A 64-year-old female with chronic kidney disease was scheduled to undergo stenting of a severely calcified lesion in the left anterior descending coronary artery following “preparation” of the lesion by orbital atherectomy performed with the Diamondback 360® Coronary Orbital Atherectomy System (OAS), 1.25 mm Classic Crown (Cardiovascular Systems, Inc., St. Paul, MN, USA) (Figure 1A) (pre- and post-OAS angiography: Figure 1B-1C and Figure 1B’-1C’, respectively). The first run was performed at 80,000 rpm for 25 s followed by the second run at 120,000 rpm for 25 s. A 2.75×38 mm everolimus-eluting stent (XIENCE; Abbott Vascular, Santa Clara, CA, USA) was successfully implanted. Optical coherence tomography (C7-XR system, C7 Dragonfly™ catheter; LightLab Imaging, St. Jude, Minneapolis, MN, USA) was performed before and after OAS. Figure 1D and Figure 1D’ show the thinning of a mixed calcified plaque (cross-sections corresponding to the dotted line in Figure 1C and Figure 1C’) (*wire artefact). In order to characterise changes in tissue components better, light attenuation was quantified circumferentially at different depths from the lumen surface using QCU-CMS software (Medis, Leiden, The Netherlands). Spread-out maps of tissue layers every 100 μm in the vessel wall are colour-coded according to their attenuation coefficient μt (Figure 1E-1G and Figure 1E’-1G’; *wire artefact) in an attempt to differentiate the mixed calcified plaque from the relatively low light-attenuating layer underlying it. Changes in light attenuation of the most superficial layer (Figure 1F-1F’) suggest the ablation of the light-attenuating tissue (yellow and red area decreased, and blue area appeared). At deeper levels, no significant change was observed (Figure 1G-1G’).
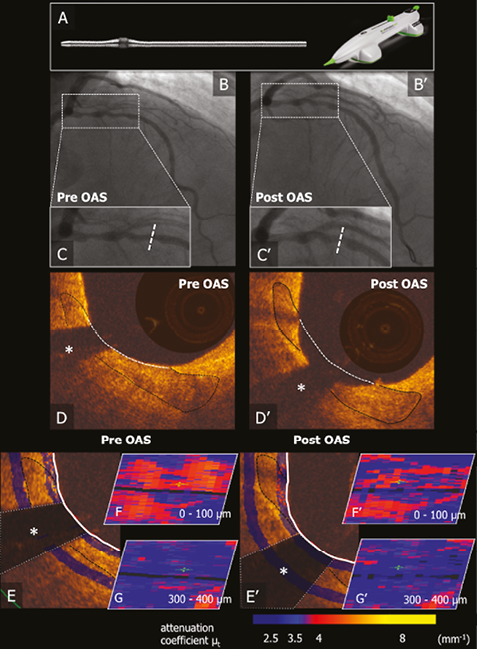
Figure 1. Impact of the orbital atherectomy system on a coronary calcified lesion. A) Diamondback 360 OAS, 1.25 mm Classic Crown. B) and C) Pre- and post-OAS angiography. D) Corresponding OCT cross-sections. E-G) Light attenuation analysis.
Guest Editor
This paper was Guest Edited by Antonio Colombo, MD; Interventional Cardiology Unit, EMO-GVM Centro Cuore Columbus and San Raffaele Scientific Institute, Milan, Italy.
Conflict of interest statement
R. Shlofmitz has received speaker’s honoraria from Cardiovascular Systems Inc. and St. Jude Medical. The other authors have no conflicts of interest to declare. The Guest Editor has no conflicts of interest to declare.