Abstract
Aims: A manageable and reproducible large animal model of human-like coronary atherosclerosis is lacking but highly needed for translational research in percutaneous coronary interventions and imaging. Farm pigs with familial hypercholesterolaemia develop advanced atherosclerosis in two to three years but then weigh >200 kg making them impractical and costly. We aimed at down-sizing this pig and accelerating coronary plaque development to make the model more useful and affordable.
Methods and results: Familial hypercholesterolaemic farm pigs were downsized by crossing them with smaller pigs while preserving their hypercholesterolaemic trait ascribed to a mutation in the low density lipoprotein receptor. We accelerated coronary plaque development by atherogenic diet feeding whereby plasma total cholesterol rose to >20 mmol/l (>800 mg/dl). We further accelerated coronary plaque development site-specifically by inflicting coronary artery balloon injury. Both spontaneously developed and balloon accelerated coronary plaques mirrored pertinent human plaque features, including a large necrotic core covered by a thin and inflamed fibrous cap as seen in the most common type of thrombosis-prone (vulnerable) plaque in humans. Associated vulnerable plaque features included neovascularisation, intraplaque haemorrhage, and expansive remodelling.
Conclusions: This human-like porcine model of coronary atherosclerosis is practical and highly relevant for translational research in percutaneous coronary interventions and imaging.
Introduction
Large pigs with spontaneous atherosclerosis were identified more than 20 years ago by Rapacz and co-workers1. Although the model seemed promising2,3, it has not been widely used because of the long time taken to develop advanced lesions (>2 years), unsuitable body weight (>200 kg), and consequential prohibitive costs.
Therefore, the preclinical testing of coronary stents has mainly relied on the response obtained in normal coronary arteries of young, normocholesterolaemic pigs or peripheral arteries of hypercholesterolaemic rabbits. But the healing response of diseased arteries under hypercholesterolaemic conditions most likely differ from that of normal arteries and may even be delayed or absent around stent struts placed in the necrotic cores of atherosclerotic plaques4,5, and also peripheral arteries may respond and heal differently than coronary arteries6. So current models can merely demonstrate limited safety features and therefore, an animal model with coronary plaques containing necrotic cores would be highly relevant for preclinical testing of stents. Additionally, a downsized model would allow longer-term safety studies in outgrown arteries with stable dimensions. Such a model would also be useful for preclinical evaluation of emerging coronary imaging technologies7.
To meet the need for a manageable and reproducible large animal model of human-like coronary atherosclerosis, we have downsized the original Rapacz farm pig and accelerated the development of atherosclerosis by an atherogenic diet and localised balloon injury. This model expresses the morphological features of the most common high-risk (vulnerable) plaque seen in human coronary artery disease, the so-called thin-cap fibroatheroma (TCFA), including a relatively large necrotic core, a thin and inflamed fibrous cap, neovascularisation, plaque haemorrhage, and microcalcifications.
Methods
This study was approved by the Danish Animal Experiments Inspectorate.
Downsizing
Downsized pigs homozygous for the R84C low density lipoprotein (LDL) receptor mutation8 were produced by crossing the Rapacz farm pig first with a smaller pig (Chinese Meishan) and then crossing the offspring with an even smaller minipig from Bretoncelles, France. Genotype was confirmed by genotypic testing throughout the breeding process. The Rapacz farm pig has been called FHC for familial hypercholesterolaemia3 and also FH-r, referring to the recessive mode of inheritance of the hypercholesterolaemic trait. We have named the downsized pig FBM, F for familial hypercholesterolaemia, B for Bretoncelles, and M for Meishan. The FBM pigs breed like normal pigs.
Pigs and diets
Ten male castrated pigs (mean age nine months) were fed standard minipig diet (Special Diets Services), and baseline blood samples were drawn. The pigs were then semi-restrictedly fed an atherogenic diet for 18 weeks after which post mortem examination was performed (Figure 1). The pigs were weighed regularly during the study.
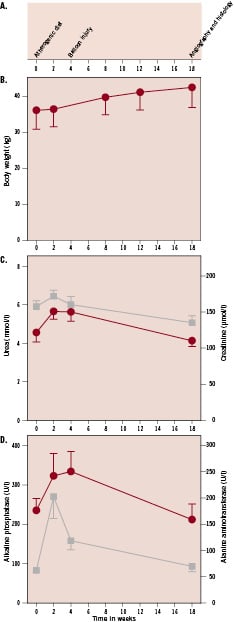
Figure 1. Study design, body weights, and kidney and liver function parameters. A: study design outline for atherogenic diet and balloon injury. B: body weights. C: urea (circles) and creatinine (squares). D: alkaline phosphatase (circles) and alanine amino transferase (squares). Values are mean±SEM.
The atherogenic diet (583V, TestDiet®; Division of Land O’Lakes Purina Feed, LLC , Richmond, IN, USA) contained 2% cholesterol, 20% lard and 1.5% cholate (w/w). To assess the effect of cholate in this diet, three pigs were fed cholate-free diet during the last five weeks of the study, consisting of standard minipig diet (Special Diets Services) added 2% cholesterol and 20% lard.
Plasma analyses
Blood samples were drawn in EDTA containing tubes at baseline and after two weeks, four weeks, and 18 weeks on the atherogenic diet. Total and free cholesterol and triglycerides were analysed with enzymatic methods. Fixed density ultracentrifugation of 1 ml plasma in 5.5 ml ultracentrifugation tubes were performed at 10C after adjusting the density to 1.019 g/ml or 1.063 g/ml with NaBr as previously described9. Notably, upon ultracentrifugation, the d<1.063 g/ml fractions contained unclear aggregated material which floated in the middle of the ultracentrifugation tube. We have not previously seen such aggregates in analyses of even more severely hyperlipidaemic plasma from cholesterol-fed rabbits and apolipoprotein E or LDL-receptor deficient mice. The aggregates, however, could be cleared by the addition of 1% triton X-100 prior to cholesterol measurements and the recovery of cholesterol after ultracentrifugation was >90%. Plasma lipoproteins were separated according to size using size-exclusion chromatography with a Superose 6B column10 (GE Healthcare Ltd, Little Chalfont, Buckinghamshire, UK). Plasma was diluted with PBS and passed through a 0.22 µm filter prior to loading on the column. To visualise apolipoprotein B, aliquots of the d<1.063 g/ml fractions and isolated human LDL were separated in 3-20% SDS page gels under denaturing conditions and proteins were silver-stained using reagents from Sigma (Sigma-Aldrich Corp., St. Louis, MO, USA).
Plasma alkaline phosphatase, aspartate aminotransferase, urea, and creatinine were measured with routine methods to detect potential harmful effects of the atherogenic diet, such as liver and kidney toxicity. Plasma glucose was measured with a Modular Autoanalyzer and reagents from Roche, Copenhagen, Denmark.
Balloon injury
Coronary artery guiding catheters were introduced through an arterial sheath inserted in the left carotid artery, and under fluoroscopic guidance over dilation of the middle segment of the right coronary artery (RCA, n=10) was performed. Likewise in the left coronary artery (LCA, n=10), balloon injury was performed in the middle segment of either the circumflex coronary artery (LCX) or the left anterior descending coronary artery (LAD). To assess the natural history of atherosclerosis development in these middle coronary artery segments, either the LAD or LCX was left uninjured and thereby served as balloon injury site control. We aimed at 50% over dilation once for 30 seconds using standard 3.5 or 4.0 mm angioplasty balloons at pressures of 8-12 atmospheres.
Angiography was performed before and after balloon inflation and repeated at the end of the study and the diameters of the balloon injured sites were measured before and after balloon injury and at the end of the study as described previously11. Also the diameter of the inflated balloon was measured. Acute diameter gain was defined as percentage increase in luminal diameter of the injury site from before to after balloon injury. Late diameter loss was defined as percentage decrease in luminal diameter of the injury site compared to a proximal reference.
Coronary pathology
The hearts were excised, and the coronary arteries were perfusion fixed with 4% formaldehyde at 100 mmHg for one hour and subsequently immersion fixed for 6-12 hours. The coronary arteries were sectioned at 4 mm intervals, paraffin embedded, sectioned (4 µm sections), and stained for microscopic examination. Haematoxylin and eosin (HE), trichrome-elastin (connective tissue including elastin), picrosirius red (collagen) and von Kossa staining (calcification) were used in the analyses. To support interpretations based on these staining methods, immunohistochemistry for smooth muscle cells (anti-smooth muscle actin, Dako M0851) and macrophages (anti-lysozyme12, Dako A0099), and special staining for endothelium (biotinylated Griffonia simplicifolia lectin I, Vector Laboratories B-1105) were performed on selected sections. The balloon injured segments were identified as segments with complete rupture of the internal elastic lamina extending through media.
The luminal area and the areas within the internal elastic lamina (IEL) and external elastic lamina (EEL) were measured on digital photomicrographs (ImageJ, NIH) and absolute intimal area and intima to media and intima to IEL area ratios were calculated for each section, and each lesion was graded according to a morphological classification scheme focusing on the necrotic core and the fibrous cap (for details please see online appendix, Table 1). Within each coronary segment of interest, results from the lesion with the largest cross-sectional area are presented here. The term «atheromatous plaque» is used for a plaque containing a necrotic core, consisting of dead cells and cellular debris (no or fragmented nuclei by HE staining) and degraded extracellular matrix (no preserved collagen by picrosirius red staining); cholesterol crystals were not required to define a necrotic core because they are relatively rare in porcine lesions13-15. Necrotic core size and thickness of the thinnest part of the fibrous cap covering the core were measured on low magnification digital photomicrographs of picrosirius red stained sections. Medial destruction was recorded in spontaneously developed lesions but not in balloon-accelerated lesions since medial disruption was required to identify the location of these lesions.
Results
One pig died during follow-up in relation to blood sampling. Consequently, nine pigs were available for final evaluation.
Body weight
The pigs thrived and showed only a steady low incline in body weight during the study, and at the end of the study, all but one pig (84 kg) had body weights between 30 and 50 kg. The urea and creatinine were not affected by the feeding protocol, whereas there was a modest and transient increase in plasma concentrations of liver enzymes after 2-4 weeks (Figure 1).
Plasma lipids, lipoproteins, and glucose
On standard diet at baseline (week 0), the plasma total cholesterol levels were ~2-fold higher than in farm pigs and other minipig strains (Figure 2A). After 2 weeks on the atherogenic diet, the total cholesterol and triglyceride levels had increased, ~4- and ~2-fold respectively (Figure 2A and 2B). Subsequently, there was a gradual decline of both total cholesterol and triglycerides until the termination of the study (Figure 2A and 2B). In the three pigs receiving the diet lacking cholate for the last four weeks, the changes in total cholesterol were similar to those in the six pigs continuing on the atherogenic diet. Ultracentrifugation analyses of plasma lipoproteins showed that HDL cholesterol had risen in proportion with total cholesterol after two weeks and then remained unchanged until the end of the study (Figure 2A). VLDL and LDL cholesterol concentrations increased markedly in response to the atherogenic diet and remained elevated over the basal levels throughout the study despite a gradual decline from two to 18 weeks (Figure 2A). Size-fractionation of plasma showed a marked increase of the concentration of cholesterol mainly in VLDL-sized lipoproteins in response to the atherogenic diet (Figure 2C). Thus, the atherogenic diet induced plasma accumulation of lipoproteins with LDL-density that are larger than human LDL particles. The rise of VLDL and LDL cholesterol was accompanied by increased apolipoprotein B 100 concentrations as judged by gel electrophoresis analyses of the VLDL+LDL ultracentrifugation fractions (Figure 2D).
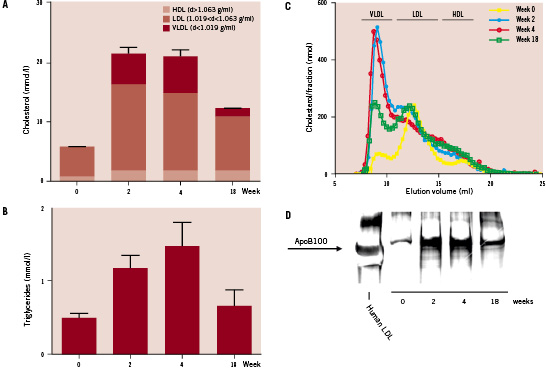
Figure 2. Plasma lipoproteins in downsized pigs fed an atherogenic diet. A, plasma total, HDL, LDL, and VLDL cholesterol determined after separation of lipoproteins with fixed density ultracentrifugation. B, plasma total triglycerides. C, plasma lipoproteins separated by size-exclusion chromatography on a Superose 6B column. The indicated elution volumes of VLDL, LDL, and HDL were determined with isolated human lipoproteins. D, the d<1.063 g/ml (VLDL+LDL) plasma fractions were pooled at each time point and an aliquot from each pool was separated in a 4-20% polyacrylamide gel in the presence of SDS under reducing conditions. Isolated human LDL was included as a control. Proteins were visualised by silverstaining. The identity of the apoB100 bands was ascertained by western blotting analyses using a polyclonal anti-human apoB antibody which reacted with porcine apoB (data not shown). Error bars represent SEM.
Mean plasma glucose concentration at termination was 4.1mmol/l (1.3 mmol/l). Post mortem microscopic examination of HE stained livers from all pigs were normal.
Coronary balloon injury
Assessed angiographically, the median inflated balloon diameters were 61% and 64% above the coronary artery diameters in the RCA and LCA, respectively. The median acute diameter gain from balloon injuries were 46% and 51% and the median late diameter losses were 12% and 18% in the RCA and LCA, respectively.
Coronary lesions
Outside the balloon injured areas, the largest and most advanced spontaneously developed lesions were invariably found in the proximal segments of the coronary arteries. These proximal lesions were almost always clearly separated from the balloon-injured sites by a segment with normal intima or intimal xanthoma only.
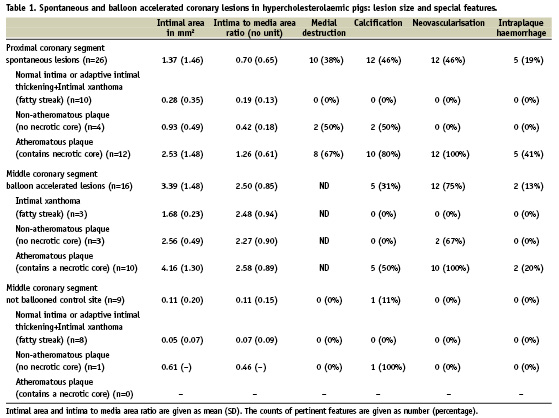
Pertinent features of spontaneously developed lesions in proximal segments, balloon accelerated lesions middle segments, and control site lesions were recorded. The lesion features are given in Table 1 and 2 and in online appendix Table 2.
Both spontaneous and balloon accelerated atheromatous plaques contained numerous macrophage foam cells but compared to human plaque the necrotic cores contained few cholesterol crystals. Despite relatively large plaque areas there were no significant angiographic stenoses, indicating that the plaques were associated with expansive remodelling. The calcification pattern of the atheromatous plaque was typically characterised by foci of calcifications in the necrotic cores towards the plaque base (Figures 3 and 4). Dense calcifications were also found in the fibrous tissue outside the necrotic core of atheromatous plaque while two non-atheromatous plaques had similar calcifications.
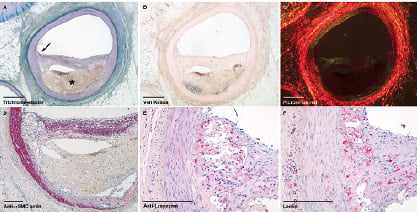
Figure 3. Spontaneously developed atheromatous plaque in the left circumflex branch of a downsized hypercholesterolaemic pig. A, overview of trichrome-elastin stain. The necrotic core is marked with asterisk, and the fibrous cap shoulder region with local thinning and inflammation is marked with arrow. There is haemorrhage within the necrotic core. B, von Kossa stain (calcifications black). C, picrosirius red stain viewed under polarised light demonstrates lack of collagen in the necrotic core. D, immunohistochemical stain for smooth muscle cells demonstrates local thinning and decreased smooth muscle cell content at the shoulder region of the fibrous cap. E, immunohistochemical stain for macrophages demonstrates macrophage infiltration of the fibrous cap at the shoulder region. F, lectin stain demonstrates neovascularisation but also stains macrophages and erythrocyte membranes. Scale bars are 1 mm in panels A, B and C and 250 μm in panels D, E and F.
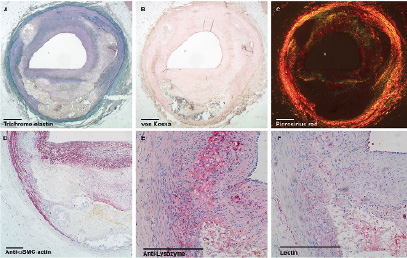
Figure 4. Balloon accelerated atheromatous plaque in the right coronary artery of a downsized hypercholesterolaemic pig. A, overview of trichrome-elastin stain shows haemorrhage within the necrotic core. B, von Kossa stain (calcifications black). C, picrosirius red stain viewed under polarised light demonstrates lack of collagen in the necrotic cores. D, immunohistochemical stain for smooth muscle cells. E, immunohistochemical stain for macrophages demonstrates macrophage infiltration of the fibrous cap. F, lectin stain demonstrates neovascularisation but also stains macrophages and erythrocyte membranes. Scale bars are 1 mm in panels A, B and C and 250 μm in panels D, E and F.
There was no statistical correlation between age, total cholesterol, HDL-cholesterol, or the ratio of total cholesterol to HDL-cholesterol and lesion size or type. However, this data set is too small to prove or dismiss such correlations.
Spontaneous versus balloon accelerated lesions
Spontaneously developed plaques were typically eccentric (Figure 3), in contrast to balloon accelerated lesions that typically were concentric. The balloon accelerated lesions were characterised by neointimal fibrotic (scar) tissue virtually void of foam cells covering the site of medial disruption while the necrotic cores, if present, were situated over an intact IEL (Figure 4).
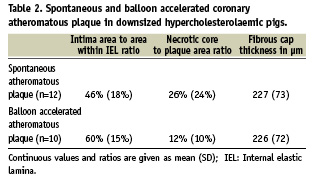
Morphometric data and characteristics of the spontaneous and balloon accelerated atheromatous plaques are compared in Table 1 and 2. The balloon accelerated atheromatous plaques were larger than the spontaneously developed lesions and had larger intima to media and intima to IEL area ratios. Both spontaneous and balloon accelerated atheromatous plaques showed neovascularisation but intraplaque haemorrhages and calcifications were more frequent in spontaneous atheromatous plaques. Also, the spontaneous atheromatous plaques also had relatively larger necrotic cores whereas fibrous cap thicknesses were equal.
Discussion
We generated a minipig with familial hypercholesterolaemia caused by a natural mutation in the LDL receptor. The mutation was originally identified in large farm pigs8 with spontaneous atherosclerosis2,3, and we downsized this pig to a more suitable size while maintaining the propensity for hypercholesterolaemia and coronary atherosclerosis. Prior to this study, the response to atherogenic diet and balloon injury has never been described in the porcine familial hypercholesterolaemia model.
Cholesterol and lesion acceleration
Pigs with normal cholesterol metabolism do not develop hypercholesterolaemia and hence do not develop atherosclerosis2,3, and although some pig strains may develop moderate hypercholesterolaemia and atherosclerosis when fed atherogenic diets, it takes a long time to develop advanced lesions making the models time-consuming and costly16. The effects of an atherogenic diet on the lipid profile and the atherosclerosis development in the LDL receptor mutated pig have never been reported before.
On a regular diet, the FBM pigs had moderately elevated plasma cholesterol levels and the atherogenic diet caused further plasma accumulation of LDL and VLDL-sized, apoB100-containing lipoproteins. The pigs were nine months old when they were put on the atherogenic diet, and we found spontaneously developed coronary atherosclerotic lesions after only 18 weeks on the atherogenic diet. The original Rapacz farm pigs developed similar lesions, however such lesions were only observed in pigs more than two years of age2,3. Hence, the atherogenic diet appears to accelerate the development of advanced atherosclerosis markedly. However, atherogenic diets are expensive, and it is advantageous that downsized pigs require a smaller daily intake allowing more affordable experiments. Notably, we did not observe adverse effects consequential to the atherogenic diet in the pigs.
Localised acceleration of atherosclerosis
Angioplasty balloon injury is well-described in pigs with normal cholesterol levels, where injuries heal with fibrosis and without necrotic core formation11. However, coronary balloon injury has never before been reported in the LDL-receptor mutated pig.
At the end of this study, the middle coronary artery control segments contained no atheromatous plaques. So like in humans, middle coronary segments were less atherosclerosis prone than proximal coronary segments in this model (Table 1 and 2). But after inflicting balloon injury, we observed a much higher atheromatous plaque frequency than in the control middle coronary segments only 14 weeks after balloon injury. Besides the medial damage and fibrotic scar induced by balloon injury, the balloon accelerated atheromatous plaque very much resembled the observed spontaneous atheromatous plaque (Table 1 and 2). Thus, adding balloon injury resulted in the same plaque components relevant to human disease and additionally, placing the balloon injuries outside locations where spontaneous lesions are frequently observed increases the total number of atheromatous plaques available in the model.
Relation to other atherosclerosis models
A combined hypercholesterolaemia and chemically induced diabetes model of coronary atherosclerosis in large pigs17 has been used for studies on gene expression and preclinical evaluation of medical therapy18,19. Although the results are interesting, it is hard to elucidate the correlation between gene expression and atherosclerosis and the effect of the therapy without the impact of diabetes. As well as it is advantageous to have a model that may predict the impact of diabetes, it is advantageous to have a model where the development of coronary atherosclerosis is not dependent on the presence of diabetes. In addition, with the present protocol we observed spontaneous atheromatous plaques as frequently as reported after up to nine months of combined diabetes and hypercholesterolaemia18,20,21.
We observed intraplaque haemorrhages, which was also recognised in the original LDL-receptor mutated farm pig2,3. This is not commonly seen in other animal models of atherosclerosis which is unfortunate since intraplaque haemorrhages may be a key mechanism in coronary plaque progression14. This model may thereby also be useful in the study of this proposed plaque progression mechanism.
A translational model
The downsized pigs are large enough for the coronary arteries to be engaged with imaging equipment without being too large to handle easily in the lab. Additionally, these downsized pig maintain relatively stable dimensions (Figure 1) allowing longer-term safety studies, e.g., stable dimensions reduces the risk of the coronary arteries outgrowing implanted stents.
Some of the spontaneously developed and balloon accelerated atheromatous plaques resembled human plaques assumed to be rupture-prone (TCFA) with necrotic core, thin and inflamed fibrous cap, neovascularisation, intraplaque haemorrhages, expansive remodelling and calcifications (Figure 3). Comparing the features of these porcine atheromatous plaques to those of human plaques classified as rupture-prone, the percentage of plaque occupied by necrotic core was 26% in the spontaneous atheromatous plaques versus 23% in human TCFA22. However, we have yet to find unequivocal evidence of plaque rupture in this short-term experimental model and therefore refrain from describing the observed atheromatous plaque as vulnerable plaque23. However, since both spontaneous and balloon accelerated atheromatous plaques harbour necrotic core, inflammation, expansive remodelling, calcifications, neovascularisation and intraplaque haemorrhage that are all characteristics of human vulnerable plaques24, both are useful for testing of emerging strategies aimed at detection and/or treatment of vulnerable plaques. In certain situations, the possibility of choosing the lesion site at will by balloon injury is particularly attractive.
Until now, experimental studies on coronary stenting have focused mainly on neointima formation induced in normal pig coronary arteries. In contrast, stents are employed on top of atherosclerotic plaques in humans. With the lack of a useful large animal model, the consequences of stent strut placement in a necrotic core have not been studied experimentally. In this model, both the spontaneous and balloon accelerated atheromatous plaques could be useful for such experimental studies of necrotic core versus fibrotic tissue stent strut response. And with balloon injury added to atherogenic diet, the frequency of lesions with necrotic cores was high, which makes this model relatively cost-effective for such studies.
Conclusions
We generated a downsized pig with defective LDL receptor. The plasma cholesterol levels were elevated on normal feed and severely elevated on an atherogenic diet. From nine months of age, spontaneously developed coronary atheromatous plaques were seen after 18 weeks on atherogenic diet and at balloon injury sites after only 14 weeks. The balloon accelerated plaques shared characteristics with the spontaneous plaques and adds to the total number of plaques in this model. Some of the plaques were morphologically similar to human vulnerable plaques, and the model seems promising for future preclinical testing of coronary imaging and interventional tools intended for human use.
Acknowledgements
We thank Birgitte Kildevæld Sahl, Rita Ullerup and Lisa Maria Røge for their expert technical assistance in preparation of coronary arteries for microscopic examination.
Funding sources
We are grateful for the funding provided by Aarhus University Research Foundation, The Danish Medical Research Council, and Institut de l’Atherothrombose, Paris, France.
Disclosures: None.
