A 76-year-old patient (logistic EuroSCORE 42.7%) was referred for severe aortic regurgitation (AR) secondary to non-calcific degeneration of a 27 mm stentless prosthesis (Appendix Figure 1). TAVI was performed with a transfemoral inflatable, non-metallic, repositionable and fully retrievable valve (25 mm Direct Flow®; Direct Flow Medical Inc., Santa Rosa, CA, USA) (Figure 1A). With the unsheathed valve in the left ventricle, the rings were inflated at 4 atm (“low pressure technique”). Once the valve was parallel to the aortic valve annulus, the upper ring was deflated. The system’s inner catheter was advanced (black arrow, Figure 1B) in order to shorten the wire’s length and control pulling forces. An “inner curve technique” was adopted by pulling the valve wire closer to the inner aortic curve, to reach annular contact in the “hinge point” (star, Figure 1B). The outer curve wire was then pulled to achieve full circumferential contact with the stentless valve annulus (Figure 1B). The valve was inflated to 12 atm (Figure 1C). Aortography confirmed no aortic regurgitation (Appendix Figure 2).
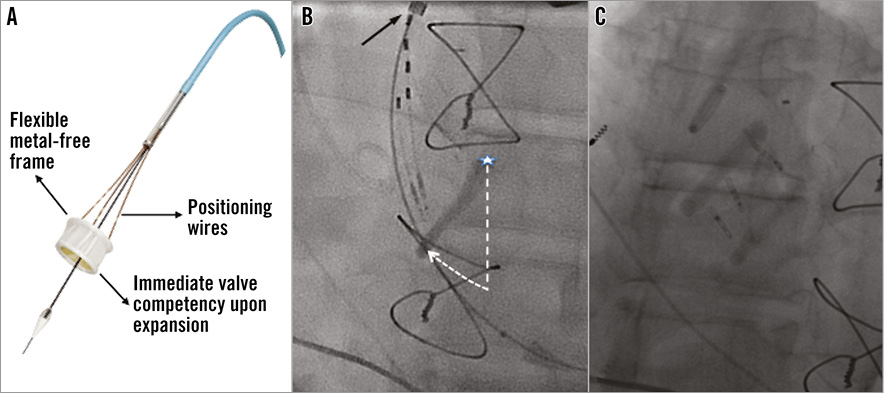
Figure 1. Direct Flow Medical Transcatheter Aortic Valve System. A) The Direct Flow Medical prosthesis. B) Valve positioning phases. Dashed straight and curved lines represent the “closing door” movement (see text for explanation). C) Final valve position.
In conclusion, the Direct Flow® intrinsic features might render this technology a valuable tool to treat pure AR.
Conflict of interest statement
S. Kische and H. Ince are Direct Flow proctors. The other authors have no conflicts of interest to declare.
Appendix
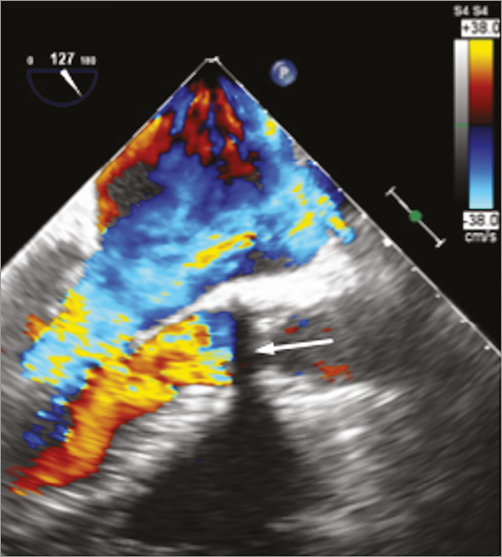
Appendix Figure 1. Preoperative echocardiography showing severe aortic regurgitation of a previously implanted stentless aortic valve (white solid arrow).
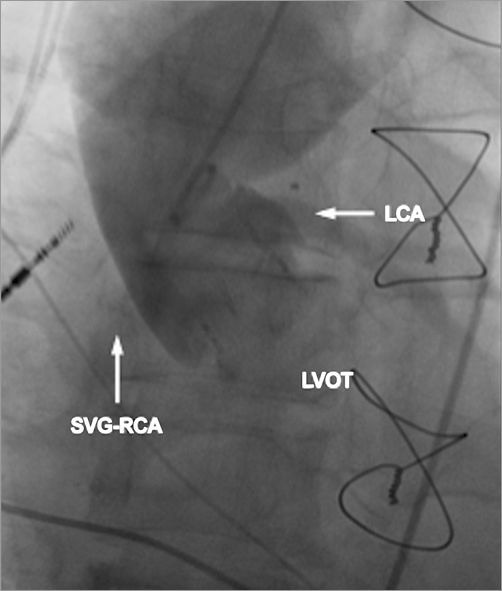
Appendix Figure 2. Aortography confirming no residual aortic regurgitation and patency of left main coronary artery (LCA) and saphenous vein graft to the right coronary artery (SVG-RCA).