Abstract
Aims: There are limited data on the trends and outcomes of mechanical circulatory support (MCS)-assisted early percutaneous coronary intervention (PCI) in acute myocardial infarction with cardiogenic shock (AMI-CS). In this study, we sought to assess the use, temporal trends, and outcomes of percutaneous MCS-assisted early PCI in AMI-CS.
Methods and results: Using the National Inpatient Sample database from 2005-2014, a retrospective cohort of AMI-CS admissions receiving early PCI (hospital day zero) was identified. MCS use was defined as intra-aortic balloon pump (IABP), percutaneous left ventricular assist device (pLVAD) and extracorporeal membrane oxygenation (ECMO) support. Outcomes of interest included in-hospital mortality, resource utilisation, trends and predictors of MCS-assisted PCI. Of the 110,452 admissions, MCS assistance was used in 55%. IABP, pLVAD and ECMO were used in 94.8%, 4.2% and 1%, respectively. During 2009-2014, there was a decrease in MCS-assisted PCI due to a decrease in IABP, despite an increase in pLVAD and ECMO. Younger age, male sex, lower comorbidity, and cardiac arrest independently predicted MCS use. MCS-assisted PCI was predictive of higher in-hospital mortality (31% vs 26%, adjusted odds ratio 1.23 [1.19-1.27]; p<0.001) and greater resource utilisation. IABP-assisted PCI had lower in-hospital mortality and lesser resource utilisation compared to pLVAD/ECMO.
Conclusions: MCS-assisted PCI identified a sicker AMI-CS cohort. There was a decrease in IABP and an increase in pLVAD/ECMO.
Introduction
Acute myocardial infarction (AMI) continues to be a leading cause of cardiovascular death and is associated with 30-45% mortality in patients with concomitant cardiogenic shock (CS)1,2,3,4,5. Contemporary guidelines from United States societies recommend emergent revascularisation in all ST-elevation myocardial infarction (STEMI) and non-ST-elevation myocardial infarction (NSTEMI) patients with haemodynamic instability6,7. Patients with AMI-CS are at a high risk for decompensation due to pre-existing left ventricular dysfunction, higher comorbidity, concomitant multivessel disease and complex coronary anatomy8. Percutaneous left ventricular assist devices (pLVAD) and extracorporeal membrane oxygenation (ECMO) are increasingly being used in the management of CS along with a decrease in intra-aortic balloon pump (IABP) use5,9,10,11. There are limited contemporary data on the concomitant use of MCS to support early PCI in AMI-CS12,13,14. Using a 10-year nationally representative database, we sought to assess the use, temporal trends and outcomes of percutaneous MCS-assisted early PCI (hospital day zero) in AMI-CS.
Methods and material
STUDY POPULATION, VARIABLES AND OUTCOMES
The Healthcare Quality and Utilization Project – National Inpatient Sample (HCUP-NIS) is the largest all-payer database of hospital inpatient stays, containing discharge data from a 20% stratified sample of community hospitals in the USA15. Similar to prior literature, using previously validated methodology, a retrospective study cohort of admissions with AMI-CS was identified from the HCUP-NIS database from January 2005 to December 20141,2,3,4,9,10. Because the International Classification of Diseases 9 Clinical Modification (ICD-9CM) codes were redefined in 2005 to distinguish between permanent MCS and short-term non-implantable devices, admissions before 2005 were excluded from this study9,10. AMI in the primary procedure field were identified using ICD-9CM codes 410.1x-410.9x and a secondary diagnosis of CS by ICD-9CM 785.5116. Early PCI was defined as PCI performed on hospital day zero. We used the procedure day for IABP (ICD-9CM 37.61), pLVAD (ICD-9CM 37.68), and ECMO (ICD-9CM 39.65) to time the MCS placement on the same day as the PCI procedure14. Demographic characteristics, hospital characteristics, primary payer, acute organ failure, organ support and comorbidities (Deyo’s modification of the Charlson Comorbidity Index) were abstracted (Supplementary Table 1),1,2,3,4,17,18,19,20,21,22.
The primary outcome was the frequency, utilisation trends, and predictors for MCS use in early PCI in AMI-CS. Secondary outcomes included in-hospital mortality, length of stay, and discharge disposition in admissions with AMI-CS that received MCS-assisted PCI in comparison to those that received early PCI alone.
STATISTICAL ANALYSIS
As recommended by HCUP-NIS, survey procedures using discharge weights provided with the HCUP-NIS database were used to generate national estimates. Using the trend weights provided by the HCUP-NIS, samples from 2000-2011 were re-weighted to adjust for the 2012 HCUP-NIS re-design23. Using trend weights available on the HCUP-NIS database, samples from 2000-2011 were retroactively re-weighted. The new sampling strategy is expected to result in more precise estimates than the previous HCUP-NIS design by reducing sampling error15. All analyses were conducted accounting for clustering of admissions within a hospital (HOSP_NIS), weighting (DISCWT), and stratification (NIS_STRATUM) of the NIS consistent with prior data24. Chi-square and t-tests were used to compare categorical and continuous variables, respectively. Univariable analysis for trends and outcomes was performed. These were represented as odds ratio (OR) with 95% confidence interval (CI). Multivariable logistic regression analysis was performed for predictors of MCS use and in-hospital mortality. To confirm the results of the primary findings, subgroup analyses stratifying admissions by age, sex, race, type of AMI and presence of cardiac arrest were performed. In the MCS-assisted PCI cohort, a priori comparison of pLVAD and ECMO to IABP was performed. A two-tailed p<0.05 was considered statistically significant. All statistical analyses were performed using SPSS, Version 25.0 (IBM Corp., Armonk, NY, USA).
Results
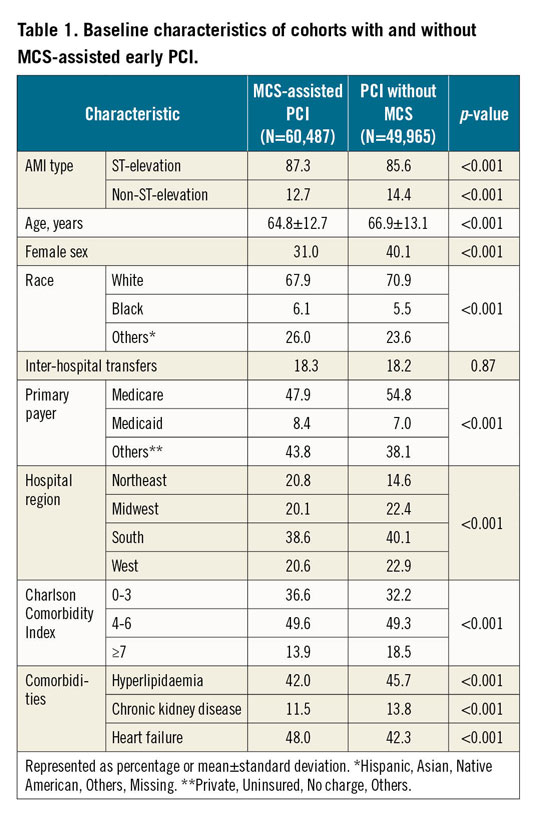
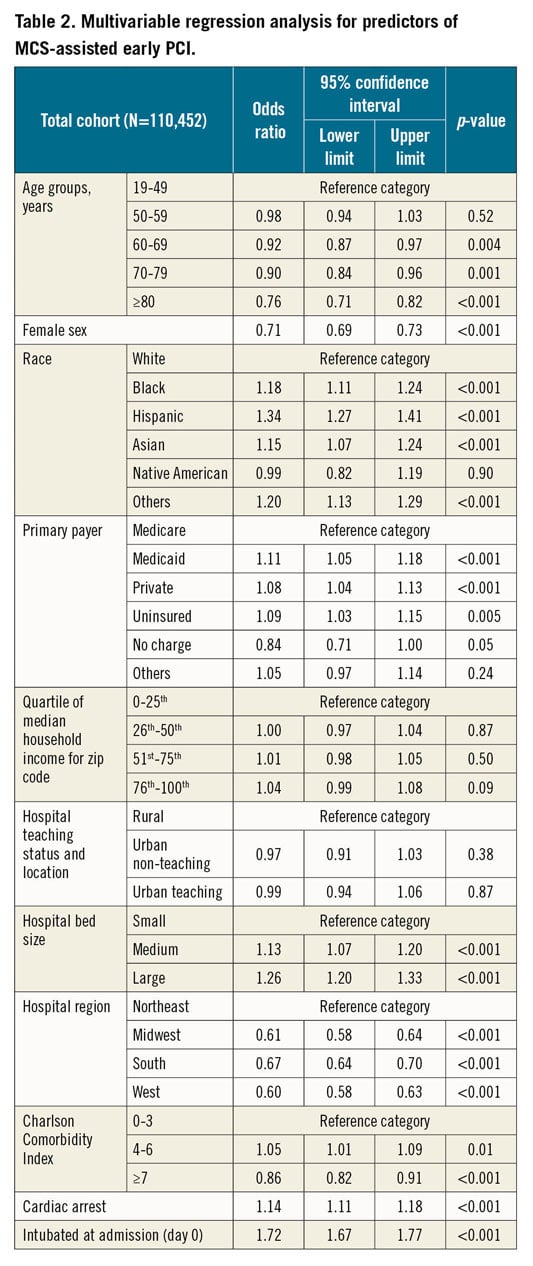
There were an estimated 6,111,445 admissions for AMI between January 2005 and December 2014, of which early PCI (hospital day 0) for AMI-CS was performed in 110,452 admissions (Figure 1A, Figure 1B). There was an overall increase in the total admissions for AMI-CS receiving early PCI in this study period, with 86.5% encompassing ST-elevation AMI-CS. Percutaneous MCS was used concomitantly with early PCI in 60,487 (54.8%) admissions, with the IABP in 57,337 (94.8%), pLVAD in 2,568 (4.2%) and ECMO in 582 (1.0%). IABP remained the predominant MCS device of choice, though there was a decrease in use from 2009 (Figure 2A, Figure 2B). MCS-assisted PCI was performed more frequently in admissions that were younger, male and non-white, and with lower comorbidity (Table 1, Supplementary Table 2). The MCS-assisted PCI cohort had higher rates of cardiac arrest (26% vs 21%; p<0.001) and respiratory failure requiring endotracheal intubation (40% vs 28%; p<0.001) on admission. During the hospital course, the MCS-assisted PCI cohort developed higher rates of non-cardiac organ failure (Supplementary Table 2). Temporal trends of MCS-assisted PCI stratified by patient and hospital characteristics are presented in Supplementary Figure 1 and Supplementary Figure 2. Multivariable logistic regression analysis for predictors of MCS use for early PCI is presented in Table 2. Younger age, male sex, non-white race, lower comorbidity, non-Medicare insurance, concomitant cardiac arrest, endotracheal intubation, and admission to a medium- or large-sized hospital were independent predictors of MCS use for early PCI.
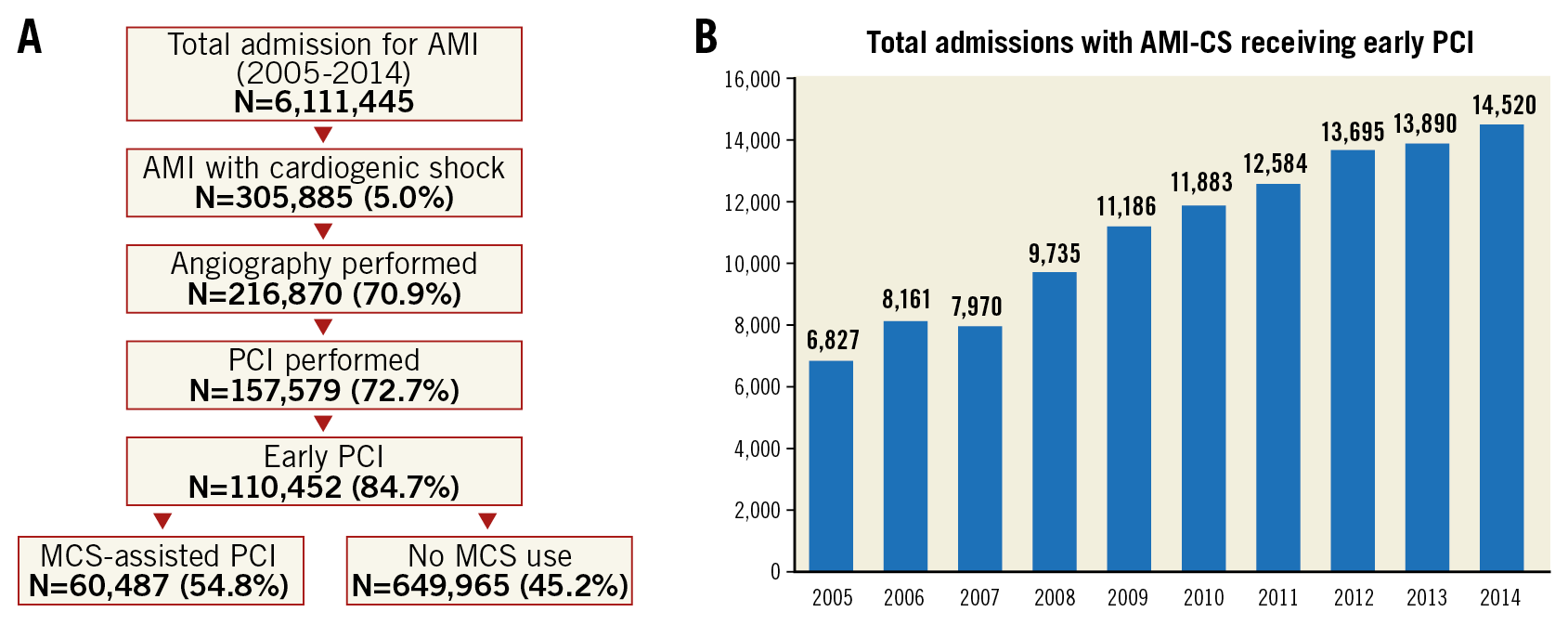
Figure 1. Study cohort. A) Consort diagram for selection of study cohort from all AMI admissions in the USA. B) 10-year temporal trends of total admissions with AMI-CS receiving early PCI (hospital day zero).
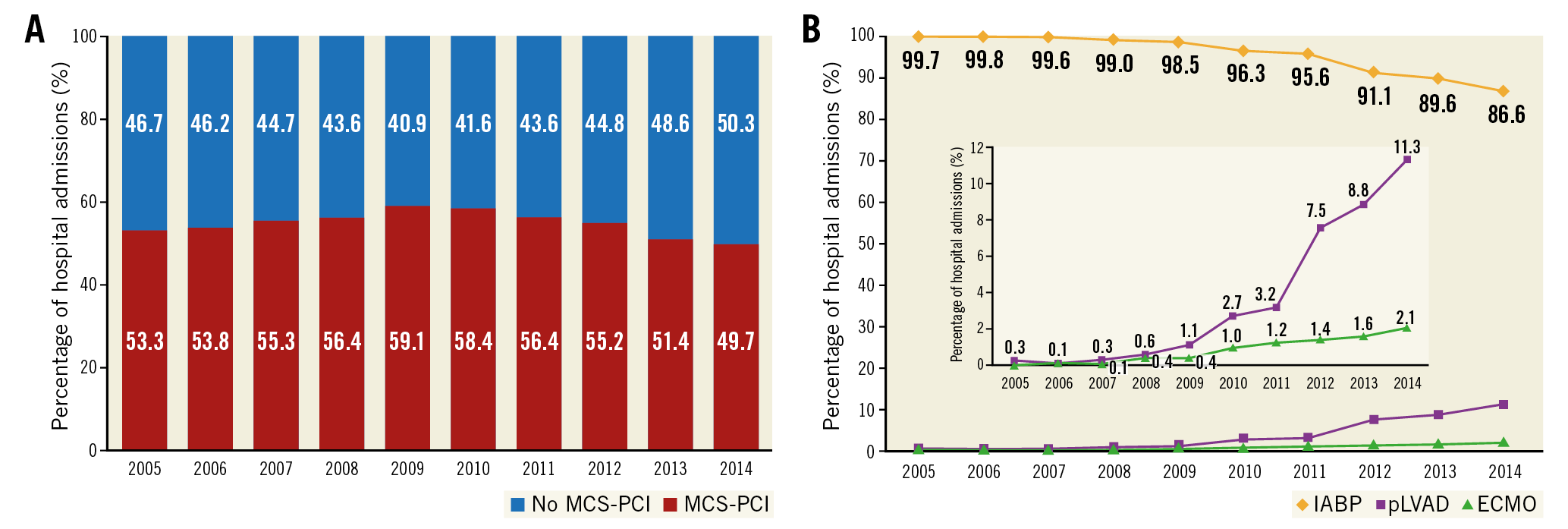
Figure 2. Temporal trends in the use of MCS assistance for early PCI in AMI-CS. A) 10-year temporal trends demonstrating the proportion of cases receiving MCS assistance for early PCI in AMI-CS. B) 10-year temporal trends of individual MCS devices for PCI assistance in AMI-CS; all p<0.001 for trend (picture-in-picture is used to provide greater magnification of pLVAD and ECMO use).
The unadjusted in-hospital mortality (31.0% vs 25.8%, OR 1.29, 95% CI: 1.26-1.33; p<0.001) was significantly higher in the cohort with MCS-assisted PCI (Figure 3A, Figure 3B for temporal trends). Use of MCS assistance for early PCI was independently predictive of higher in-hospital mortality (OR 1.23, 95% CI: 1.19-1.27; p<0.001) (Supplementary Table 3). Other significant predictors of in-hospital mortality included older age, earlier year of admission, and acute non-cardiac organ failure. These results remained consistent when admissions were stratified by age, sex, race, type of AMI-CS and presence of cardiac arrest (Figure 4). The MCS-assisted PCI cohort had longer length of stay and fewer discharges to home (Table 3).
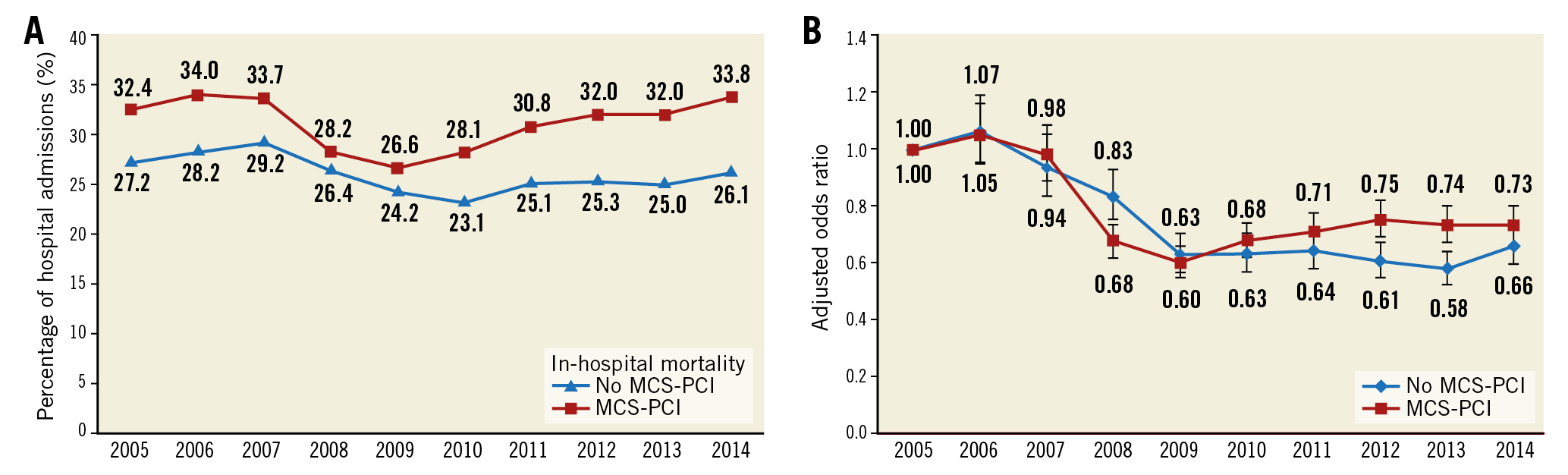
Figure 3. Temporal trends of in-hospital mortality in AMI-CS receiving early PCI. A) Unadjusted temporal trends of in-hospital mortality in AMI-CS receiving early PCI stratified by MCS use (p<0.001 for trend over time). B) Adjusted temporal trends for in-hospital mortality in AMI-CS receiving early PCI stratified by MCS use with 2000 as referent year; adjusted for age, sex, race, primary payer status, socio-economic stratum, hospital characteristics, comorbidities, AMI type, acute organ failure, cardiac arrest, invasive haemodynamic monitoring, intubation on admission, and haemodialysis use (p<0.001).
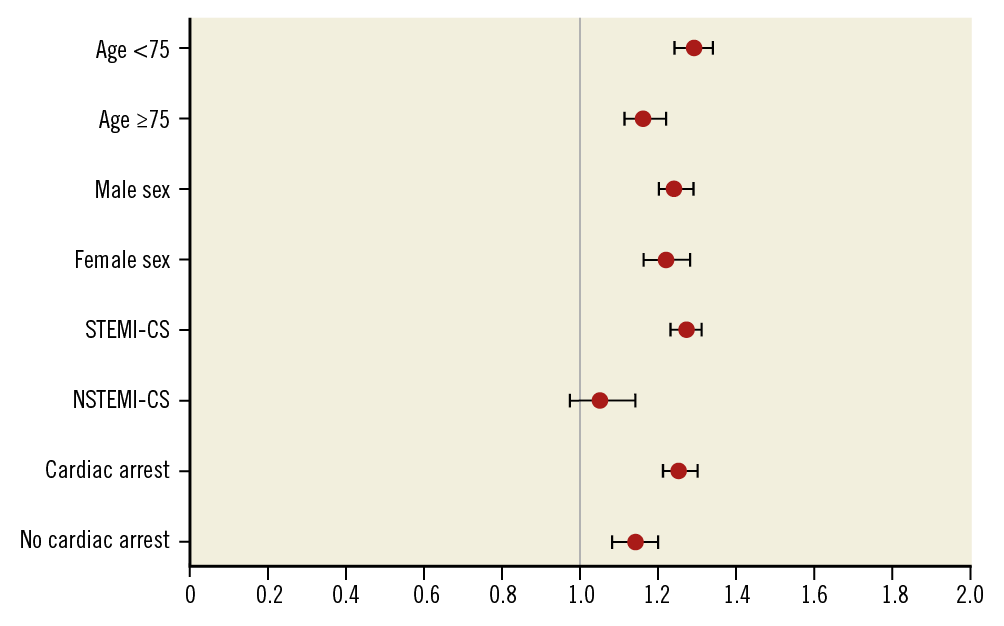
Figure 4. Multivariate predictors of in-hospital mortality in AMI-CS receiving MCS-assisted early PCI compared to those without MCS-assisted PCI. Multivariable adjusted odds ratios (95% confidence intervals)* for in-hospital mortality in the admissions receiving early PCI stratified by age, sex, race, type of AMI-CS and presence of cardiac arrest; all p<0.001. *Adjusted for age, sex, race, year of admission, primary payer, socio-economic status, hospital location/teaching status, hospital bed size, hospital region, comorbidity, type of AMI, acute organ failure, cardiac arrest, invasive haemodynamic monitoring, mechanical ventilation and haemodialysis.
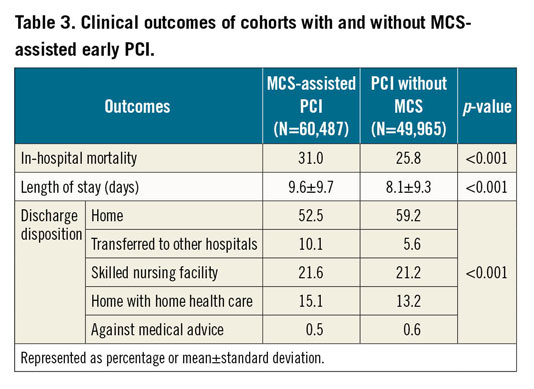
In the MCS-assisted PCI cohort, pLVAD and ECMO were used more commonly in AMI-CS with concomitant cardiac arrest and respiratory failure requiring endotracheal intubation compared to IABP (Supplementary Table 4). Unadjusted in-hospital mortality was higher in the groups with pLVAD (49% vs 30%, OR 2.25, 95% CI: 2.08-2.43; p<0.001) and ECMO (54% vs 30%, OR 2.75, 95% CI: 2.33-3.24; p<0.001) compared to the IABP cohort. In a multivariable analysis incorporating demographics, hospital characteristics, comorbidity, acute organ failure and organ support, use of pLVAD (OR 2.21, 95% CI: 2.01-2.43; p<0.001) and ECMO (OR 3.09, 95% CI: 2.53-3.76; p<0.001) for PCI assistance were associated with higher in-hospital mortality. Compared to pLVAD and ECMO, admissions with IABP were discharged home more frequently (42% vs 11% vs 53%; p<0.001) and with a shorter length of stay (9.6±10.4 vs 16.7±22.5 vs 9.5±9.4 days; p<0.001).
Discussion
In this nationally representative study of 110,452 patient admissions with AMI-CS who underwent early PCI (day of admission), we noted MCS use in 55% of the admissions. The IABP remained the most commonly used MCS device with a decrease in utilisation between 2009 (98.5%) and 2014 (86.6%). Between 2009 and 2014, though there was a concomitant increase in the use of pLVAD (1.1% to 11.3%) and ECMO (0.4% to 2.1%), the overall trend for MCS-assisted PCI showed a decrease from 2009 (59.1% to 49.7%). Younger age, male sex, non-white race, lower comorbidity, concomitant cardiac arrest and endotracheal intubation were significant predictors of MCS use. The MCS-assisted PCI cohort was sicker and had higher in-hospital mortality and greater resource utilisation compared to AMI-CS patients receiving early PCI without MCS use. Despite the higher uptake in pLVAD and ECMO devices to support PCI, there has not been a significant decrease in in-hospital mortality in AMI-CS admissions.
MECHANICAL CIRCULATORY SUPPORT IN AMI-CS
Prior analyses on AMI-CS and MCS using large databases have focused on unselected MCS use, unselected CS patients and MCS-assisted PCI in all-comers14,25,26. In contrast to these studies, our data address a very specific population of STEMI and NSTEMI patients with CS who were treated with emergent PCI within the first 24 hours. These patients are typically sicker than unselected AMI-CS patients and therefore may benefit the most from MCS implantation. As noted in this study and by other groups, there has been a steady increase in the use of percutaneous MCS devices in the catheterisation laboratory for the management of AMI-CS5,9,10,14,27. The IABP has been the traditional device of choice in AMI-CS, with more recent data demonstrating an increase in the use of pLVAD and ECMO27. In AMI-CS patients, compared to the IABP, the Impella® device (Abiomed, Danvers, MA, USA) has not shown a significant outcome benefit despite improved haemodynamic stabilisation28. Contrary to these studies, we noted higher in-hospital mortality in the pLVAD and ECMO cohorts as compared to the IABP cohort. Potential explanations for this higher mortality include (i) higher acuity of illness in the pLVAD cohort, that could not be measured holistically due to lack of physiological data, (ii) confounding by indication in this real-world population and (iii) variability in the use of these devices since the study period was before societal guidelines on percutaneous MCS13, and (iv) higher number of post-cardiac arrest patients in the MCS group who may not benefit from MCS if they have catastrophic neurologic injury. These results are consistent with prior retrospective analyses in patients with unselected CS that have demonstrated higher mortality in patients with pLVAD use and are worthy of further study in carefully designed prospective trials5,9,10,14,27. The widespread adoption of these devices may be associated with “indication creep”, wherein these devices are used in younger and less sick patients who are least likely to benefit from them. These patients may benefit from the adoption of a multidisciplinary team approach for careful patient, procedure and treatment selection4,5,17,29,30,31. Further strategies targeting aspects such as multidisciplinary care, standardised protocols, and prevention of metabolic injury and complications remain priorities in this field4,17,29,32.
TRENDS IN THE USE OF MECHANICAL CIRCULATORY SUPPORT
Traditionally, the IABP has been used for left ventricular support during PCI in AMI-CS; however, there has been a trend towards decreasing use in recent years5,9,10,14,27. Despite the lack of a demonstrable mortality benefit from the IABP in AMI-CS, >85% of the population in this study received an IABP for MCS-assisted PCI11. Around the year 2009, there was an increase in use of pLVAD and ECMO, with a significant increase around 2012. This could be postulated to be due to the influence of two important studies, i.e., the IABP-SHOCK (Intraaortic Balloon Pump in Cardiogenic Shock) and PROTECT II (Prospective, multicenter, randomized controlled trial of the Impella Recover LP 2.5 system versus IABP in patients undergoing non-emergent high risk PCI) trials that were published in 201211,12. Furthermore, we demonstrated female sex and non-white race to be associated with lower use of MCS-assisted early PCI and that these had higher in-hospital mortality. These sex and race disparities have been noted in prior studies in a different population of acute cardiac care patients and are worthy of careful assessment in AMI-CS patients17. Hospital-level disparities exist in the outcomes of AMI-CS patients receiving MCS1. Prior work from our group has shown larger hospitals to have lower in-hospital mortality in AMI-CS; however, the mortality is higher in those receiving MCS1,9,10. This can be postulated to be due to the higher acuity of this population not fully accounted for by various regression analyses. Prior literature has shown a volume-outcome relationship in unselected CS patients that has resulted in an advocacy for multidisciplinary care in specialised shock centres33. Due to the sampling design changes to the HCUP-NIS database in 2012, this study was unable to assess the relationship of hospital volume with outcomes in these patients. However, using hospital location and size as a surrogate for case volume and presence of multidisciplinary teams, we were unable to demonstrate differences in in-hospital mortality.
Limitations
This study has several limitations, some of which are inherent to the analysis of a large administrative database. The definition of CS was based on discharge diagnoses and not haemodynamic parameters. However, prior validation studies have shown high specificity (99%) and negative predictive value (98%) for this definition34. Furthermore, the definitions used for AMI and organ failure have been validated previously, which may decrease the inherent issues associated with the use of administrative codes4,16. Since further granularity in timing beyond day of procedure is unavailable, and AMI-CS evolves dynamically during the first 24 hours, it is possible that this study included patients who received MCS for cardiac arrest, worsening CS or post-PCI complications independent of the need for supporting the index PCI. Information on vasoactive medication use and dosing, laboratory parameters (peak serum lactate, serum creatinine, haemoglobin, bicarbonate, acid-base balance, etc.), left ventricular function, and haemodynamic variables known to influence outcomes in this population, were unavailable in the HCUP-NIS database. Therefore, the multivariable analyses performed in this study are unable to account for these important parameters. The timing and duration of CS, which are known to influence mortality, could not be reliably measured from this database8. However, by restricting our outcomes to early PCI, we are optimistic that most patients in either cohort presented with CS at admission. Angiographic data, such as target vessel for PCI, classification and the presence of multivessel disease with/without chronic total occlusions, that may significantly influence outcomes, were not available in this database. Despite these limitations, this study addresses an important knowledge gap, highlighting the national use of MCS to assist PCI in AMI-CS.
Conclusions
In this study of 110,452 admissions with AMI-CS that underwent early PCI, we noted that more than half the population received concomitant MCS. Though the IABP remains the most commonly used device, there has been a steady increase in the use of pLVAD and ECMO in recent years. The use of MCS identified a sicker cohort of AMI-CS patients. The cohorts with pLVAD and ECMO use had higher in-hospital mortality and resource utilisation compared to the IABP cohort, highlighting the need for further careful study in dedicated prospective studies.
|
Impact on daily practice Mechanical circulatory support-assisted percutaneous coronary intervention in acute myocardial infarction with cardiogenic shock identified a sicker population with higher in-hospital mortality. Careful selection of patients and procedures is needed to improve outcomes in this critically ill population. |
Appendix. Study collaborators
John F. Bresnahan, MD; Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, USA. Guy S. Reeder, MD; Department of Cardiovascular Medicine, Mayo Clinic, Rochester, MN, USA.
Conflict of interest statement
The authors/study collaborators have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.