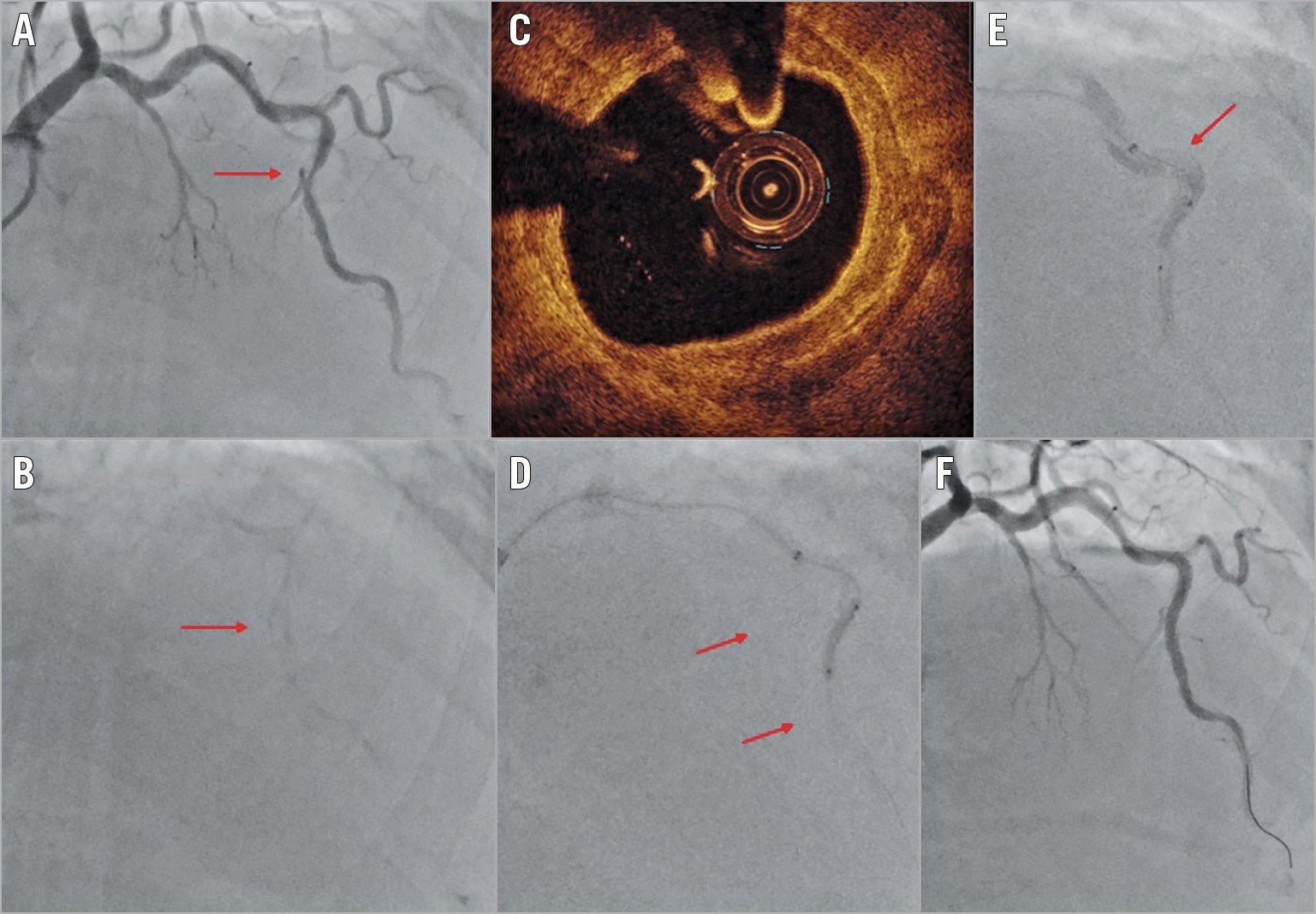
Figure 1. LAD angiography and OCT. A) & B) Basal angiograms (red arrow, heavily calcified stenosis). C) OCT 360° calcified plaque. D) Deep intubation with a GuideLiner and IVL balloon inflation (4 atm). E) IVL balloon rupture with subsequent vessel dissection. F) Final result.
Coronary calcifications represent one of the hardest challenges for interventional cardiologists. Calcifications increase difficulties related to the procedure, causing a decreased stent expansion and higher number of dissections1. Recently, numerous devices for coronary debulking have appeared on the market such as the Coronary Lithoplasty® System for intravascular lithoplasty (IVL; Shockwave Medical, Inc., Santa Clara, CA, USA) designed to disrupt both superficial and deep calcified plaque with a circumferential mechanical energy distribution2. Despite its effectiveness3, some doubts remain regarding its safety and possible procedural complications. Here we present a case of coronary dissection due to the rupture of the inflated IVL balloon.
A 47-year-old man with end-stage renal disease was referred to our cath lab with a view to renal transplant. The angiography showed single-vessel coronary artery disease with critical heavily calcified mid left anterior descending (LAD) stenosis in the context of a very tortuous anatomy not suitable for rotational atherectomy (Figure 1A, Figure 1B, Moving image 1). We decided to manage this case with percutaneous coronary intervention (PCI), using optical coherence tomography (OCT) and IVL. PCI was performed via a femoral 7 Fr catheter. After deep intubation with a 6 Fr GuideLiner® (Teleflex Medical, Wayne, PA, USA) and predilation with a 2.5×15 mm semi-compliant balloon we performed OCT (Figure 1C). OCT showed a circumferential calcific lesion; no dissections were observed (Moving image 2). Due to the length and tortuosity of the lesion, we decided to perform IVL with a 3.0×12 mm balloon at 4 atm (ratio 1:1 balloon:vessel) (Figure 1D). At the sixth second of the second delivery phase, the IVL balloon broke with subsequent dissection of the LAD (Figure 1E, Moving image 3). Finally, two everolimus-eluting stents were delivered to the mid LAD and post-dilation was performed (Figure 1F, Moving image 4).
In conclusion, calcified lesion treatment can be associated with several intraprocedural complications (balloon rupture, dissection, perforation). Balloon rupture can happen even with low pressure. The IVL balloon is not an exception. Certainly, further research is needed to understand the possibilities and limits of such an innovative and promising technique.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Basal angiography: critical heavily calcified mid LAD stenosis in the context of a very tortuous anatomy.
Moving image 4. Final result.
Moving image 2. Angiography performed during OCT acquisition. After deep intubation with a GuideLiner and predilation, no dissection was observed.
Moving image 3. Coronary Lithoplasty System balloon rupture with subsequent vessel dissection.