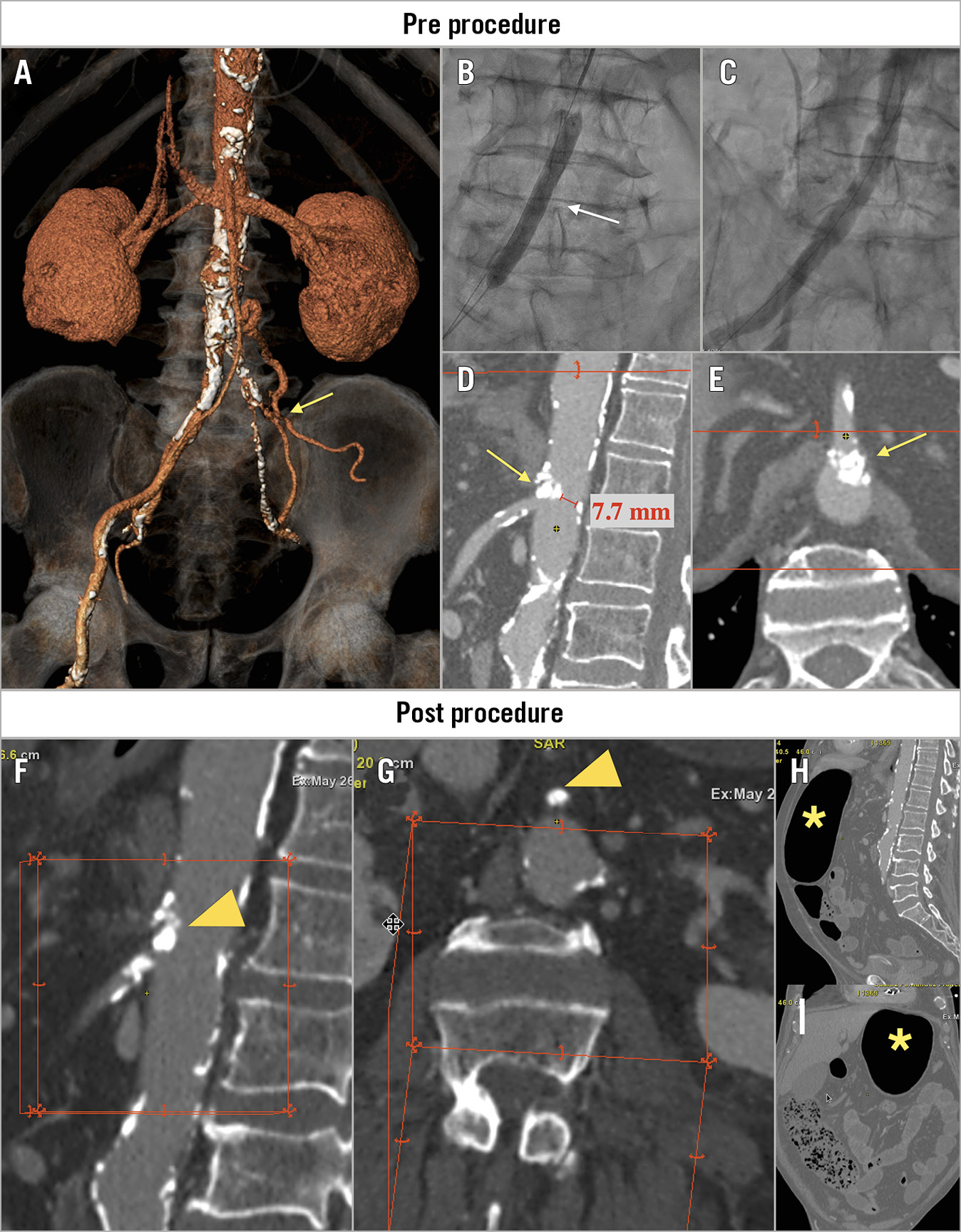
Figure 1. Pre- and post-procedure imaging. A) 3D-CT showing severe and extensive calcification of the descending aorta, iliac and femoral arteries along with a chronic common left iliac artery occlusion (yellow arrow). B) Intravascular lithotripsy (IVL) of the right iliac artery (white arrow). C) Iliac angiography post IVL. D) & E) Pre-procedure CT showing a calcified nodule at the origin of the superior mesenteric artery (SMA) without flow compromise (yellow arrows). F) & G) Occlusion of the SMA due to an eruptive calcified nodule protruding into the lumen (yellow arrowheads). H) & I) Abdominal CT showing a large gastric bubble and distended transverse colon loops (yellow asterisks).
Acute mesenteric ischaemia (AMI) is an uncommon but life-threatening medical condition associated with an ominous prognosis1. Data on this dramatic complication following transcatheter aortic valve replacement (TAVR) are currently limited to isolated case reports2,3. The overall incidence, characteristics and consequences of total occlusion of AMI after TAVR remain unknown.
An 82-year-old man with hypertension, diabetes mellitus, hyperlipidaemia, severe chronic obstructive pulmonary disease, extensive peripheral artery disease and severe aortic stenosis (aortic valve area 0.82 cm2) presented with mild effort dyspnoea (New York Heart Association [NYHA] functional Class III). The patient was deemed to be a candidate for TAVR because of severe comorbidities (Society of Thoracic Surgeons [STS] score 6%).
Although alternative access was assessed, the TAVR procedure was performed through the right transfemoral approach. Preprocedural computed tomography (CT) revealed a chronic common left iliac artery occlusion (Figure 1A, Moving image 1) with severe and extensive non-circumferential calcification of right femoral and iliac arteries (minimal lumen diameter of 4.6 and 5 mm, respectively). Elective intravascular lithotripsy (IVL) using a 7 mm balloon (Shockwave Medical, Santa Clara, CA, USA) was performed to facilitate the sheath insertion (Figure 1B, Figure 1C). After overcoming some difficulties in advancing the sheath and delivery system through the iliac artery (Moving image 2), an Evolut™ PRO 26 mm valve (Medtronic, Minneapolis, MN, USA) was successfully implanted (Moving image 3).
A few hours after the procedure, the patient developed progressive abdominal pain, nausea and vomiting along with vagally mediated conduction disturbances leading to temporary pacemaker implantation. Emergent abdominal CT angiography revealed an occlusion of the superior mesenteric artery (SMA) due to an eruptive calcified nodule protruding into the lumen. Of note, this calcified nodule was previously identified in the preprocedural CT, at the origin of the SMA, but without any flow compromise (pre procedure: Figure 1D, Figure 1E; post procedure: Figure 1F, Figure 1G). Also, the CT disclosed a huge gastric bubble and distended transverse colon loops with thinning and abnormal enhancement of the bowel wall (Figure 1H, Figure 1I). The patient was referred to surgery and exploratory laparotomy exhibited an ischaemic and dilated ascending and transverse colon without findings of perforation. The ischaemic segment was completely resected leading to a right hemicolectomy and end-ileostomy. Despite early surgery, the patient suffered progressive clinical worsening, developing a multiple organ dysfunction syndrome and died three days after the TAVR procedure.
To the best of our knowledge, this is the first case report describing an acute occlusion of the ostium of the SMA in direct relation to a TAVR procedure. This case highlights the importance of a comprehensive assessment of the access route, considering alternative approaches to transfemoral (including transcarotid, trans-subclavian and transcaval) during the preprocedural planning to minimise the risk of major vascular complications.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Iliofemoral angiography (pre IVL).
Moving image 2. Fluoroscopy showing the passage of the delivery system through the right iliac artery.
Moving image 3. Iliofemoral angiography (post procedure).