Abstract
Aims: Angiographic guidance for percutaneous coronary intervention (PCI) has substantial limitations. The superior spatial resolution of optical coherence tomography (OCT) could translate into meaningful clinical benefits. We aimed to compare angiographic guidance alone versus angiographic plus OCT guidance for PCI.
Methods and results: Patients undergoing PCI with angiographic plus OCT guidance (OCT group) were compared with matched patients undergoing PCI with angiographic only guidance (Angio group) within 30 days. The primary endpoint was the one-year rate of cardiac death or myocardial infarction (MI). A total of 670 patients were included, 335 in the OCT group and 335 in the Angio group. OCT disclosed adverse features requiring further interventions in 34.7%. Unadjusted analyses showed that the OCT group had a significantly lower one-year risk of cardiac death (1.2% vs. 4.5%, p=0.010), cardiac death or MI (6.6% vs. 13.0%, p=0.006), and the composite of cardiac death, MI, or repeat revascularisation (9.6% vs. 14.8%, p=0.044). Angiographic plus OCT guidance was associated with a significantly lower risk of cardiac death or MI even at extensive multivariable analysis adjusting for baseline and procedural differences between the groups (OR=0.49 [0.25-0.96], p=0.037) and at propensity-score adjusted analyses.
Conclusions: This observational study, the first ever formally to appraise OCT guidance for PCI decision-making, suggests that the use of OCT can improve clinical outcomes of patients undergoing PCI.
Introduction
Percutaneous coronary intervention (PCI) is a mainstay in the management of coronary artery disease. However, the luminological drawbacks of angiographic guidance have been established since the late 1980s and early 1990s1. Despite this awareness, intravascular ultrasound (IVUS), an invasive imaging modality with tomographic capability and higher resolution than angiography, has so far failed to offset convincingly the role of angiographic guidance during routine PCI2-9. Reasons for the uncertainty in relation to the benefit of an IVUS-guided approach to provide substantial benefits in comparison to angiography can be several, but one of the key factors might indeed be spatial resolution, as even IVUS cannot image with precision and accuracy small structures such as stent struts or subtle procedural complications10.
Optical coherence tomography (OCT) has recently been introduced in clinical practice, with further developments already available including frequency-domain (FD)-OCT and non-occlusive imaging11,12. Whereas the superiority of OCT in comparison to any other available intracoronary imaging modality in terms of spatial resolution is unchallenged, with ensuing extensive use in clinical research, there is uncertainty in its risk-benefit role in routine clinical practice in comparison to angiography or IVUS13,14.
We hypothesised that routine OCT use on top of angiographic guidance can improve mid-term clinical outcomes in comparison to angiographic guidance alone in patients undergoing PCI in the current era. Thus, the aim of the retrospective Centro per la Lotta contro l’Infarto-Optimisation of Percutaneous Coronary Intervention (CLI-OPCI) study was to compare clinical outcomes in subjects undergoing PCI with angiographic guidance alone versus angiographic plus OCT guidance.
Methods
DESIGN
This was a retrospective multicentre study based on an explicit yet pragmatic treatment protocol distributed to all interventional cardiologists working at involved centres, which was meant to make the practice uniform and to enforce similar criteria for intervention whenever OCT was performed to guide PCI. However, this protocol was operational and by no means experimental. Therefore, it did not require strict selection criteria, rigid actions, or envisage violations. In addition, OCT catheters and imaging consoles were already CE marked in Europe for invasive coronary imaging before, during or after PCI during the conduct of the study. Accordingly, ethical approval was waived in the light of the observational retrospective design. Finally, all patients provided written informed consent for the index procedure and for phone/direct visit follow-up.
PATIENTS
Consecutive patients undergoing PCI with angiographic plus OCT guidance (OCT group) at three high OCT-volume Italian centres between 2009 and 2011 were matched 1:1 with randomly selected patients undergoing PCI with angiographic only guidance within 30 days and in the same institution (Angio group).
PROCEDURES
Given the retrospective design, treatment choices, including stent type and ancillary pharmacologic therapy, were at the operator’s discretion. However, a specific and explicit interventional protocol developed on the basis of our institutional expertise with OCT11-13,15 was used for patients in the OCT group.
The use of OCT guidance for coronary angioplasty was left at the operator’s discretion, with some operators preferring either OCT guidance or angiographic guidance for most of their cases. Of note, all procedures, independently of the use of OCT, were performed by senior staff members with established skills and case-load. Indeed, it is expected that OCT may be preferred in more challenging or complex lesions, or when angiography is unlikely to provide clear guidance for interventional strategy or device selection. Conversely, it is expected that angiographic guidance is to be preferred more commonly for relatively simple lesions in unstable patients.
Specifically, PCI was performed using standard techniques via the femoral or right radial approach using 6 Fr or 7 Fr sheaths and catheters. Patients received either drug-eluting stents (DES) or bare metal stents (BMS) at the discretion of the operator. All patients were treated with 325 mg aspirin prior to PCI and loaded with 600 mg clopidogrel or 60 mg prasugrel if not already on a maintenance dose. Dual antiplatelet therapy was recommended in all patients. During PCI, patients were administered unfractionated heparin (a bolus of 70 IU/kg and additional doses aimed at achieving an activated clotting time of 250-300 seconds). Use of platelet glycoprotein IIb/IIIa inhibitors was also at the operator’s discretion.
After discharge, patients were followed as per local practice at one to three and six months. Thereafter, all patients were questioned at follow-up by experienced research nurses by means of a direct visit or phone contact between 11.5 and 12.5 months after the index procedure, to adjudicate events. In case of uncertainty or disagreement, source documents were retrieved and pertinent angiograms or hard copy documentation were examined in detail.
OPTICAL COHERENCE TOMOGRAPHY
Optical coherence tomography was acquired by means of the C7 XR system (St. Jude Medical, St. Paul, MN, USA)12,13,15. The FD-OCT imaging catheters were delivered over a 0.014” guidewire through the guiding catheter, after administration of intracoronary nitrates (100 μg). For effective clearing of blood from the imaging field, angiographic contrast media was injected through the guiding catheter with an automated power injector. Specifically, injection of 14 mL of contrast at a rate <4 mL/s was sufficient to achieve an imaging time of 2-3 seconds consistently in all of the major coronary branches. At a pull-back rate of 20 mm/sec, an imaging time of two seconds was long enough to scan a 4 cm-long segment. Frequency-domain OCT images were calibrated adjusting the Z-offset. This critical step was performed before image acquisition in order to obtain accurate measurements.
Optical coherence tomography images were analysed applying the following established definitions (Figure 1)15. Edge dissection was defined as the presence of a linear rim of tissue, with a width of ≥200 µm and a clear separation from the vessel wall or plaque that was adjacent (<5 mm) to a stent edge13,15. Reference lumen narrowing was defined as a lumen area <4.0 mm2. Stent malapposition was identified when the stent lumen distance was greater than the sum of strut thickness plus abluminal polymer thickness, according to each stent manufacturer’s specifications, plus a compensation factor of 20 µm to correct for strut blooming, and was considered significant if the stent lumen distance was greater than 200 µm13,16. Stent underexpansion was defined based on established IVUS criteria of optimal stent expansion (i.e., in-stent minimal lumen area ≥90% of the average reference lumen area or ≥100% of lumen area of the reference segment with the lowest lumen area)13. Thrombus was defined as intraluminal mass ≥200 µm, with no direct continuity with the surface of the vessel wall or a highly backscattered luminal protrusion in continuity with the vessel wall and resulting in signal-free shadowing15,17,18.
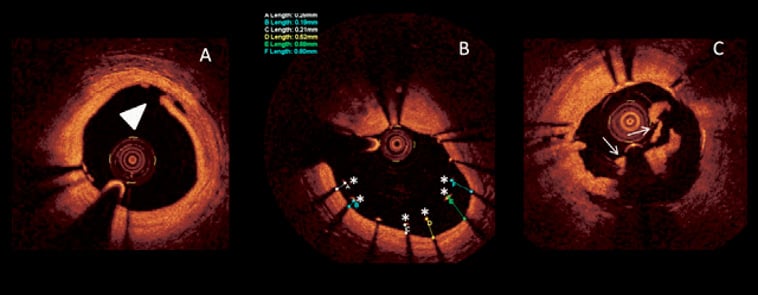
Figure 1. Optical coherence tomography assessment of acute complications during percutaneous coronary intervention. A) Edge dissection is imaged as a clear rim of tissue. B) Stent malapposition, with malapposed struts (asterisks) and their relative malapposition length shown. Stent struts can be identified from their bright blooming appearance and characteristic dorsal shadowing. C) Thrombus (arrow) is imaged as an irregular mass with dorsal shadowing protruding within the lumen.
The OCT quantitative criteria for optimal stent deployment were arbitrarily taken by authors when the protocol was devised to accomplish the goal of optimising stent positioning without overreacting to those minor alterations that are commonly observed by OCT13. The 200 µm threshold that was applied for many OCT criteria of optimal stenting is close to the resolution of IVUS. Such a threshold was chosen to address the clinical impact of the OCT technique which, having a ten times higher resolution, is capable of depicting findings likely to be missed by IVUS. Lastly, the reference lumen narrowing had to be greater than 4 mm2, as in previous IVUS studies. This cut-off was able to identify stents prone to thrombosis19.
The following actions were recommended when OCT disclosed such procedural issues not immediately recognised by angiography: edge dissection and reference lumen narrowing required the implantation of an additional stent at the edge of the previously implanted stent; stent underexpansion required further dilation of the previously implanted stent with a non-compliant balloon of the same diameter at ≥18 ATM or with a semi-compliant balloon having a diameter ≥0.25 mm larger than the previously used balloon at ≥14 ATM; stent malapposition required further dilation of the previously implanted stent with a non-compliant or semi-compliant balloon having a diameter ≥0.25 mm larger than the previously used balloon at ≥14 ATM; thrombus required further dilation of the previously implanted stent with a non-compliant or semi-compliant balloon of the same diameter at 8-14 ATM for 60 seconds.
The decision as to whether to perform further OCT assessments or additional interventions if the problem persisted was left at the operator’s discretion.
ENDPOINTS AND ADDITIONAL DEFINITIONS
The primary endpoint of the study was the 12-month rate of cardiac death or non-fatal myocardial infarction (MI). Additional endpoints were short-term (30-day) rates of death, cardiac death, and non-fatal MI, and 12-month rates of death, cardiac death, non-fatal MI, target lesion repeat revascularisation (TLR) and definite stent thrombosis. All outcomes were defined in keeping with the Academic Research Consortium recommendations20.
Statistical analysis
Continuous variables are reported as mean (standard deviation) and were compared with a Student’s t-test. Categorical variables are reported as n (%) and were compared with the chi-squared test (or the Fisher’s exact test, when an expected cell count was <5). Of note, matched pairs were not created for the purpose of direct hypothesis testing, but simply to ensure a contemporary mix of cases and controls. Addressing multiple confounders with matching would have been futile (as any dichotomous matching feature exponentially increases the possible alternatives for matching). Rather, matching was a preliminary process which was followed by extensive multivariable analyses aimed at controlling for known confounding factors. Specifically, multivariable logistic regression was used to adjust for potential confounders (covariates associated with OCT group at bivariate analyses with p<0.05), thus including in the final model the following variables: age, dyslipidaemia, prior PCI, admission diagnosis, number of diseased vessels, left main disease, PCI on left anterior descending, multivessel PCI, stent length per patient, DES usage, stent overlap, and maximum balloon diameter. Independence and lack of collinearity between covariates entered into the multivariable model were explicitly appraised (finding no statistical evidence of dependence or collinearity). We opted for a 0.05 entry cut-off to be pragmatic and to include obviously important covariates while not burdening the model with too many independent variables. Despite this, the event per variable ratio was lower than optimal (ideal value above 8-10)21. Since our multivariable model, as it was without further statistical ameliorations, was at substantial risk of overfitting or biased results, we added propensity score adjustment and bootstrapping. Thus, non-parsimonious propensity score-adjusted analyses were performed, exploiting bootstrap resampling (with 95% confidence intervals based on 1,000 bootstrap samples)21. Cox proportional hazard models were also used for sensitivity analyses. Statistical significance was set at the two-tailed 0.05 level. All computations were performed with SPSS 19.0 (SPSS Inc., Chicago, IL, USA).
Results
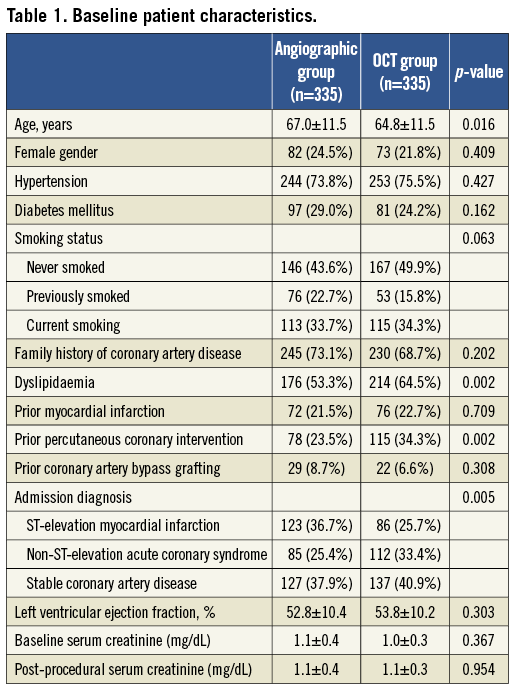
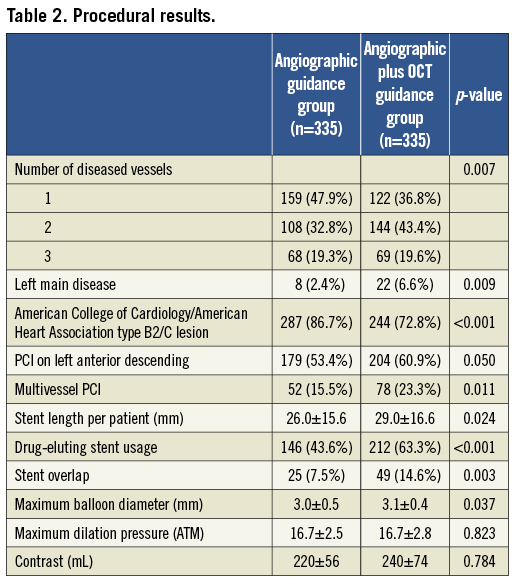
A total of 670 patients were included, 335 in the OCT group and 335 in the Angio group. Baseline and procedural features are reported in Table 1 and Table 2, respectively. Patients in the Angio group were older (67.0±11.5 years vs. 64.8±11.5 years, p=0.016), more frequently presented with ST-elevation MI (36.7% vs. 25.7%, p=0.005), type B2/C lesions (86.7% vs. 72.8%, p<0.001) and were less likely to be treated with DES (43.6% vs. 63.3%, p<0.001). Conversely, subjects in the OCT group had a higher prevalence of non-ST-elevation acute coronary syndromes (33.4% vs. 25.4%, p=0.005), dyslipidaemia (53.3% vs. 64.5%, p=0.002), prior PCI (23.5% vs. 34.3%, p=0.002), multivessel disease (52.1% vs. 63.2%, p=0.007), and left main disease (2.4% vs. 6.6%, p=0.009), more frequently received treatment on the left anterior descending (53.4% vs. 60.9%, p=0.050) or multiple vessels (15.5% vs. 23.3%, p=0.011), had longer total stent length (26.0±15.6 mm vs. 29.0±16.6 mm, p=0.024), and more frequently received overlapping stents (7.5% vs. 14.6%, p=0.003) and larger balloons (3.0±0.5 mm vs. 3.1±0.4, p=0.037).
Acquisition of OCT was not associated with any major complication, as no case of significant spasm, dissection or life-threatening arrhythmia occurred (i.e., requiring pharmacologic therapy, revascularisation, or cardioversion/defibrillation). Accordingly, no significant differences in post-procedural renal function were found comparing the OCT group versus the Angio group. Conversely, OCT disclosed a number of adverse intracoronary features which could not be detected at angiography. Specifically, edge dissection was shown in 14.2%, lumen narrowing in 2.8%, stent malapposition in 29.7%, stent underexpansion in 11.4%, and thrombus in 22.0% (Table 3).
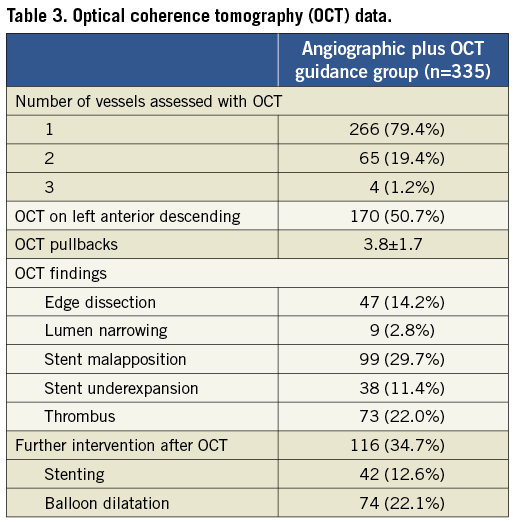
Findings resulting from OCT led to additional interventions in as many as 34.7% of the subjects (Table 3). Specifically, further stenting was performed in 12.6% of cases (in 5.4% to treat an edge dissection and in the remaining 7.2% to enlarge a reference lumen area that was <4 mm2). Additional balloon dilatation was needed in 22.1% of cases (in 14.0% to fix stent underexpansion, and in 8.1% to reduce intrastent thrombus).
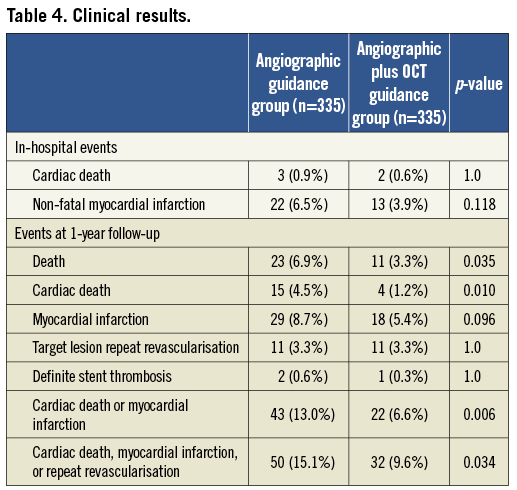
Short-term outcomes were similar in the OCT and Angio groups (Table 4). On the other hand, unadjusted analyses at mid-term follow-up showed that the OCT group had a significantly lower 12-month risk of cardiac death (1.2% vs. 4.5%, p=0.010), cardiac death or MI (6.6% vs. 13.0%, p=0.006), and the composite of cardiac death, MI, or repeat revascularisation (9.6% vs. 14.8%, p=0.044) (Table 4). Even at extensive multivariable logistic regression analysis adjusting for baseline and procedural differences between the groups, angiographic plus OCT guidance was associated with a significantly lower risk of cardiac death or MI (odds ratio =0.49 [0.25-0.96], p=0.037). Finally, propensity score-adjusted analysis exploiting bootstrap resampling confirmed the independent association between OCT and the 12-month rate of cardiac death or non-fatal MI (odds ratio=0.37 [0.10-0.90], p=0.050). Similar results were obtained with standard Cox proportional hazard analysis (hazard ratio=0.51 [0.28-0.93], p=0.028), as well as after propensity score adjustment and bootstrapping (hazard ratio=0.44 [0.21-0.92], p=0.030).
Discussion
This study, the first to date formally to compare angiographic plus OCT guidance versus angiographic guidance alone for routine PCI has the following implications: a) OCT can be safely performed to guide routine PCI; b) OCT discloses additional procedural issues not recognised by angiography in most unselected patients undergoing PCI, leading to additional interventions in a third of them; c) in this retrospective registry, OCT guidance on top of angiography was associated with significant clinical benefits even at multivariable analysis adjusting. Nevertheless, further randomised trials are eagerly awaited to confirm or disprove these favourable data supporting the role of OCT guidance to improve PCI results.
Percutaneous coronary revascularisation has seen momentous changes in the last few decades. Since its introduction, the evolution in techniques and devices has dramatically reduced the risk of early complications and has improved long-term results. However, it appears striking that we rely largely on the same imaging approaches the late Andreas Grüntzig exploited more than 30 years ago: fluoroscopy and angiography. Indeed, the limitations of angiographic guidance for coronary procedures are well established, but angiography is still the workhorse imaging approach for the vast majority of PCI cases.
Whereas IVUS appears useful in many settings, including bifurcation lesions, chronic total occlusions and diffuse disease, there is conflicting evidence on its role in improving clinical outcomes when used to guide PCI. Two randomised studies carried out in the 1990s failed to prove the superiority of an IVUS-guided approach versus the plain angiography-guided strategy6. However, a meta-analysis by Casella et al suggested that IVUS could reduce repeat revascularisation rates after BMS implantation6. More recently, Roy and colleagues and Park et al suggested that IVUS can reduce, respectively, stent thrombosis after DES implantation and mortality after PCI for unprotected left main disease7,22. However, other studies of similar quality have not confirmed such a beneficial impact of IVUS8,9.
One of the potential reasons for the not fully convincing results shown by IVUS study may be the limited spatial resolution of IVUS (100 μm axially, and 200-250 μm laterally). Instead, OCT provides very much higher resolution, in the range of 10-15 μm, despite only limited penetration into tissues12,15. Thus, OCT may have distinct practical advantages compared both to angiography and to IVUS, given its ability to identify lumen contours, struts and nearby structures correctly.
The promising role of OCT is clearly demonstrated by its leadership in clinical research, as all new coronary devices are currently investigated with this imaging technique. However, whether these theoretical advantages also translate into clinical benefits remains unclear. We previously reported on a pioneering experience of OCT guidance for PCI, including 74 patients with complex lesions, and demonstrated that OCT guidance is feasible and safe13.
Our present work thus builds upon these premises and exploits the experience and expertise with OCT achieved at the three participating centres. By using concurrent controls, this study provides statistical inference estimates for the risk benefit of angiographic plus OCT guidance versus angiographic guidance alone for PCI. We found that OCT can be safely and effectively performed whenever envisaged, thanks to the current low-profile probe and the non-occlusive technique. Moreover, we showed that OCT opens a real Pandora’s box of potentially serious procedural issues which are altogether missed by angiography, including edge dissection, reference lumen narrowing, stent malapposition, stent underexpansion and thrombus. This fact is demonstrated by the additional post-OCT interventions undertaken in 34.7% of patients receiving OCT.
The association between OCT guidance and improved clinical outcomes is promising and provides support for additional randomised trials on this topic. The fact that OCT did not increase short-term or mid-term adverse events is proof of its safety. In addition, the statistically significant reductions in cardiac death or non-fatal MI suggest that OCT guidance may minimise the presence and impact of procedural issues which can impact on cardiac death and/or MI, in particular periprocedural and in-hospital MI. The prognostic role of periprocedural or in-hospital MI has been the subject of on-going debate23, but it is reasonable to consider as prognostically ominous all large periprocedural MI (e.g., those associated with a peak CK-MB >5 times the upper limit of normal) or any periprocedural MI in a very frail or sick patient.
Limitations
This work has several limitations, including those typical of non-randomised studies relying on unadjusted and then multivariable adjusted analyses to control for known confounders and to make statistical inference21. Matching solely on the date of PCI may have created substantial imbalances between groups, with selection bias playing a potentially large role in the study.
Indeed, PCI in the emergency setting, which is fraught with a high risk of complications, was significantly more common in the angiographic guidance group. However, this was partly balanced by the more frequent adoption of OCT guidance for patients with urgent procedures (non-ST-elevation acute coronary syndromes) or more complex interventions. Due to these imbalances in the clinical distribution of the patients studied, we cannot exclude the possibility that the high adverse event rate we observed in the Angio group is due to a higher risk profile. In addition, the retrospective design and the lack of follow-up control angiography may, respectively, increase the risk of underlying bias and undermine the statistical power to detect outcome differences. Finally, as for any non-randomised study, while multivariable adjustment, especially including propensity scores and bootstrap, may reduce the impact of most known confounding factors, we should not forget that no method can truly adjust for all known confounders or for unknown confounders, and thus our results remain mainly hypothesis-generating.
Funding sources
This study was supported by the Centro per la Lotta contro l’Infarto – Fondazione Onlus, Rome, Italy.
Conflict of interest statement
The authors have no conflicts of interest to declare.