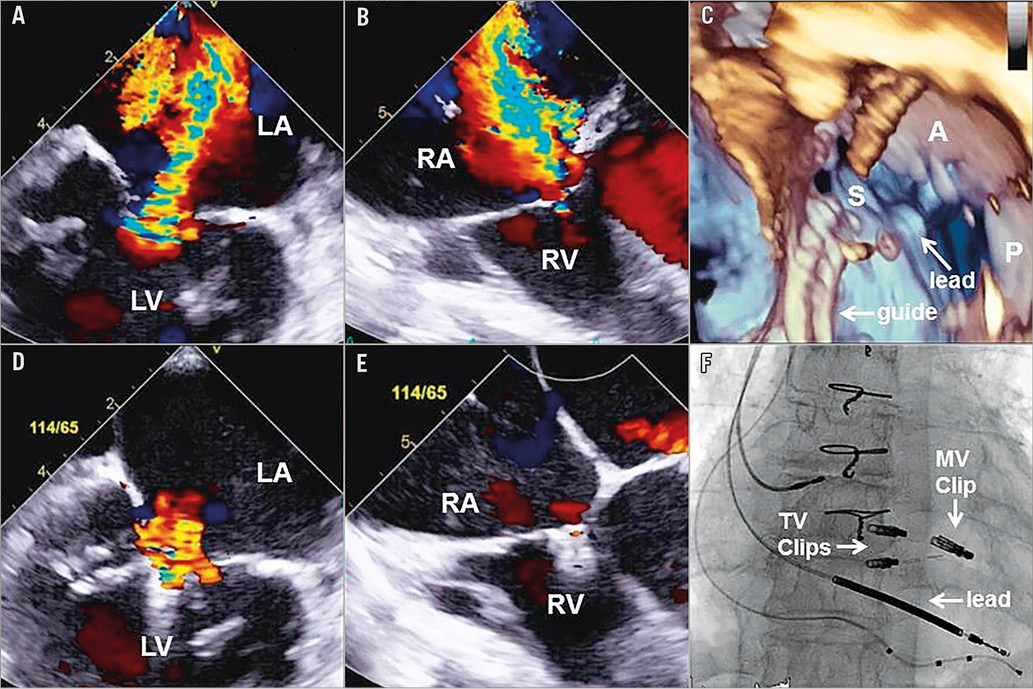
A 70-year-old woman presented with heart failure. Past history included coronary disease with previous coronary artery bypass grafting (CABG) and percutaneous coronary intervention (PCI), left ventricular (LV) dysfunction with ejection fraction (EF) 30%, previous implantable cardioverter defibrillator (ICD) and atrial fibrillation. The patient had persistent NYHA Class III dyspnoea, fatigue and peripheral oedema despite medical therapy and cardiac resynchronisation therapy (CRT) upgrade one year prior. Echocardiography demonstrated severe secondary mitral regurgitation (MR) (Panel A) and severe secondary tricuspid regurgitation (TR) (Panel B) due to ICD lead impingement on the septal leaflet and annular dilatation (Panel C, Moving image 1). After Heart Team review, combined transcatheter mitral and tricuspid repair with the MitraClip (Abbott Vascular, Santa Clara, CA, USA) was planned.
A single MitraClip was deployed at A2-P2 resulting in mild MR (Panel D) with a mean gradient of 2 mmHg. After withdrawing the guide catheter into the right atrium, the clip delivery system was navigated perpendicular to the anterior and septal leaflets using 3D transoesophageal echo and fluoroscopy (Panel C, Moving image 2). The anterior and septal leaflets were treated with two clips, starting at the commissure and carefully avoiding the lead, resulting in mild TR (Panel E, Panel F, Moving image 3) with a mean gradient of 2 mmHg. The patient was discharged home the next day. At one-month follow-up, she reported improved symptoms and functional capacity. Baseline 6-minute walk test increased from 260 to 400 m, and NT-BNP decreased from 4,394 to 3,572 ng/L. Repeat echocardiography was unchanged.
Tricuspid regurgitation (TR) is an increasingly recognised complication of pacemaker and defibrillator lead insertion, and carries a poor prognosis1,2. The septal and posterior leaflets are most frequently involved, with TR resulting from lead perforation, impingement or adherence to the leaflets, often with associated tethering. Surgical treatment usually involves lead repositioning and leaflet repair combined with annuloplasty, but has significant associated morbidity and mortality. Of the currently available transcatheter tricuspid repair devices, only the MitraClip can directly address lead-induced leaflet tethering3.
In this report, we demonstrate the feasibility of MitraClip for lead-associated TR, treating the anterior and septal leaflets with significant and sustained TR reduction. Given that TR caused by device leads is often focal, it would appear ideally suited for edge-to-edge repair with the MitraClip. In our case, TR was due to both lead-induced septal leaflet tethering and annular dilatation, and TR reduction was achieved by improved coaptation between the anterior and septal leaflets after implantation of two clips.
Comprehensive echo assessment to determine the mechanism of TR is essential prior to considering intervention, and operators should avoid placing clips too close to device leads to prevent leaflet trauma. In future, combined transcatheter tricuspid edge-to-edge repair and annuloplasty may provide the best long-term outcomes, reproducing the surgical standard.
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
Moving image 1. Preprocedural 3D TEE demonstrating impingement of the septal leaflet by the ICD lead.
Moving image 2. Intraprocedural 3D TEE of guide navigation in the right atrium.
Moving image 3. Post-procedural 3D TEE after implantation of clips between anterior and septal leaflets.
Supplementary data
To read the full content of this article, please download the PDF.
Preprocedural 3D TEE demonstrating impingement of the septal leaflet by the ICD lead.
Intraprocedural 3D TEE of guide navigation in the right atrium.
Post-procedural 3D TEE