Early discharge (ED) and next-day discharge (NDD) pathways following transfemoral (TF) transcatheter aortic valve implantation (TAVI) have been gaining acceptance among Heart Teams123. We recently demonstrated the safety and feasibility of NDD following TAVI with three different types of commercially available transcatheter heart valves3. However, there is a lack of data on ED and NDD in patients undergoing TAVI using alternative access (A-TAVI). Therefore, this research assessed the safety of an ED/NDD pathway in patients who underwent A-TAVI.
Data from consecutive, all-comers patients who underwent elective A-TAVI between July 2018 and November 2024 were prospectively collected in a dedicated database. Patients followed a fast-track anaesthesia pathway consisting of extubation in the hybrid operating room, 1-hour recovery in the post-anaesthesia care unit, and transfer to the inpatient ward, similar to TF-TAVI under conscious sedation23. Mobilisation was promptly encouraged within four hours following the completion of the procedure, and a transthoracic echocardiogram was performed the following morning. Patients had an electrocardiogram (ECG) shortly after TAVI and again the following day. To qualify for the NDD pathway, patients needed to be ambulatory, capable of self-care, and to meet the following criteria: no new conduction disturbances on their ECG, no uncontrolled arrhythmias (such as rapid atrial fibrillation), and no transient conduction abnormalities on telemetry monitoring23. They also needed to show no signs of haemodynamic instability or major adverse events (such as stroke), and be free of symptoms related to heart failure, ischaemic chest pain, suspected infection, acute kidney injury, or decreased urine output. Stable haemoglobin levels were also required for discharge suitability23.
The primary outcome was 30-day unplanned readmissions. The secondary outcome was exploratory, focusing on differences between cardiac and non-cardiac causes of readmission. To provide better appreciation of the primary outcome, the cohort was analysed based on access site, namely subclavian/axillary, carotid, and transapical, then further analysed considering time-to-discharge, thus, NDD, 48-hour discharge and ≥72-hour discharge.
Outcomes were reported according to Valve Academic Research Consortium-3 definitions4. Institutional review board and ethics committee approval was obtained from the Western University Health Science Research Ethics Board.
Continuous variables are reported as mean±standard deviation and categorical variables are reported as frequencies (%). Comparisons were performed using the chi-square test for categorical variables and analysis of variance for continuous variables. Statistical analyses are two-tailed, and a p-value of <0.05 was considered statistically significant. Statistical analyses were performed using Stata, version 14.1 (Stata Corp).
A total of 85 patients underwent A-TAVI via subclavian/axillary (n=29), carotid (n=21), and transapical (n=35) vascular access. While transapical TAVI patients had a higher prevalence of diabetes mellitus (p=0.013) and previous coronary artery bypass graft surgery (p=0.016), the preprocedural risk profile as assessed by the Society of Thoracic Surgeons score was similar (p=0.30), regardless of access site. There were no differences between the groups in terms of preprocedural atrial fibrillation, right bundle branch block, left bundle branch block, left ventricular ejection fraction (LVEF), the proportion of individuals with an LVEF <35%, and aortic annulus perimeter. All A-TAVI patients received general anaesthesia. In-hospital adverse events and echocardiographic data at hospital discharge were similar between the three A-TAVI groups (Table 1).
A total of 33 patients followed NDD: 16 (48%) subclavian/axillary patients and 17 (52%) carotid patients. Eight (47%) subclavian/axillary patients, 2 (12%) carotid patients, and 7 (41%) transapical patients were discharged 48 hours after TAVI. The length-of-stay was logically higher among transapical patients with a median of 3 (interquartile range [IQR] 3-5) days compared to subclavian/axillary patients with a median of 1 (IQR 1-2) days and carotid patients with a median of 1 (IQR 1-1) day (Table 1).
At 30 days, there were no significant differences in all-cause readmissions when considering discharge pathways (NDD: 6.1%, 48-hour: 18%, and 72-hour: 11%; p=0.09) or according to access site (subclavian/axillary: 14%, carotid: 4.8%, and transapical: 11%; p=0.12). While readmissions were all for cardiac reasons among subclavian/axillary and carotid patients, non-cardiac causes were more common among transapical patients. As expected, the same pattern was observed when analysing the data according to discharge pathways (Table 1). No deaths occurred within 30 days of discharge in either group.
The present study represents the first to report outcomes of A-TAVI patients discharged home the next day or at 48 hours following their TAVI procedure (Central illustration). It underscores the safety of an NDD/ED pathway among a subset of high-risk patients deemed unsuitable for a TF approach. Although patients who were discharged the next day or at 48 hours underwent 100% and 60% subclavian/axillary and carotid access, respectively, those undergoing the transapical approach may need longer monitoring after the procedure, yet close to 50% can be discharged on day 2 following A-TAVI. The NDD/ED strategy was not associated with an increased risk of all-cause readmissions, cardiac and non-cardiac causes of readmission, or deaths up to 30 days of follow-up. We also show the utilisation of three different types of commercially available transcatheter heart valves used for A-TAVI (subclavian/axillary and carotid), representing a novel contribution to the current knowledge.
The main limitation of this study is its small sample size; however, it is the first to report outcomes on NDD/48-hour discharge in a population who underwent A-TAVI. A randomised controlled trial would help to establish the ideal pathway after TAVI; however, as already demonstrated3, in the absence of periprocedural complications that necessitate a clinically indicated prolonged length of stay, conducting such a trial would be challenging. Additionally, this study was carried out in a high-volume centre of excellence for valvular heart disease treatment, where efficient bed turnover is essential for optimising healthcare delivery.
NDD and 48-hour discharge in patients undergoing A-TAVI were associated with similar outcomes at 30 days in terms of 30-day readmissions and mortality, regardless of the type of vascular access. The results further support the expansion of NDD/ED pathways to be considered for all patients undergoing TAVI.
Table 1. Baseline, periprocedural and 30-day outcomes according to access site and discharge pathway.
| Variables | Subclavian/axillary n=29 | Carotid n=21 | Transapical n=35 | p-value | NDD n=33 | 48 hours n=17 | ≥72 hours n=35 | p-value |
|---|---|---|---|---|---|---|---|---|
| Baseline characteristics | ||||||||
| Age, years | 81.4±5.4 | 78.4±5.2 | 79.7±4.9 | 0.36 | 81.7±4.9 | 78.1±8.3 | 79.1±8.6 | 0.18 |
| Female sex | 9 (31) | 13 (62) | 17 (49) | 0.09 | 15 (45) | 9 (53) | 15 (43) | 0.79 |
| Hypertension | 26 (90) | 20 (95) | 35 (100) | 0.15 | 30 (91) | 17 (100) | 34 (97) | 0.28 |
| Diabetes | 3 (10) | 8 (38) | 15 (43) | 0.01* | 7 (21) | 4 (24) | 15 (43) | 0.12 |
| Previous CABG | 4 (14) | 5 (24) | 16 (46) | 0.02* | 3 (9) | 6 (35) | 16 (46) | 0.01* |
| STS-PROM score | 3.7±1.9 | 3.6±1.1 | 4.2±1.5 | 0.30 | 3.7±1.2 | 3.6±0.9 | 4.0±1.9 | 0.52 |
| Electrocardiographic data | - | - | - | - | - | - | - | - |
| Atrial fibrillation | 11 (38) | 6 (29) | 8 (23) | 0.42 | 13 (39) | 2 (12) | 10 (29) | 0.13 |
| No conduction abnormalities | 17 (59) | 12 (57) | 27 (77) | 0.15 | 19 (58) | 13 (76) | 24 (69) | 0.19 |
| Right bundle branch block | 3 (10) | 2 (9.5) | 1 (2.9) | - | 3 (9) | 2 (12) | 1 (3) | - |
| Left bundle branch block | 1 (3.4) | 3 (14) | 0 (0) | - | 4 (12) | 0 (0) | 0 (0) | - |
| Previous permanent pacemaker | 1 (3.4) | 2 (9.5) | 3 (8.6) | 0.64 | 2 (6.1) | 0 (0) | 4 (11) | 0.31 |
| Echocardiographic data | - | - | - | - | - | - | - | - |
| Ejection fraction, % | 55±11 | 59±12 | 56±14 | 0.49 | 57±13 | 59±13 | 54±13 | 0.27 |
| Ejection fraction <35% | 5 (17) | 2 (9.5) | 3 (8.6) | 0.56 | 4 (12) | 2 (12) | 4 (11) | 0.86 |
| Aortic valve area, cm2 | 0.60±0.13 | 0.63±0.13 | 0.59±0.19 | 0.79 | 0.64±0.24 | 0.55±0.19 | 0.61±0.16 | 0.34 |
| Mean gradient, mmHg | 49±20 | 43±10 | 48±16 | 0.44 | 46±15 | 49±21 | 48±15 | 0.81 |
| Computed tomography data | - | - | - | - | - | - | - | - |
| Aortic annulus perimeter, mm | 78.7±6.4 | 76.3±5.9 | 74.1±6.3 | 0.35 | 77.8±6.8 | 74.8±5.6 | 77.9±7.8 | 0.29 |
| Procedural data | ||||||||
| Subclavian/axillary | - | - | - | - | 16 (48) | 8 (47) | 5 (14) | 0.01* |
| Carotid | - | - | - | - | 17 (52) | 2 (12) | 2 (6) | <0.001* |
| Transapical | - | - | - | - | 0 (0) | 7 (41) | 28 (80) | <0.001* |
| General anaesthesia | 29 (100) | 21 (100) | 35 (100) | - | 33 (100) | 17 (100) | 35 (100) | - |
| Valve type and size | ||||||||
| ACURATE neo small (23 mm)a | 1 (3.4) | 0 (0) | 4 (11) | - | 1 (0.3) | 0 (0) | 4 (11) | 0.35 |
| ACURATE neo medium (25 mm) a | 1 (3.4) | 2 (9.5) | 7 (20) | - | 3 (9.1) | 0 (0) | 7 (20) | 0.18 |
| ACURATE neo large (27 mm) a | 4 (14) | 2 (9.5) | 3 (8.6) | - | 2 (6.1) | 2 (12) | 5 (14) | 0.53 |
| Evolut 23 mmb | 1 (3.4) | 3 (14) | 0 (0) | - | 2 (6.1) | 0 (0) | 2 (5.7) | 0.26 |
| Evolut 26 mmb | 3 (10) | 5 (24) | 0 (0) | - | 5 (15) | 2 (12) | 1 (2.9) | 0.20 |
| Evolut 29 mmb | 3 (10) | 2 (9.5) | 0 (0) | - | 3 (9.1) | 2 (12) | 0 (0) | 0.40 |
| Evolut 34 mmb | 1 (3.4) | 1 (4.8) | 0 (0) | - | 2 (6.1) | 0 (0) | 0 (0) | 0.65 |
| SAPIEN 23 mmc | 1 (3.4) | 1 (4.8) | 10 (29) | - | 2 (6.1) | 7 (41) | 3 (8.6) | 0.01* |
| SAPIEN 26 mmc | 12 (41) | 2 (9.5) | 6 (17) | - | 10 (30) | 4 (24) | 6 (17) | 0.44 |
| SAPIEN 29 mmc | 2 (6.9) | 3 (14) | 5 (14) | - | 3 (9.1) | 0 (0) | 7 (20) | 0.19 |
| Predilation | 14 (48) | 7 (33) | 14 (40) | - | 14 (42) | 4 (24) | 17 (49) | 0.22 |
| Post-dilatation | 4 (14) | 4 (19) | 6 (17) | - | 4 (12) | 4 (24) | 6 (17) | 0.58 |
| Pacing | ||||||||
| Temporary venous pacing | 19 (66) | 11 (52) | 35 (100) | <0.001* | 15 (45) | 15 (88) | 35 (100) | <0.001* |
| TAVI wire pacing | 10 (34) | 10 (48) | 0 (0) | 18 (55) | 2 (12) | 0 (0) | ||
| In-hospital adverse events | ||||||||
| New permanent pacemaker# | 0 (0) | 2 (10) | 3 (9.4) | 0.18 | 0 (0) | 2 (12) | 3 (9.7) | 0.32 |
| Vascular complications | 3 (10) | 0 (0) | 0 (0) | 0.20 | 0 (0) | 2 (12) | 1 (2.9) | 0.05 |
| Bleeding | 2 (6.9) | 0 (0) | 2 (5.7) | 0.52 | 0 (0) | 2 (12) | 2 (5.7) | 0.19 |
| Major | 2 (6.9) | 0 (0) | 1 (2.9) | 0.36 | 0 (0) | 2 (12) | 1 (2.9) | 0.49 |
| Minor | 0 (0) | 0 (0) | 1 (2.9) | 0.49 | 0 (0) | 0 (0) | 1 (2.9) | 0.78 |
| Life-threatening | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Stroke/TIA | 3 (10) | 0 (0) | 1 (2.9) | 0.32 | 0 (0) | 2 (12) | 2 (5.7) | 0.03* |
| Transient ischaemic attack | 2 (6.9) | 0 (0) | 0 (0) | 0.31 | 0 (0) | 2 (12) | 0 (0) | 0.02* |
| Non-disabling stroke | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Disabling stroke | 1 (3.4) | 0 (0) | 1 (2.9) | 0.47 | 0 (0) | 0 (0) | 2 (5.7) | 0.02* |
| Discharge echocardiographic data | ||||||||
| Ejection fraction, % | 60±6 | 57±6 | 56±5 | 0.47 | 57±13 | 59±13 | 56±9 | 0.82 |
| Aortic valve area, cm2 | 1.53±0.41 | 1.61±0.33 | 1.40±0.39 | 0.72 | 1.62±0.36 | 1.50±0.34 | 1.52±0.32 | 0.33 |
| Mean gradient, mmHg | 9.4±3.9 | 8.5±4.3 | 9.1±3.7 | 0.73 | 9.5±4.0 | 9.4±3.8 | 8.5±4.2 | 0.60 |
| Paravalvular leakage | - | - | - | - | - | - | - | - |
| None/trace | 19 (66) | 11 (52) | 32 (91) | 0.01* | 22 (67) | 10 (59) | 30 (86) | 0.16 |
| Mild | 10 (34) | 9 (43) | 3 (8.6) | - | 10 (30) | 7 (41) | 5 (14) | - |
| Moderate | 0 (0) | 1 (4.8) | 0 (0) | - | 1 (3) | 0 (0) | 0 (0) | - |
| Length of stay | ||||||||
| 24 hours | 16 (55) | 17 (81) | 0 (0) | <0.001* | - | - | - | - |
| 48 hours | 8 (28) | 2 (9.5) | 7 (20) | 0.28 | - | - | - | - |
| ≥72 hours | 5 (17) | 2 (9.5) | 28 (80) | <0.001* | - | - | - | - |
| Median, days | 1 (1-2) | 1 (1-1) | 3 (3-5) | <0.001* | - | - | - | - |
| Minimum-maximum, days | 1-8 | 1-4 | 2-19 | - | - | - | - | - |
| Overall, 30-day readmissions | 4 (14) | 1 (4.8) | 4 (11) | 0.12 | 2 (6.1) | 3 (18) | 4 (11) | 0.09 |
| Cardiac causes | 4 (14) | 1 (4.8) | 1 (2.9) | 0.21 | 2 (6.1) | 3 (18) | 1 (2.9) | 0.07 |
| New permanent pacemaker§ | 1 (3.6) | 1 (5.9) | 0 (0) | 0.23 | 2 (6.5) | 0 (0) | 0 (0) | 0.42 |
| Congestive heart failure | 2 (6.9) | 0 (0) | 1 (2.9) | 0.74 | 0 (0) | 2 (12) | 1 (2.9) | 0.72 |
| Acute coronary syndrome | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Arrhythmias | 1 (3.4) | 0 (0) | 0 (0) | 0.89 | 0 (0) | 1 (5.9) | 0 (0) | 0.37 |
| Valve-related | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Non-cardiac causes | 0 (0) | 0 (0) | 3 (8.6) | 0.46 | 0 (0) | 0 (0) | 3 (8.6) | 0.23 |
| Stroke/TIA | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Vascular complications | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Infections | 0 (0) | 0 (0) | 2 (5.7) | 0.65 | 0 (0) | 0 (0) | 2 (5.7) | 0.56 |
| Respiratory | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Gastrointestinal | 0 (0) | 0 (0) | 0 (0) | - | 0 (0) | 0 (0) | 0 (0) | - |
| Other | 0 (0) | 0 (0) | 1 (2.9) | 0.93 | 0 (0) | 0 (0) | 1 (2.9) | 0.98 |
| Data are presented as mean±SD, median (interquartile range), or n (%). Some percentages may not add up to 100% owing to rounding. *Indicates statistical significance (p<0.05). #Patients without previous pacemaker (subclavian/axillary n=28, carotid n=19, transapical n=32; NDD n=31, 48 hrs n=17, 72 hrs n=31). §Out of patients without pre- and postprocedural (subclavian/axillary n=28, carotid n=17, transapical n=29; NDD n=31, 48 hrs n=15, 72 hrs n=28) pacemaker. aBy Boston Scientific; bby Medtronic; cby Edwards Lifesciences. CABG: coronary artery bypass grafting; SD: standard deviation; STS-PROM: Society of Thoracic Surgeons Predicted Risk of Mortality; TAVI: transcatheter aortic valve implantation; TIA: transient ischaemic attack | ||||||||
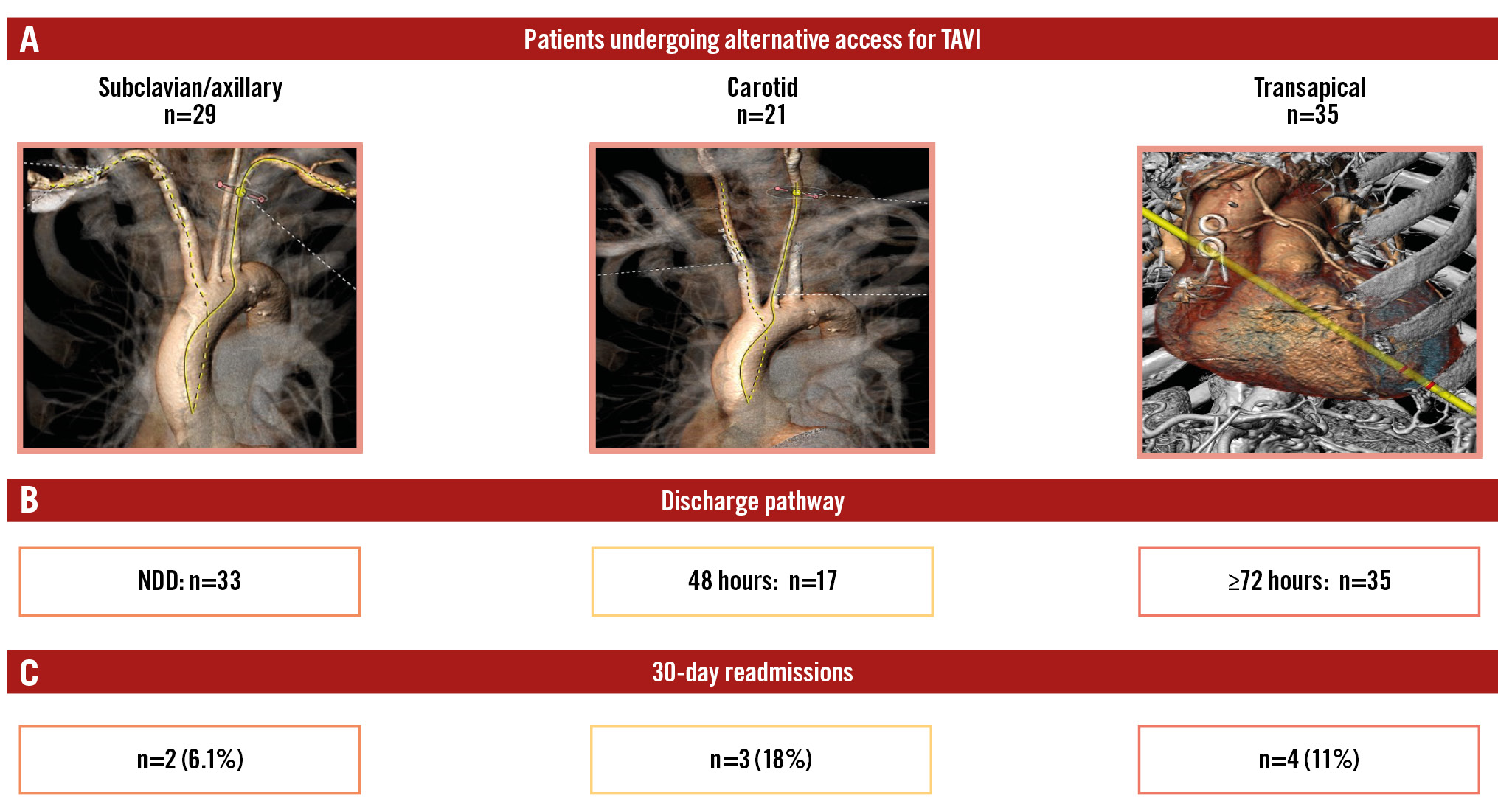
Central illustration. Next-day and 48-hour discharge following alternative access for TAVI. A) Vascular access sites for A-TAVI. B) Discharge pathways. C) 30-day readmission rates. A-TAVI: TAVI via alternative access; NDD: next-day discharge; TAVI: transcatheter aortic valve implantation
Conflict of interest statement
M.W.A. Chu has received speaker honoraria from Medtronic, Edwards Lifesciences, Terumo Aortic, and Artivion Inc. P. Diamantouros is a consultant and proctor for Boston Scientific. R. Bagur is a consultant and proctor for Medtronic. The other authors have no conflicts of interest inherent to the content of this manuscript to declare.