PCI and utilise specialised equipment that can take considerable time to deliver. Herein, we confirmed previous work, demonstrating longer procedure times and overall radiation exposure during CTO-PCI1,26. A significant decrease in AK of nearly 50% was seen in CTO-PCI procedures performed on the ECO and CLA systems versus the standard REF system. Notably, this decrease occurred despite important increases in FT (75% between REF and CLA), without significant increases in contrast usage, despite higher procedural complexity (Table 6) and without overt concerns regarding image quality from the operators. As such, even in the hands of highly experienced/senior CTO operators, whose skills may facilitate efficient progress through procedures, important decreases in AK are achievable using dose-optimised equipment. Further, given the improvement in procedural success rates achieved on the CLA system despite higher procedural complexity, our data suggest that radiation-optimised equipment may facilitate procedural success by allowing longer procedural duration without the risk of excessive patient and operator radiation exposure.
The efficiency index is a clinical indicator of imaging equipment performance. The EI may be thought of as a measure of the fluoroscopy time available to an operator within a given total (fluoro+cine) radiation limit. A higher EI indicates better radiation-optimised equipment for a given procedure type. As shown in Table 7, EI increased significantly from REF to ECO to CLA (p<0.001 for all comparisons) for both DXC and CTO procedures. Comparisons of EI between DXC and CTO were not significant for any equipment mode (REF p=0.931; ECO p=0.203; CLA p=0.074), indicating good internal consistency of the EI measure and that technology improvements were equally beneficial across procedure types.
Many studies over the past decade have examined the issue of radiation exposure during DXC and PCI12-16,27-36. Overall, our results are in agreement with the literature, demonstrating an important decrease in overall radiation dose delivered with the use of radiation dose-optimising equipment. The results of our study also underscore the lack of utility of FT alone as a true measure of radiation exposure.
Limitations
Several study limitations warrant mention. Firstly, though all operators were highly experienced and employed radiation-limiting strategies, differences in operator radiation setting preferences and speed/skill may have ultimately influenced the final radiation dose delivered in each room independently from fluoroscopic technology. Secondly, differences in operator skill and case selection may have influenced success rates due to reasons other than radiation limits and procedural time. Finally, though EI is an intuitive measure, the most appropriate usage of this parameter requires prospective study and further validation.
Conclusions
Both the feasibility and success of CTO-PCI have increased substantially over the past 10 years. Limitations to procedural success are now more focused on the limitations of the angiographic equipment and fluoroscopic imaging technologies.
Herein, we have shown that improved fluoroscopic generator technology (ECO) and a novel image processor (CLA) can reduce overall radiation dose (AK) by approximately 50% in both DXC and CTO-PCI. Significant radiation reductions were achieved despite increases in fluoroscopy time and contrast use, suggesting that these novel imaging technologies may facilitate the performance of increasingly complex procedures without encountering radiation dosage limitations. Further, this study failed to document an important increase in contrast usage due to longer procedures or low-dose images. In view of these findings, the workflow in our catheterisation laboratories has changed to place complex procedures preferentially in rooms with dose-optimised fluoroscopic equipment. This will probably become the standard as radiation-limiting technologies become mainstream.
| Impact on daily practice Dose-optimising fluoroscopic equipment reduces patient and operator radiation during both diagnostic and complex CTO-PCI procedures with no change in contrast utilisation despite longer fluoroscopic times. This has the potential to change practice by allowing operators to attempt highly complex procedures without the limitation of excessive patient or operator radiation exposure. Such equipment also has the potential to reduce the overall radiation burden borne by operators throughout their careers in interventional cardiology. |
Funding
The study was funded in part by Philips Healthcare. The sponsor had no input whatsoever on the evaluation protocol, investigation, data analysis, and preparation of the manuscript.
Conflict of interest statement
S. Kalra is on the speaker’s bureau of Abiomed and Servier Canada. A. Kirtane has received institutional research grants from BSC, Medtronic, Abbott Vascular, St. Jude Medical, CathWorks, Siemens, Abiomed, and Eli Lilly. D. Karmpaliotis is on the speaker’s bureau of Abbott Vascular, Medtronic, Boston Scientific, and is a consultant for Vascular Solutions. The other authors have no conflicts of interest to declare.