A 74-year-old male with heart failure and left ventricular ejection fraction of 40% presented with exertional chest pain and dyspnoea. The patient had undergone percutaneous coronary intervention to the right coronary artery 12 years earlier following an inferior myocardial infarction. One year ago, they received an implantable cardioverter-defibrillator implantation as secondary prophylaxis after experiencing out-of-hospital cardiac arrest with no evidence of progression in the known one-vessel disease. Coronary angiography revealed a chronic total occlusion (CTO) in a large side branch of the left anterior descending artery (LAD) with a flush occlusion at the ostium of the CTO vessel (Moving image 1). The exact origin of the occluded vessel was unclear because of the flush ostial nature of the CTO, raising the possibility that it could be an intermediate or an early diagonal branch (Figure 1A).
Proximal cap ambiguity is typically addressed using retrograde wiring or intravascular ultrasound (IVUS)-guided cap puncture1. However, in this case, retrograde options were unavailable, and IVUS of the LAD failed to identify the proximal cap of the target occluded vessel because of an extensive segment of deep circumferential calcium at the polygon of confluence (Moving image 2). As a result, IVUS-guided cap puncture was not feasible. Additionally, commonly used solutions, such as balloon-assisted subintimal entry or scratch-and-go, were not viable in this scenario.
To overcome this challenge, intravascular lithotripsy (IVL) was applied along the proximal LAD to disrupt the deeply embedded circumferential calcium previously impenetrable by IVUS (Figure 1B). Considering the coronary anatomy and reduced ejection fraction, 60 pulses were delivered, with pauses every 10 seconds to allow for perfusion recovery. The acoustic pressure waves generated by the IVL catheter and subsequent dilation with a 4.0 mm non-compliant balloon (Moving image 3) resulted in fractures of both superficial and deep calcium, enabling IVUS (Figure 1E) to penetrate deeper into the media and adventitia. As a result, the bifurcation (indicated by a step up in vessel size) and the level of the true ostial CTO proximal cap were successfully identified.
With improved visualisation of the proximal cap, an IVUS-guided puncture was performed using a Gaia Second wire (Asahi Intecc), which crossed the CTO segment into the distal true lumen (Figure 1C, Moving image 4, Moving image 5). In this way, IVL not only helped identify the origin of the CTO but also facilitated wire passage through the fractured calcified cap. A similar approach has been described by Werner and colleagues2, who employed IVL to assist in retrograde wire crossing in a CTO with a severely calcified proximal cap. Ultimately, our procedure was completed using the double-kissing nano-crush bifurcation technique3, with a successful outcome (Figure 1D, Moving image 6-Moving image 7-Moving image 8-Moving image 9-Moving image 10).
Although the use of IVL has been described in side branches to facilitate penetration of heavily calcified proximal caps when the origin of the cap is known4, our case is the first to describe the utility of IVL as a tool to remove proximal cap ambiguity in the presence of long, heavily calcified segments of the parent artery when the site of the CTO proximal cap is entirely unclear and traditional IVUS-guided or retrograde options are unfeasible or have failed.
The term 'Stone whisper technique' was chosen to symbolise the precise use of IVL to address calcified vessels in these situations, like whispering to a stone to gently break it apart without causing undue harm or disturbance. The idea of 'whispering' may also be linked to mythological or allegorical roots, such as ancient tales where wisdom or gentle actions overcame seemingly immovable obstacles.
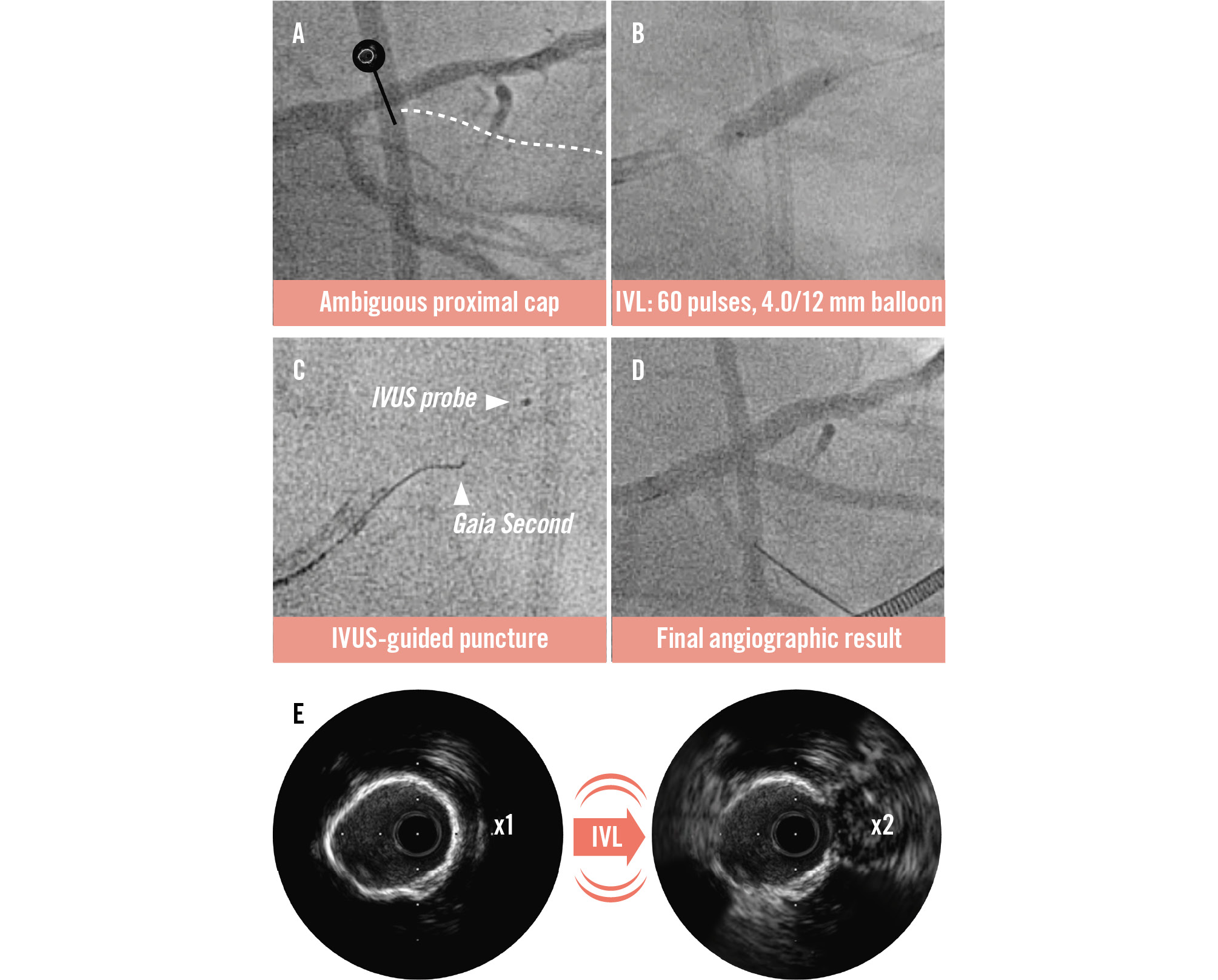
Figure 1. The stone whisper technique. A) Angiography showing a flush occlusion of the CTO vessel. The marker corresponds with the cross-sectional IVUS image (E). B) Application of IVL, with a 4.0 mm diameter/12 mm length balloon, disrupting the deep circumferential calcium. C) Successful advancement of the Gaia Second wire through the CTO segment. D) Final angiographic result after the DK nano-crush technique. E) IVUS imaging failed to penetrate because of circumferential calcium but revealed the proximal cap after calcium cracking with IVL. CTO: chronic total occlusion; DK: double kissing; IVL: intravascular lithotripsy; IVUS: intravascular ultrasound
Conflict of interest statement
The authors have no conflicts of interest to declare.
Supplementary data
To read the full content of this article, please download the PDF.
Moving image 1. Setup shot. Retrograde filling of target vessel with ambiguous proximal cap.
Moving image 2. IVUS run. Failed visualisation of the proximal cap due to circumferential calcium.
Moving image 3. Application of IVL.
Moving image 4. IVUS-guided puncture after IVL.
Moving image 5. Successful wiring into the true lumen.
Moving image 6. Antegrade shot after successful wiring and predilation.
Moving image 7. DK nano-crush – before deployment of side branch stent.
Moving image 8. DK nano-crush – deployment of main vessel stent.
Moving image 9. DK nano-crush – second kissing balloon inflation.
Moving image 10. Final result.
