Abstract
Aims: Tricuspid regurgitation (TR) is associated with high morbidity and mortality rates with limited treatment options. We report one- and two-year outcomes of the Cardioband tricuspid valve reconstruction system in the treatment of ≥moderate functional TR in the TRI-REPAIR study.
Methods and results: Thirty patients were enrolled in this single-arm, multicentre, prospective study. Patients were evaluated as having ≥moderate, symptomatic functional TR and deemed inoperable due to unacceptable surgical risk. Clinical, functional, and echocardiographic data were prospectively collected up to two years (mean duration 604±227 days). At baseline, 83% were in NYHA Class III-IV, and the mean LVEF was 58%. Technical success was 100%. At two years, there were eight deaths. Echocardiography showed a significant reduction in septolateral annular diameter of 16% (p=0.006) and 72% of patients (p=0.016) with ≤moderate TR grade; 82% of patients were in NYHA Class I-II (p=0.002). Six-minute walk distance and KCCQ score improved by 73 m (p=0.058) and 14 points (p=0.046), respectively.
Conclusions: These results demonstrate that the Cardioband tricuspid system showed favourable results in patients with symptomatic, ≥moderate functional TR. Annular reduction and TR severity reduction remained significant and sustained at two years. Patients experienced improvements in quality of life and exercise capacity. ClinicalTrials.gov Identifier: NCT02981953
Introduction
The reported US age- and sex-adjusted prevalence of moderate or greater tricuspid regurgitation (TR) is 0.55%1. The prevalence increases with age. This was confirmed by the OxVALVE population cohort study which found that ~2.7% of their patients (age 74.2±6.5 years) had moderate or greater TR2. A recent meta-analysis of 70 studies showed that, compared to patients with no TR, patients with mild, moderate, or severe TR had a progressively increased risk of all-cause mortality3.
Functional TR accounts for 90% of patients diagnosed with TR and is potentially caused by dilatation of the annulus as a result of increased pulmonary and right ventricular pressure, and atrial fibrillation4. In the USA alone, there are more than 1.6 million cases of moderate or greater TR and only 8,000 surgical procedures performed annually5,6. Corrective surgery for TR in patients who frequently have multiple comorbidities is associated with significantly high in-hospital mortality, although improved outcomes may be achieved with minimally invasive approaches7,8. Current guidelines recommend surgery for functional TR only in patients undergoing left-sided valve surgery9. Most of these procedures are accomplished using surgical annuloplasty.
A transcatheter approach may be a suitable option for patients suffering from moderate or greater TR who are at high or prohibitive surgical risk10,11. The Cardioband™ tricuspid valve reconstruction system (Edwards Lifesciences, Irvine, CA, USA) addresses TR through annular reduction and is the first CE mark-approved transcatheter therapy for the treatment of TR. We previously reported six-month results of the TRI-REPAIR study and herein we report two-year outcomes12.
Methods
TRIAL DESIGN AND PATIENT SELECTION
Between October 2016 and July 2017, 30 patients were deemed eligible by the site Heart Team and enrolled at eight EU sites in the single-arm, multicentre, prospective TRI-REPAIR study to evaluate the safety and performance of the Cardioband tricuspid system in patients with functional TR. Key eligibility criteria included New York Heart Association (NYHA) functional Class II-IVa, moderate or greater chronic functional TR, symptomatic despite stable medical treatment at minimum on a diuretic regimen, tricuspid annular diameter ≥40 mm, and surgery precluded as a treatment option. Key exclusion criteria included left ventricular ejection fraction (LVEF) <30%, systolic pulmonary artery pressure >60 mmHg, echocardiographic evidence of severe right ventricular dysfunction, and recent myocardial infarction or known unstable angina within 30 days prior to the index procedure12. The TRI-REPAIR study was conducted in conformity with the ethical principles set forth in the Declaration of Helsinki, Good Clinical Practice principles, and in accordance with ISO 14155:2011. The study was approved by local ethics committees and the respective health authorities of the participating countries. It is registered in clinicaltrials.gov (NCT02981953). All patients provided written informed consent.
ECHOCARDIOGRAPHY ANALYSES
TR severity and anatomical assessment for device implantation was performed by the sites using transthoracic (TTE), transoesophageal echocardiography (TEE), and cardiac computed tomography (CT). Thereafter, the implant size was chosen according to the preoperative measurements of the tricuspid annulus length using a cardiac CT scan at maximal diastolic opening of the valve. TEE and fluoroscopic guidance were performed intraprocedurally to facilitate implantation. TTE was performed at baseline and for all post-procedural clinical follow-up visits. To gauge right coronary artery (RCA) proximity, intraprocedural coronary angiography was performed several times to prevent complications.
An independent core laboratory (Cardiovascular Research Foundation, New York, NY, USA) assessed all echocardiographic data based on American Society of Echocardiography (ASE) guidelines13. The tricuspid annular diameter was measured from the four-chamber view in end-diastole. Proximal isovelocity surface area (PISA) was assessed using 2D colour flow Doppler where the TR jet was aligned with the insonation beam and the colour Doppler baseline shifted in the direction of the TR jet. A Nyquist limit between 25 and 35 cm/sec was used to optimise the PISA signal. The vena contracta is elliptical; therefore, its width was calculated as an average of the measured diameters in two orthogonal planes (simultaneous multi-plane image or from the four-chamber view and the inflow view). Quantitation of effective regurgitant orifice area (EROA) and regurgitant volume was performed by PISA and Doppler volumetric methods14.
The TR was assessed using standard 2D colour Doppler methods and its severity was graded according to the five-grade scheme proposed by Hahn and Zamorano15.
THE CARDIOBAND TRICUSPID SYSTEM
The Cardioband tricuspid system is designed for valve reconstruction through a transfemoral approach and delivers an adjustable implant for annular reduction12. Briefly, the implant consists of a contraction wire and polyester fabric covering with radiopaque markers attached to an adjustment mechanism. It is deployed along the anterior and posterior regions of the annulus and is affixed using a series of anchors in a stepwise manner under echocardiographic and fluoroscopic guidance for optimal placement (Figure 1). Once the implant is affixed to the annulus, the size-adjustment tool is introduced over a wire to contract the Cardioband tricuspid implant. Reduction of the tricuspid annular diameter is assessed in real time by echocardiography under beating heart conditions and adjusted as appropriate to minimise TR. Once the TR is optimally reduced, the implant is detached from the delivery system and the delivery system is removed.
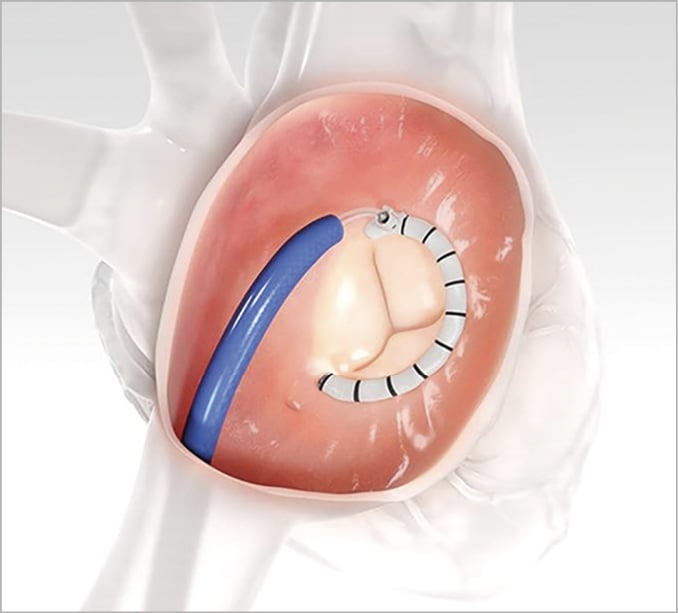
Figure 1. Transcatheter Cardioband Tricuspid Valve Reconstruction System. Cardioband tricuspid implant along the adjusted tricuspid valve annulus. Image provided by Edwards Lifesciences with permission.
TRIAL ENDPOINTS
The primary performance endpoint for the TRI-REPAIR study was successful access, deployment, and positioning of the Cardioband tricuspid implant and reduction of the septolateral annular diameter at the end of the procedure and at discharge. The primary safety endpoint was the rate of major serious adverse events (MSAEs; a composite endpoint of death, myocardial infarction, cardiac tamponade, device-related cardiac surgery, and stroke) and serious adverse device effects (SADEs) at 30 days12. All MSAEs and SADEs throughout the follow-up period were adjudicated by an independent clinical events committee (Cardiovascular Research Foundation, New York, NY, USA). We herein report one- and two-year outcomes including the secondary endpoints septolateral annular diameter, TR severity, PISA EROA, mean vena contracta, NYHA class, oedema as assessed by pitting oedema, six-minute walk test (6MWT), and Kansas City Cardiomyopathy Questionnaire (KCCQ).
STATISTICAL ANALYSIS
Statistical comparison between baseline and post-procedure follow-up periods was performed using paired analyses. Either the Student’s t-test or the Wilcoxon signed-rank test was performed post hoc. Time-to-event variables were analysed using Kaplan-Meier survival analysis. Statistical significance was set at p<0.05 as two-tailed tests and the analyses were performed using SAS software, version 9.4 (SAS Institute, Inc., Cary, NC, USA). Results are presented as mean±SD.
Results
BASELINE CHARACTERISTICS
Mean patient age was 75±7 years with the majority being female (n=22; 73%) and in NYHA Class III-IV (n=25; 83%). All patients had functional TR, and the majority of patients had atrial fibrillation (n=28; 93%), systemic hypertension (n=24; 80%), and chronic renal disease (n=16; 53%). Other comorbidities included diabetes (n=8; 27%) and elevated systolic pulmonary artery pressure (n=15; 50%). Mean European System for Cardiac Operative Risk Evaluation (EuroSCORE II) was 4.1%, Society of Thoracic Surgeons (STS) mortality score was 2.6%, and the NT-proBNP level was 2,925 ng/L (n=23) (Table 1). One- and two-year follow-up was performed in 24 and 20 patients, respectively (Figure 2). The mean duration of patient follow-up was 604±227 days.
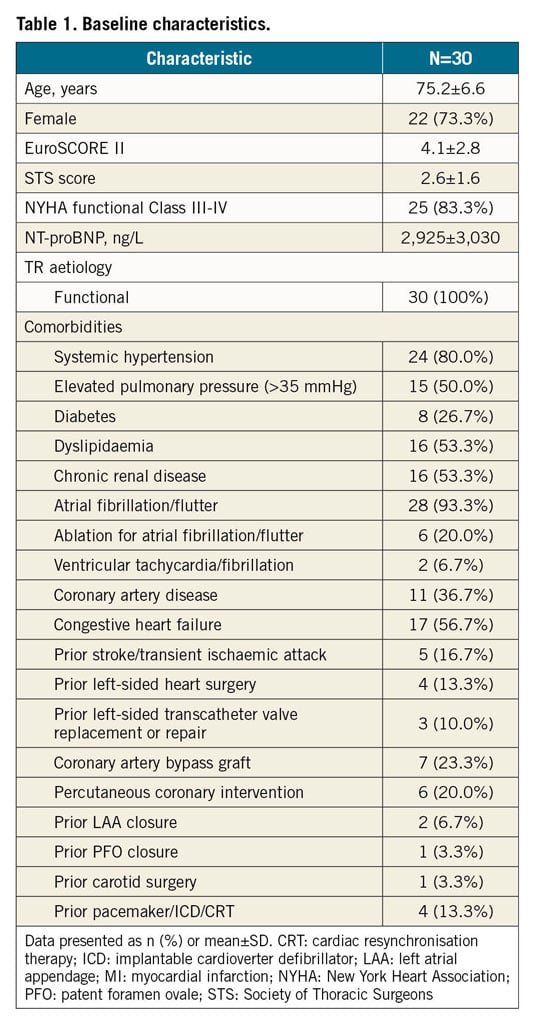
Figure 2. Patient disposition diagram. ¶One device-related. *Died between one and two years.
ECHOCARDIOGRAPHIC RESULTS
The primary performance endpoint, technical success, was 100%.
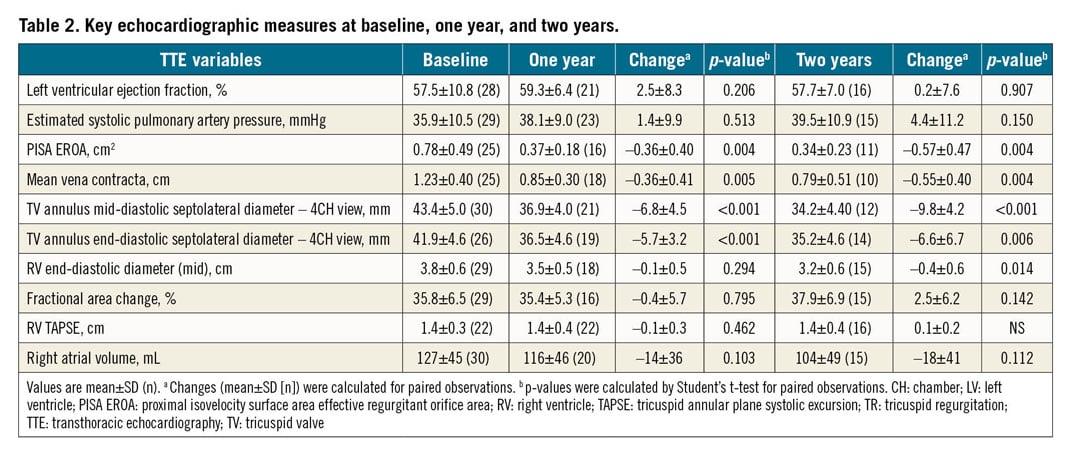
At baseline, the end-diastolic septolateral diameter was 41.9±4.6 mm (n=26). Multiple quantitative measurements of TR severity assessed by parameters such as PISA EROA, mean vena contracta, and regurgitant volume, were all elevated (Table 2). TR severity by PISA EROA was measured by the sites and evaluable by the core laboratory in 25 patients: 19 (76%) were graded severe to torrential, 5 (20%) moderate, and 1 (4%) mild TR. Paired echocardiographic data comparing baseline measurements to one-year and two-year measurements are provided (Table 2).
Annular diameter was significantly reduced at discharge and this was sustained at one and two years. End-diastolic septolateral annular diameter was 41.9±4.6 mm (n=26) at baseline, 36.2±4.7 mm (n=22) at discharge (p<0.001; paired analysis compared to baseline), 36.5±3.3 mm (n=19) at one year (p<0.001; paired analysis compared to baseline), and 35.2±4.6 mm (n=14) at two years (p<0.001; paired analysis compared to baseline) (Figure 3). Along with reduction in annular diameter after the procedure, TR severity improved significantly. Whereas 24% of patients had ≤moderate TR at baseline, this progressively increased to 55% (p<0.001; paired analysis compared to baseline) at discharge, 63% (p=0.007; paired analysis compared to baseline) at one year, and 72% at two years (p=0.016; paired analysis compared to baseline) (Figure 3).
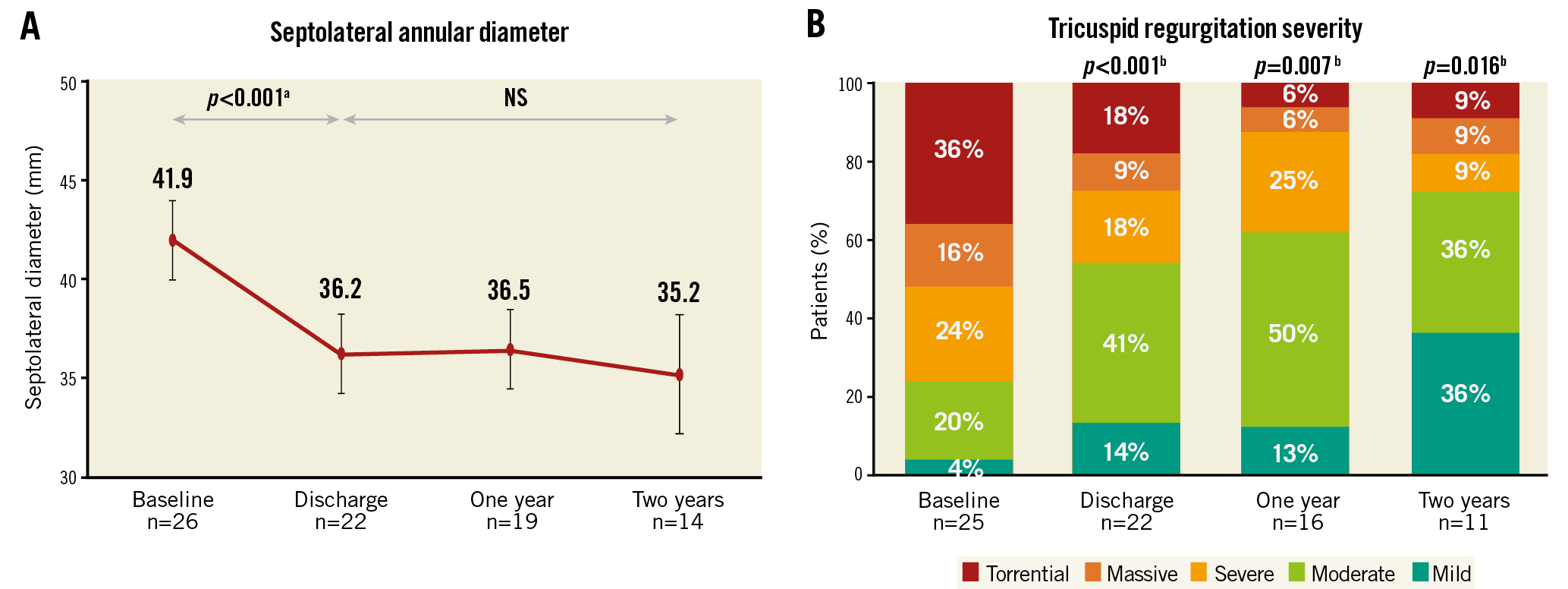
Figure 3. Reduction in septolateral annular diameter and tricuspid regurgitation severity for the Cardioband Tricuspid Valve Reconstruction System. A) Significant reduction in end-diastolic septolateral annular diameter. B) Mild/moderate TR was present in 24% of patients at baseline, 63% at one year (p=0.007) and 72% at two years (p=0.016). Paired Student’s t-test for continuous variables or the Wilcoxon signed-rank test for categorical variables. aBaseline vs discharge (n=22), baseline vs one year (n=17) or baseline vs two years (n=12). bBaseline vs discharge (n=20), baseline vs one year (n=15) or baseline vs two years (n=10). The figure reports all available data, i.e., unpaired. The p-values were calculated from paired data reflected in the figure legend.
Furthermore, PISA EROA significantly reduced from 0.8±0.5 cm2 (n=25) at baseline to 0.5±0.4 cm2 (n=22) at discharge (p<0.001; paired analysis compared to baseline), 0.4±0.2 cm2 (n=16) at one year (p=0.004; paired analysis compared to baseline), and was sustained at 0.3±0.2 cm2 (n=11) at two years (p=0.004; paired analysis compared to baseline) (Table 2). Similarly, mean vena contracta decreased from 1.2±0.4 cm (n=25) at baseline to 1.0±0.5 cm (n=20) at discharge (p=0.012; paired analysis compared to baseline), 0.8±0.3 cm (n=18) at one year (p=0.005; paired analysis compared to baseline), and was sustained at 0.8±0.5 cm (n=10) at two years (p=0.004; paired analysis compared to baseline) (Table 2).
FUNCTIONAL AND CLINICAL RESULTS
At one and two years, functional status was improved from baseline. Seventeen percent (17%) of patients were in NYHA Class I-II at baseline, which increased significantly to 78% (p<0.001; paired analysis compared to baseline) and 82% (p=0.002; paired analysis compared to baseline) at one year and two years, respectively (Figure 4A). In addition, 37% of patients had no oedema at baseline, which increased to 70% at one year (p=0.073; paired analysis compared to baseline), and 88% at two years (p=0.063; paired analysis compared to baseline) (Figure 4B).
Six-minute walk distance had increased by 42 metres at one year (p=0.053; paired analysis) and 73 metres at two years (p=0.058; paired analysis) when compared to baseline (Figure 4C). Similarly, the overall KCCQ score had increased by 19 points at one year (p<0.001; paired analysis) and 14 points at two years (p=0.046; paired analysis) when compared to baseline (Figure 4D).
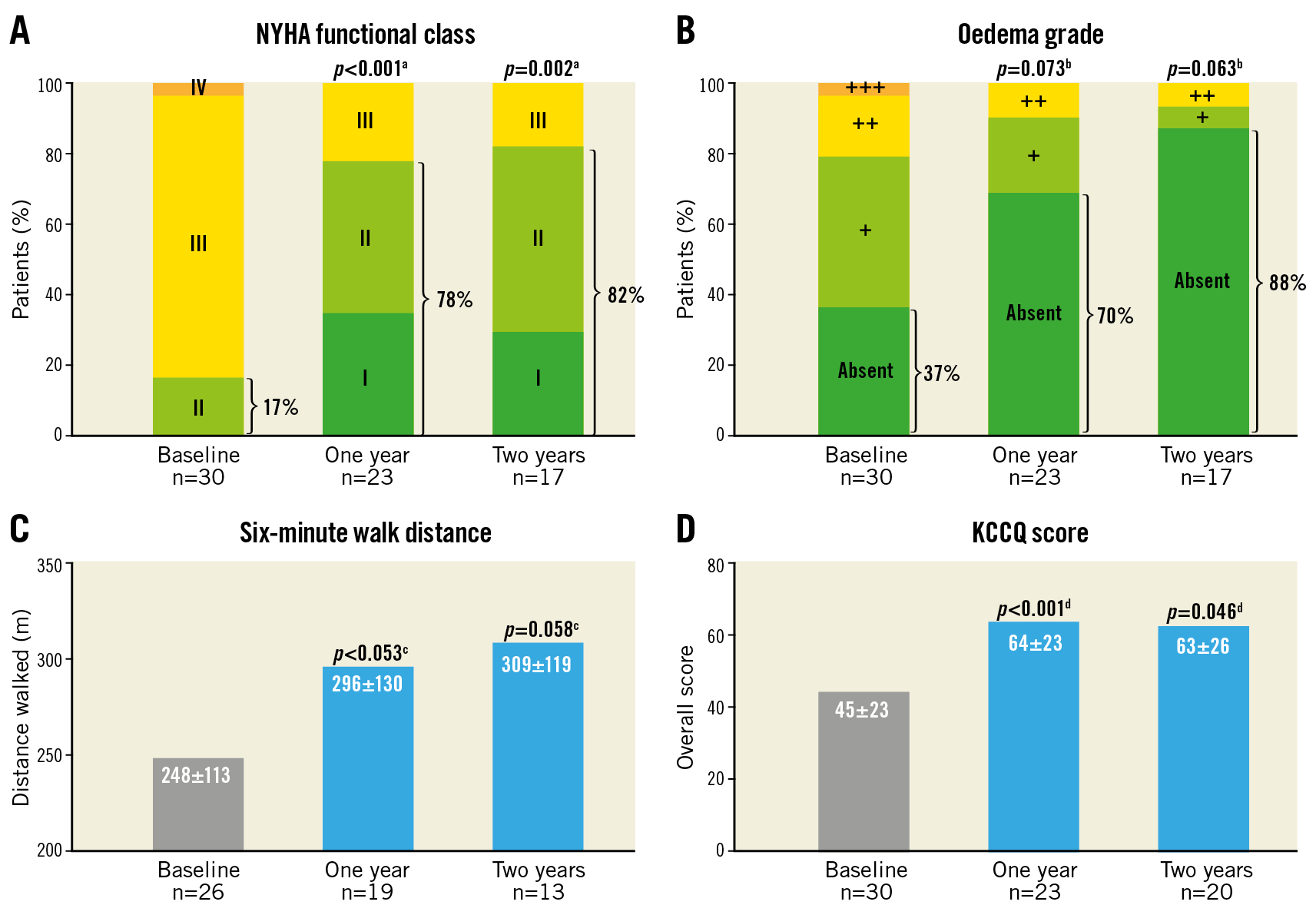
Figure 4. Clinical and functional improvements from baseline to two years for the Cardioband Tricuspid Valve Reconstruction System. A) New York Heart Association (NYHA) functional Class I-II was increased to 82% at two years. B) Oedema grade ++ or worse, classified by pitted oedema grades, was reduced to 6% at two years. C) Six-minute walk distance increased to 309±119 metres at two years. D) Kansas City Cardiomyopathy Questionnaire (KCCQ) scores increased to 63±26 points at two years. Paired Student’s t-test for continuous variables or the Wilcoxon signed-rank test for categorical variables. aBaseline vs one year (n=23) or baseline vs two years (n=17). bBaseline vs one year (n=23) or baseline vs two years (n=17). cBaseline vs one year (n=19) or baseline vs two years (n=12). dBaseline vs one year (n=23) or baseline vs two years (n=20). The figure reports all available data, i.e., unpaired. The p-values were calculated from paired data reflected in the figure legend.
ADVERSE EVENTS
Adverse events are summarised in Table 3. The two-year survival and freedom from heart failure (HF) hospitalisation Kaplan-Meier estimates were 73±8% (Figure 5A) and 56±10% (Figure 5B), respectively. At two years, there were eight deaths. Six non-cardiovascular deaths beyond 30 days included one patient due to progression of chronic lymphatic leukaemia, one patient due to respiratory failure, one patient due to worsening of chronic renal failure, one patient who died due to multifactorial reasons primarily pulmonary artery embolism, one patient due to acute renal failure, and one patient due to metastatic liver cancer. Two patients underwent device-related secondary interventions as a result of worsening TR. There were other late events that were not related to the device or procedure: one patient experienced a late non-disabling ischaemic stroke, three patients experienced severe bleeding complications, one patient experienced conduction system disturbance and one patient experienced ventricular tachycardia. There were no late instances of renal failure or coronary complications. Throughout follow-up, there were no myocardial infarctions and no device-related cardiac surgery.
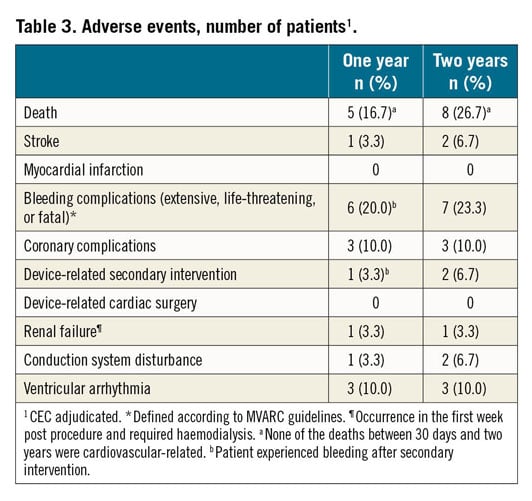
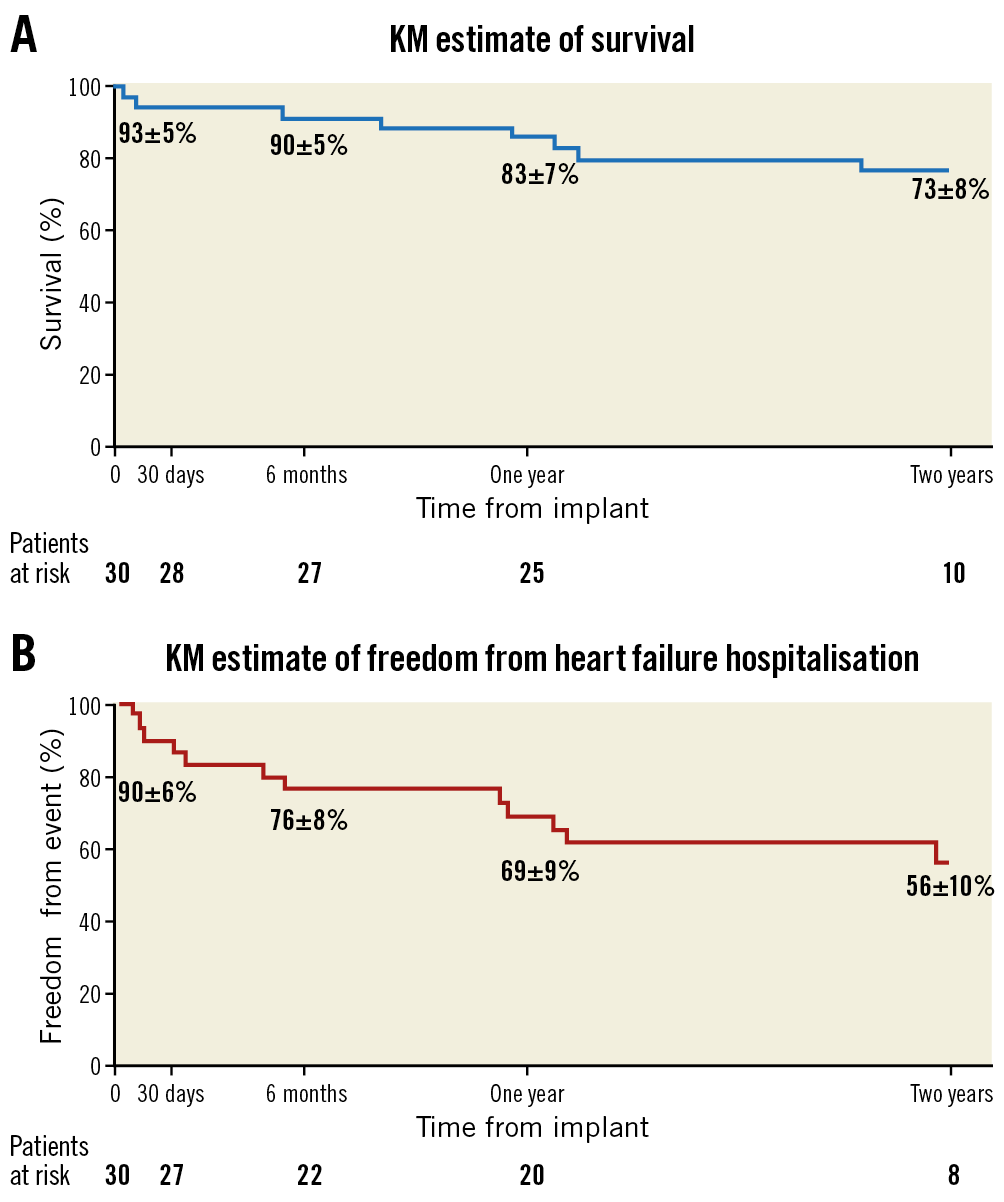
Figure 5. Two-year survival and hospitalisation Kaplan-Meier curves. A) The KM estimate of survival at two years was 73%. B) The KM estimate of freedom from heart failure hospitalisation at two years was 56%.
Discussion
At the two-year follow-up, the TRI-REPAIR study shows significant reduction of tricuspid annular dimension and TR, leading to amelioration of HF symptoms and increased exercise capacity with one- and two-year survival rates of 83% and 73%, respectively. This contrasts with two-year survival rates closer to 60% for medical therapy in prior reports6,16,17.
Although we have strong epidemiological evidence that TR is related to poor outcomes, data which prove that dedicated TR reduction leads to improved prognosis are lacking. Taramasso et al compared outcomes of medical therapy and device therapy by propensity matching a control cohort formed from two large retrospective registries enrolling medically managed patients with moderate or greater TR with patients enrolled in the TriValve registry16. Transcatheter tricuspid valve intervention was associated with greater survival and freedom from HF rehospitalisation which remained significant after adjusting for sex, NYHA class, right ventricular dysfunction, and atrial fibrillation (HR 0.39, 95% CI: 0.26 to 0.59; p<0.0001) and after further adjustment for mitral regurgitation and pacemaker/defibrillator (HR 0.35, 95% CI: 0.23 to 0.54; p<0.0001).
Annular flattening and dilatation are thought to be the earliest morphologic changes associated with TR, with ventricular dilatation occurring late or in association with significant pulmonary hypertension18. Annular dilatation has been directly correlated with TR severity and progression of disease19. Thus, annuloplasty has long been considered the treatment of choice for most patients with severe, symptomatic TR, reserving replacement for patients presenting with severe right ventricular dilatation and marked tricuspid leaflet tethering20. Given the high in-hospital mortality associated with isolated TR surgery, transcatheter options, particularly one that mimics the preferred surgical procedure, would have a clear rationale. In-hospital mortality in the TRI-REPAIR study was 3.3%, which compares favourably with the 8.8% in-hospital mortality for isolated TR surgery7,12.
There remain limitations to annular repair. Severe anatomical leaflet defects preclude sole annular repair and may leave replacement as the only treatment choice. The RCA is located in anatomic vicinity to the tricuspid annulus and remains an important screening consideration, but fortunately too close proximity of the artery to the annulus is an uncommon cause for excluding patients from this procedure12.
Unfortunately, many TR patients receive appropriate clinical attention too late in the natural history of the disease. Many patients suffer from severe and progressive right heart dilatation, leading to tethering of the leaflets towards the ventricular apex. If the tenting distance exceeds 10 mm, an isolated annular reduction may not be the appropriate solution for TR repair, as is also known from open heart surgery21. In addition, progressive right heart dilatation and impairment is associated with extensive annular dilatation, sometimes exceeding a septolateral distance of 50 mm. These annuli are too large to be treated with the current sizes of the Cardioband device. On the one hand, this issue may be resolved by providing larger implant devices; on the other hand, timely identification and earlier selection of patients in need may help to resolve this issue.
Many patients in the TRI-REPAIR study had severe right ventricular and annular dilatation and almost half of the patients displayed not just severe but massive or torrential TR. Nevertheless, annular dimensions were reduced in all patients and, in most patients, this was accompanied by a significant reduction of TR. The clinical benefit as assessed by HF symptoms and exercise capacity after TR reduction in some patients was impressive. Symptomatic relief was seen even though we were able to reduce TR to moderate or less in only 63% of patients at one year and 72% at two years. Similar findings were recently reported with leaflet repair devices22,23. It may be speculated that even such a modest reduction in TR severity impacts profoundly on renal and hepatic perfusion and could improve forward stroke volume and cardiac output.
As in other feasibility studies, patients enrolled in the TRI-REPAIR study were selected based on protocol-defined inclusion criteria; a wider experience is needed to determine the potential for the Cardioband tricuspid system to treat all TR patients. Consistent with the inclusion criteria, all enrolled patients had site-reported moderate or greater TR with a tricuspid annular diameter of >40 mm. Some site-reported values differed from core laboratory assessments, which reported one patient as having mild TR and six patients as having a tricuspid annular diameter <40 mm. Regardless, the overall interpretation of the study did not change when these seven patients were eliminated in a sensitivity analysis12.
Catheter-based treatment of TR is in its infancy and current scientific activities are predominantly feasibility studies. The Cardioband tricuspid system and leaflet repair devices are the only CE-approved catheter-based treatment of TR in Europe. Even though these approaches appear safe with low periprocedural complication rates, their efficacy is limited in patients with severe or greater TR. Catheter-based tricuspid valve replacement has the potential to eliminate TR, with percutaneous approaches being developed. However, afterload mismatch has been observed subsequent to the eradication of TR in patients with impaired right ventricular function.
There are no head-to-head comparisons between devices, but at least some initial experience with combination procedures exists. In many patients, intense annular dilatation leads to extensive leaflet malcoaptation, precluding a leaflet repair approach as the primary option. On the other hand, tethering due to RV dilatation is an additional common finding in those patients. Therefore, it is reasonable to combine annular reduction via the Cardioband tricuspid system with subsequent leaflet repair therapy. Some initial case experiences appear promising23.
Limitations
This was a single-arm, early feasibility study with 30 patients. Study-related limitations include different site-reported values from core laboratory assessments (one patient had mild TR) and missing TR quantitation (PISA EROA) due to inadequate imaging despite site training. These limitations highlight the need for standardising TR assessment, the dependence of TR on loading conditions, and the limitations of assessing TR at a single time point. Finally, the sustained benefit seen in this cohort of survivors may reflect a survivorship bias as well as a self-selection of patients with either less baseline TR or greater TR reduction. Long-term TR reduction as well as durability of annular repair with the Cardioband tricuspid system requires further study. The next logical step is controlled randomised studies which test the hypothesis that transcatheter treatment of TR improves patient outcomes compared to medical therapy.
Conclusions
In the TRI-REPAIR study, in patients with moderate or greater functional TR, annular repair with the Cardioband tricuspid system resulted in sustained and significant TR reduction with a low complication rate at two years. Survival was 73% with no late cardiovascular deaths. Substantial improvements in functional class, exercise capacity and quality of life were sustained at two years.
|
Impact on daily practice The Cardioband tricuspid system resulted in sustained echocardiographic, clinical, and functional improvements at two years in patients with moderate or greater TR, demonstrating that annular reduction with the Cardioband tricuspid system is a favourable option to treat patients with clinically significant functional TR. |
Acknowledgements
A list of investigators, institutions, and research organisations participating in the TRI-REPAIR study is provided in Supplementary Appendix 1.
Funding
Funded by Edwards Lifesciences.
Conflict of interest statement
G. Nickenig, R.S. von Bardeleben, U. Schäfer, S. Baldus, M. Montorfano, and F. Deuschl have received speakers’ honoraria as well as travel and grant support from Edwards Lifesciences. E. Agricola and R. Schüler have received speakers’ honoraria from Edwards Lifesciences. F. Deuschl, S.H. Deo, S. Gilmore, and T. Feldman are employees of Edwards Lifesciences. R.T. Hahn reports speaker honoraria from Baylis Medical, Edwards Lifesciences and Medtronic, consulting for Abbott Structural, Edwards Lifesciences, Medtronic, Navigate and Philips Healthcare, and being the Chief Scientific Officer for the Echocardiography Core Laboratory at the Cardiovascular Research Foundation for multiple industry-sponsored trials, for which she receives no direct industry compensation. The other authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.