Abstract
Aims: We aimed to estimate the rate of renal artery adverse events following renal denervation with the most commonly applied radiofrequency catheter system based on a comprehensive review of published reports.
Methods and results: We reviewed 50 published renal denervation (RDN) trials reporting on procedural safety including 5,769 subjects with 10,249 patient-years of follow-up. Twenty-six patients with renal artery stenosis or dissection (0.45%) were identified of whom 24 (0.41%) required renal artery stenting. The primary meta-analysis of all reports indicated a 0.20% pooled annual incidence rate of stent implantation (95% CI: 0.12 to 0.29% per year). Additional sensitivity analyses yielded consistent pooled estimates (range: 0.17 to 0.42% per year). Median time from RDN procedure to all renal intervention was 5.5 months (range: 0 to 33 months); 79% of all events occurred within one year of the procedure. A separate review of 14 clinical trials reporting on prospective follow-up imaging using either magnetic resonance imaging, computed tomography or angiography following RDN in 511 total subjects identified just 1 new significant stenosis (0.20%) after a median of 11 months post procedure (one to 36 months).
Conclusions: Renal artery reintervention following renal denervation with the most commonly applied RF renal denervation system (Symplicity) is rare. Most events were identified within one year.
Introduction
Hypertension remains a global health crisis with well over one billion adults afflicted and fewer than 30% controlled1 despite the availability of safe and effective drug therapies. Autonomic nervous system modulation via percutaneous renal denervation (RDN) has been shown to reduce blood pressure in animal models and in clinical trials and represents a potentially useful adjunctive therapy option2,3. Recent prospective trials have shown statistically and clinically significant reductions in both office and 24-hour blood pressure following RDN with radio frequency (RF) as compared to sham control in patients with uncontrolled hypertension according to the World Health Organization classification4 in both the presence and absence of concomitant antihypertensive drug therapy5,6. These and other clinical trials have also reported minimal safety risk in terms of both procedural complications and vascular events. However, RF ablation systems apply energy to the renal arterial wall and thus impose an inherent risk of permanent damage. Therefore, scrutiny of all potential adverse safety events is an important part of establishing the clinical relevance of the RDN procedure.
The incidence of serious renal artery adverse events following RDN is uncertain and difficult to elucidate, since few events have been reported. RDN systems have been approved and applied for clinical use in multiple countries since 2008. Hence, published clinical experience is available on several thousand patients with follow-up duration ranging up to three years. We estimated the occurrence of renal artery adverse events following denervation with common RF systems to determine whether RF ablation increases the risk of renal artery stenosis in the population with uncontrolled hypertension.
Methods
A search of the MEDLINE database was performed using the terms “renal” AND “denervation” from January 2009 to January 2019 following PRISMA guidelines7. Prospective trials and case reports cited in one previous report8 and a recent meta-analysis of RDN trials9 were also reviewed. The search included both randomised and non-randomised trials and registries that employed either the Symplicity Flex™ and/or the Symplicity Spyral™ RF denervation systems (Medtronic, Santa Rosa, CA, USA). Other RF devices and/or devices using other sources were not included. Reports that did not specifically address safety, including the presence or absence of renal artery events, and secondary analyses of previously reported studies were excluded. A case series (n=51) of RDN with the Symplicity Flex device employed via non-standard brachial access10 was also excluded, although no preprocedural or post-procedural adverse events were reported. If a trial was updated for safety and efficacy after the initial report, unique events from each report were counted. Updated reviews of the SYMPLICITY HTN-3 trial and the Global SYMPLICITY Registry were also included. Individual case reports of renal artery damage were tabulated separately and not included in the meta-analysis. Stenoses were counted if they were classified as “significant”, greater than 50%, resulted in stent implant or if not specified. If reported, the association of the event with pre-existing non-significant renal artery stenosis at the time of the procedure was recorded.
The pooled incidence rate of any renal artery stent implantation was determined by meta-analysis of the study-level incidence rates. The primary analysis was a fixed-effects meta-analysis on untransformed rates using the inverse variance method for pooling. Due to several studies reporting zero events, a continuity correction of 0.5 was applied to each study with a zero event rate. Several sensitivity analyses were performed to evaluate the robustness of the pooled incidence estimate (Supplementary Appendix 1). Other data are summarised as raw counts and means (SD) or median (minimum, maximum). Meta-analyses were performed in R, version 3.5.0 (R Foundation for Statistical Computing, Vienna, Austria) using the “meta” package (version 4.9-3).
Results
INCIDENCE OF RENAL ARTERY DAMAGE FOLLOWING RF RDN
Fifty published reports detailing procedural safety with Symplicity Flex or Spyral systems were identified and included in the primary meta-analysis (Figure 1). Median follow-up for the total of 5,769 patients was 6 months (range: 1-36 months) amounting to 10,249 patient-years of net follow-up. Ten of these studies (20%) reported 26 total cases of renal artery damage (0.45%) including 19 cases of stenoses (0.33%) and 7 dissections (0.12%). Twenty-four of the 26 cases with stenosis or dissection resulted in stent implant (0.42%), including one case with 2 stents. Six of the 24 cases resulting in stent implant (25%) were from randomised trials with the rest reported in non-randomised trials or registries. The primary meta-analysis for all reports resulted in an annual incidence rate of renal stenting of 0.20% per year (95% CI: 0.12 to 0.29%) (Figure 2). Additional sensitivity analyses revealed consistent results (Supplementary Figure 1, Supplementary Figure 2).
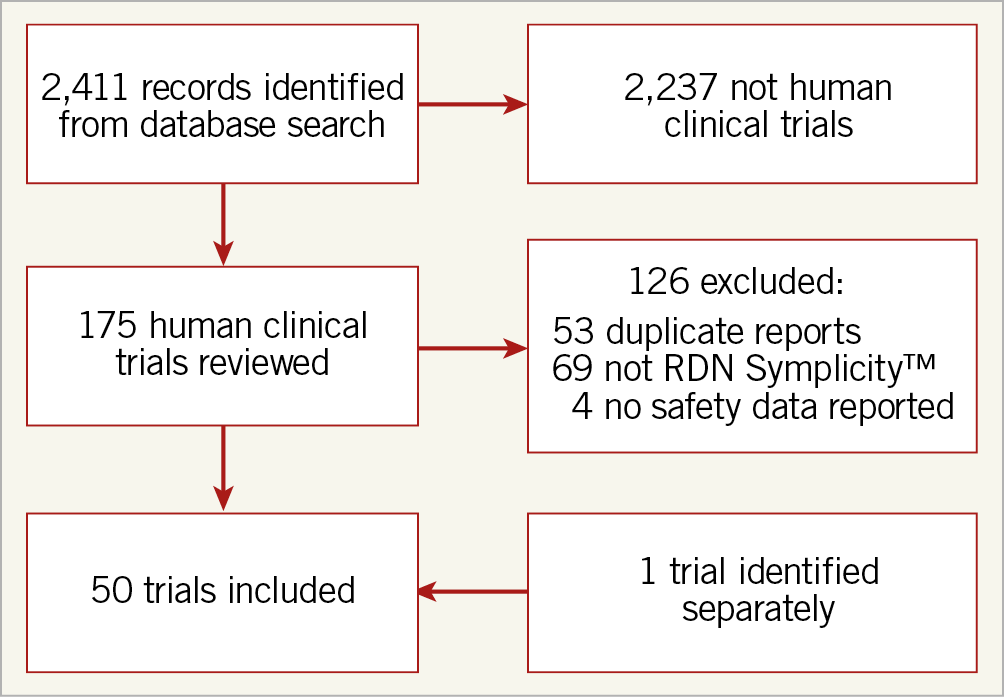
Figure 1. PRISMA block diagram.
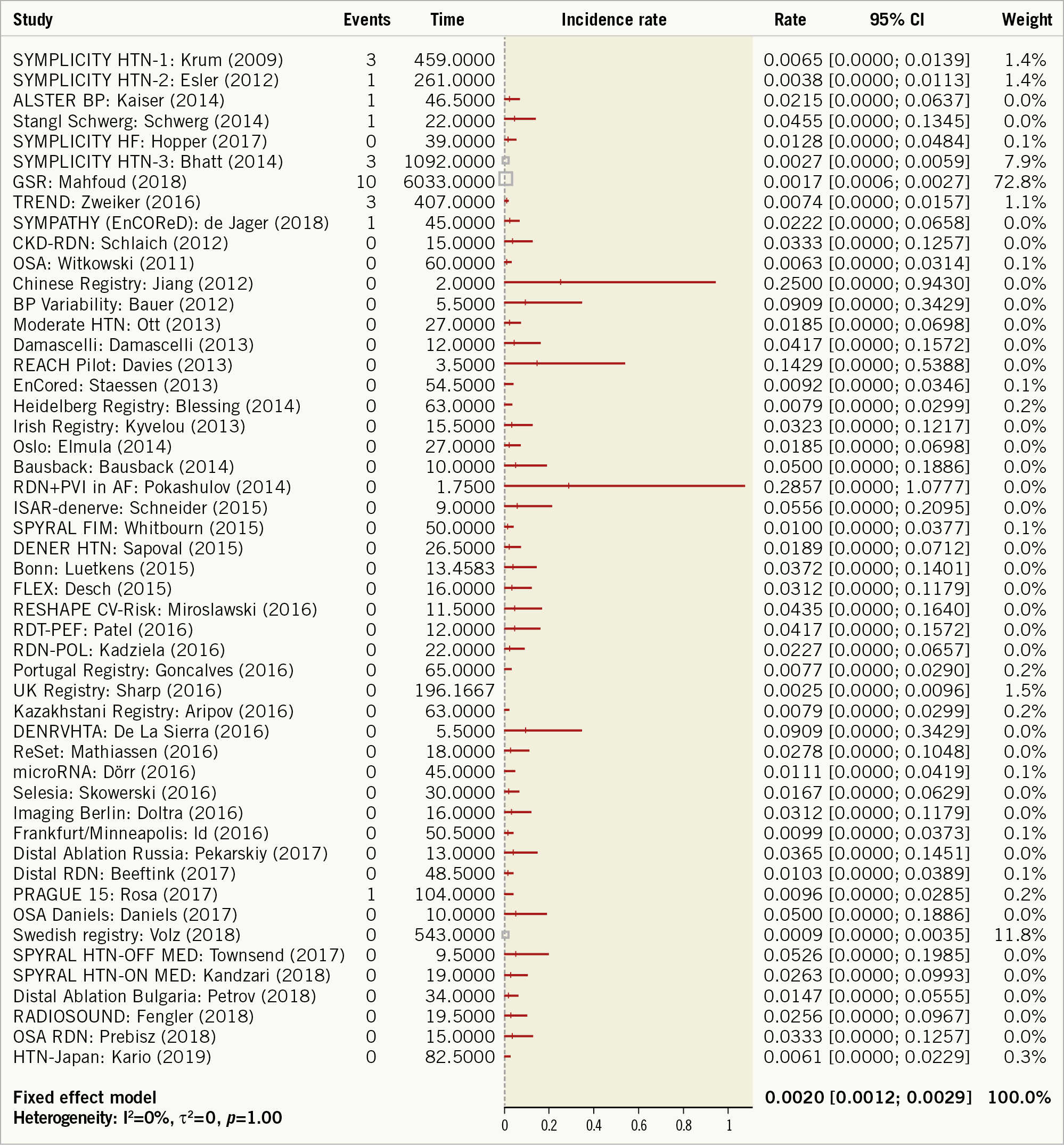
Figure 2. Forest plot of incidence of stent implant following RF renal denervation from 50 published trials reporting event occurrence representing 5,769 patients and 10,249 patient-years of total patient follow-up. Incidence rate estimated using a fixed effects meta-analysis on untransformed values with a continuity correction of 0.5 for studies with zero events. Study time is reported in units of patient-years and event rates are events per patient-year.
POST-PROCEDURAL RENAL ARTERY EVENTS
Besides the 24 patients receiving stents identified from published trials and registries, an additional 11 individual cases of renal artery stenosis have also been reported (Table 1). Stents were implanted in 10 of the 11 case subjects, including two cases in which two stents were implanted. The median time to stenosis detection for the case reports was 5.0 months (range 3 to 28 months) (Table 1). Most cases were identified after recurrent hypertension, occasionally with concomitant symptoms. Combining case reports and clinical studies, renal artery damage following denervation with the Symplicity Flex catheter has been reported in 37 subjects, including 34 cases of stent implantation. Of these 34 cases, the median time to renal artery stenting was 5.5 months (range 0-33 months) (Figure 3). Of the 34 patients receiving stents, 25 resulted in stent implant at least one month after the RDN procedure. The presence or absence of baseline renal stenosis was not reported in 3 of the 25 post-procedural stenting cases, while 8 of the remaining 22 (36%) stented cases reported some baseline stenosis or a previous history of renal artery stenting.
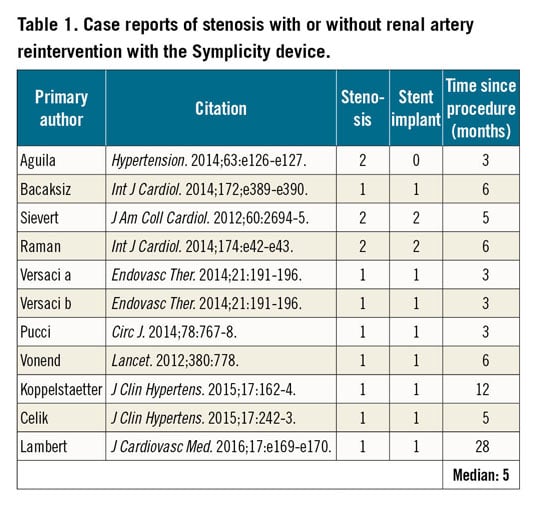
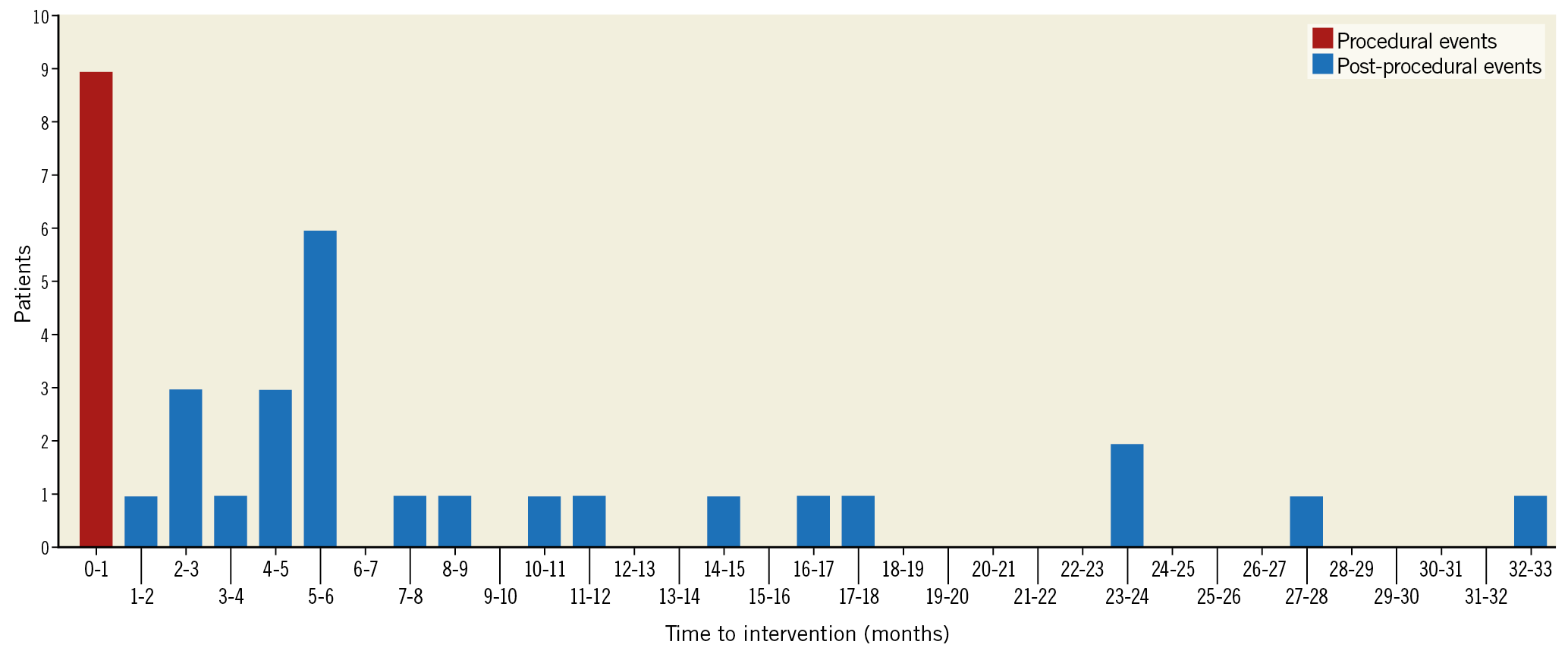
Figure 3. Histogram of time from RDN procedure to renal artery stenting for 34 cases. Data were derived from both case reports and clinical trials reporting time of stent implant. Red bar at 0 to 1 month includes 9 stents implanted during the procedure. All other events were reported at least 1 month after the procedure (median: 5.5 months).
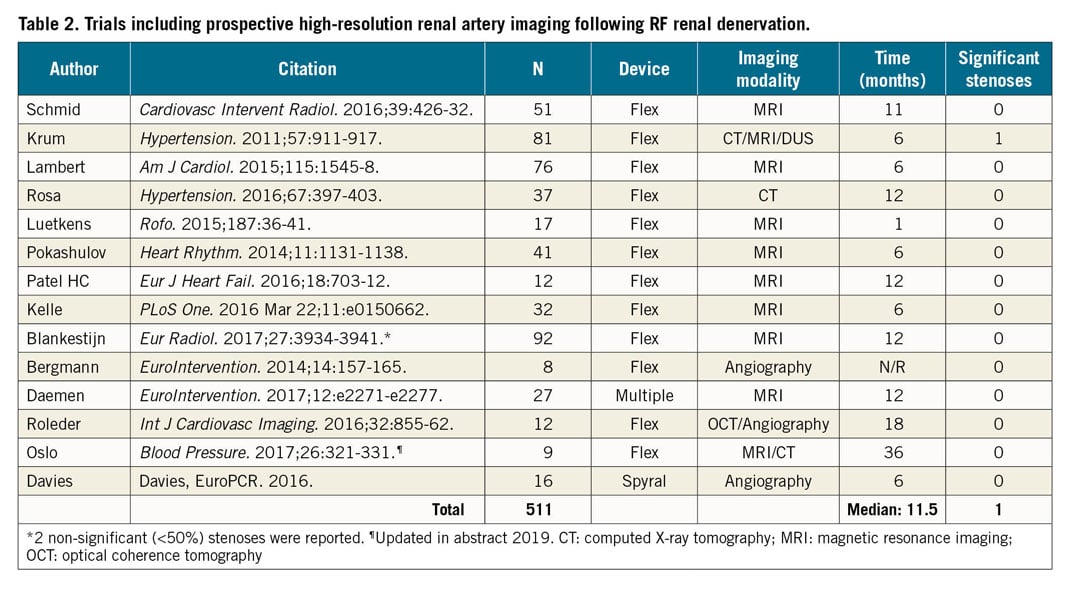
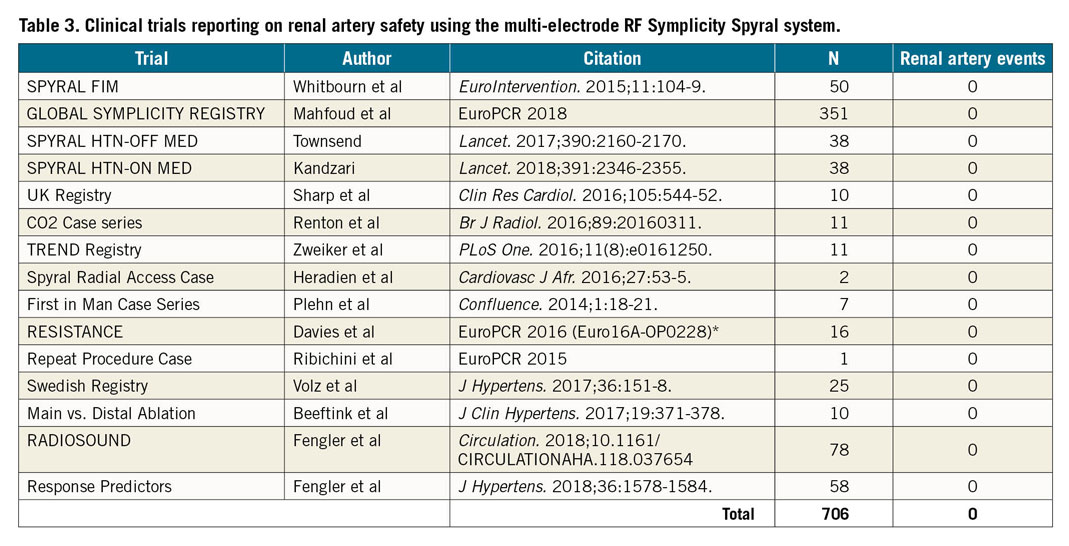
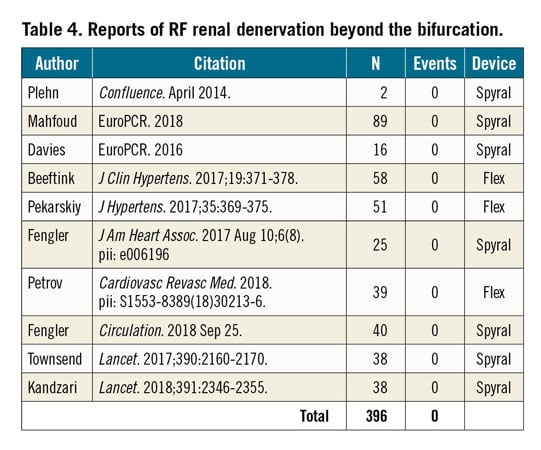
A separate analysis identified 14 studies that reported prospective performance of high-resolution renal artery imaging following RDN using either repeat angiography, magnetic resonance imaging or computed X-ray or optical coherence tomography (Table 2). A total of 511 subjects were studied with one significant stenosis observed (0.2%) via computed X-ray tomography after a median of 11 months post procedure (range: 1-36 months) (Table 2). No cases of stenosis or dissection have been reported to date involving the second-generation multi-electrode Symplicity Spyral system among 15 reports including 706 patients (Table 3). Additionally, 10 reports including 396 subjects have reported on RF RDN therapy beyond the main bifurcation with no renal reinterventions reported (Table 4).
PROCEDURAL EVENTS
Stents were delivered during the RDN procedure in 9 of 34 (26%) patients including 7 cases of acute renal artery dissection (Figure 3). Procedural access-site complications were reported in 1.4% (82 of 5,769) of all subjects from the 50 reports.
Discussion
Renal artery stenosis, primarily occurring in the proximal segment, is common in hypertensive subjects and may lead to serious adverse outcomes including worsening hypertension, reduced renal function and renal necrosis. This is the first analysis to estimate the rate of reported adverse renal events following RF RDN with the most widely applied RDN system and to evaluate whether RDN increases the risk of renal artery stenting in this population. Meta-analysis of 50 trials, including a net population of 5,769 patients and 10,249 patient-years of data, estimated an annual incidence of renal artery stenting following RF RDN of 0.20%. Time to reported stenting ranged from 0 to 33 months with most events occurring within 6 months post procedure (Figure 2). The small number of renal artery adverse events uncovered in this analysis supports the general safety of the RF RDN procedure, especially when considered relative to the well-substantiated cardiovascular risks associated with sustained uncontrolled hypertension11.
Many of the events were identified by additional imaging following symptomatic recurrence of hypertension. Thus, it is possible that some stenoses not accompanied by recurrent hypertension or worsening renal function remain undetected and unreported. However, we also performed a separate review of prospective high-resolution imaging totalling 511 patients following RF RDN that identified just one case of significant renal artery stenosis. Since these were non-selected subjects of varying risk, the overall results imply that significant stenosis caused by RDN is rare. The absolute rate of occurrence of other non-renal adverse events such as access-site complications was also uncommon (1.5%) and consistent with prior reports of femoral access-site complications12.
Renal artery injury following RF denervation could be caused by several mechanisms including physical trauma created by the guide catheter, denervation catheter or guidewire or by the RF energy applied to the vessel wall. Nine of 34 reported stent implants occurred during the procedure (26%). Due in part to the low rate of incidence, it was also difficult to determine from our analysis whether reported renal artery stent implants occurring after the procedure were specifically due to the procedure or rather simply due to natural disease progression. Indeed, over one third (36%; 8 of 22) of renal stent implant cases reporting basal renal artery morphometry indicated basal stenosis (<50%) at the site of the stenting prior to RDN or renal stenting prior to RDN. We also report one case of renal artery stenosis and one case of dissection that were not associated with stent implant. Overall, these data indicate that not all renal artery vascular events reported after RDN are entirely related to the procedure. Notably, the landmark Cardiovascular Outcomes in Renal Atherosclerotic Lesions (CORAL) trial found that renal artery stenting did not confer a significant benefit with respect to the prevention of clinical events in patients with either hypertension or chronic kidney disease (CKD)13. Therefore, the clinical course following detection of renal stenosis should be considered carefully within the context of the individual patient history, risk and degree of stenosis, although all patients should be monitored for clinical signs of new or worsening renal stenosis.
The present analysis includes procedures performed with the first-generation single electrode RF catheter system that was applied primarily in the main renal artery. However, more recent reports have focused on the potential to increase therapy efficacy by treating the distal portion of the main renal artery and the branches beyond the primary bifurcation using the more technically advanced second-generation multi-electrode system4,5. This procedural advance has led to particular concerns over the risk of a distal branch stenosis and further uncertainty around appropriate treatment for a stenosis in such a difficult to access location. Notably, a subset of the patients included in the present analysis (n=706) (Table 3) was treated with the newer-generation multi-electrode Symplicity Spyral catheter, with no renal artery events reported. Likewise, the present analysis included a subgroup of patients with treatment beyond the main bifurcation (396 patients from 9 reports) (Table 4) with no reported adverse events in the distal arteries. Recent RDN trials have also allowed enrolment of patients with accessory renal arteries greater than 3 mm in diameter. These eligible arteries were treated in the most recent trials with no events reported4,5. These preliminary results indicate that safety with second-generation devices and more experienced proceduralists could lead to a progressively lower incidence of adverse renal artery events over time, although longer-term data are required. More prospective high-resolution image-based evaluation of stenosis is planned for ongoing prospective sham-controlled trials in the hypertensive population.
Comparable data for the natural incidence of renal artery adverse events in the hypertension population are scarce. Estimates of the incidence of renal artery stenosis in the hypertensive population range widely from approximately 0.5 to 5% per year14. In the SPYRAL HTN-OFF and HTN-ON MED trials4,5, a combined 0.9% (7 out of 806) of patients were excluded from participation based on identification of significant renal artery stenosis >50% prior to randomisation. Another older report published before the widespread introduction of statin therapy for hyperlipidaemia estimated progression of non-significant stenosis of less than 60% to stenosis greater than 60% to be roughly 20% per year15. Combining these reported values provides an estimate of the annual incidence of new severe stenosis between 0.10% and 1.0% per year. A separate estimate of renal artery stenosis in the Medicare population indicated an incidence of renal stenosis of 0.37% per year16. Finally, a study of 14,152 patients undergoing cardiac catheterisation who were screened for renal stenosis reported significant progression of existing stenosis or new stenosis in 133 patients after an average of 2.6 years, or an incidence of approximately 0.36% per year17. This range of estimates is comparable with the present estimates and suggests that RF RDN may not dramatically increase the rate of renal artery adverse events in the population with uncontrolled hypertension.
Previous animal and clinical investigations have demonstrated acute vessel damage following RF RDN. Histological evidence from normotensive pigs undergoing RDN with the Symplicity Flex catheter resulted in endothelial damage that recovered within seven days and damage to the media that peaked within seven days but decreased progressively, thereby suggesting complete healing of the arterial wall and soft tissue by 180 days18,19,20,21. Human studies of the renal arteries using optical coherence tomography and intravenous ultrasound immediately following RDN with the first-generation Symplicity Flex catheter identified a low incidence of vasospasm, microdissection, lumen narrowing, intimal oedema and micro-thrombus22,23. The present analysis suggests that these acute micro injuries are probably transient and have minimal clinical sequelae. Furthermore, randomised trials of RDN have shown similar major adverse event rates between RDN and sham control groups, although these trials were underpowered to show non-inferiority4,5,24. These findings suggest that the occurrence of adverse events following RF denervation is low enough to require a very large sample size to demonstrate non-inferiority to control in a prospectively designed trial and that carefully selected and pre-specified objective performance goals may be more appropriate trial safety outcomes.
Limitations
Our analysis has important limitations. Clinical trials and registries do not always mandate renal artery imaging of asymptomatic patients and therefore renal artery abnormalities following the RF RDN procedure might be missed. We have therefore included an analysis of available case reports of incidental or symptomatic discovery of renal artery stenosis. Also, prospective imaging has identified only one event to date (Table 2). Subclinical weakening of the renal artery wall might not become clinically manifest for several months or years, so the current estimated rates could change as trials with longer follow-up are reported. However, we also performed a separate meta-analysis only including trials with ≥12 months of follow-up that resulted in a similar result (Supplementary Figure 2). The large number of studies with zero events poses complexity for statistical pooling of incidence rates, with no universally accepted approach for handling such meta-analyses25. However, our results were consistent with several sensitivity analyses, with pooled estimates ranging between 0.17% per year and 0.42% per year (Supplementary Appendix 2). Events were not adjudicated, although only studies that specifically reported renal event occurrence, or lack thereof, were included. Likewise, most studies did not elaborate on the possible mechanistic or procedural causes of the stenotic event. Other RDN systems, including other RF devices, ultrasound, and neurotoxin injection, were not included in this analysis since the net relative estimated population size in published data is much lower than that for RF systems, and thus too low to estimate rates of occurrence accurately. Also, pooling event data among different systems with different designs and energy sources could be misleading, since the safety of each approach is probably unique to a specific device design. The present analysis was also limited to renal artery damage; review of renal function was beyond the present scope. However, recent meta-analyses have also found minimal reductions in renal function following RDN9,26.
Conclusions
The real-world reported incidence of significant renal artery stenosis or dissection, including events resulting in renal artery stenting following renal denervation procedures with the most commonly applied RF renal denervation system is estimated to be 0.20% per year. This estimate is comparable to the reported natural incidence of events in an untreated hypertensive population. Most reported events were identified within one year.
|
Impact on daily practice The clinical decision to refer a patient for percutaneous renal denervation should be based on a clear understanding of the long-term risks as well as the potential benefits of the procedure. Beyond recent reports of good clinical efficacy in terms of blood pressure reduction from randomised sham-controlled trials, this meta-analysis indicates that concerns about renal artery damage resulting from the procedure should be minimal. Renal denervation may thus be considered for a wide range of patients with uncontrolled hypertension including younger patients with lower cardiovascular risk. |
Conflict of interest statement
M. Böhm reports institutional support for the conduct of clinical trials from Medtronic. R.R. Townsend, A. Walton and J. Weil receive honoraria from Medtronic for serving on the medical advisory board. D.A. Hettrick and G.L. Hickey are employees of Medtronic. A.S.P. Sharp receives research grants and speaker fees from Medtronic. P.J. Blankestijn receives honoraria from Medtronic for serving on the medical advisory board, paid to the institution. G. Mancia receives speaker fees from Medtronic.
Supplementary data
To read the full content of this article, please download the PDF.