A 64-year-old male with Churg-Strauss syndrome (CSS) presented with worsening dyspnoea without chest pain besides having long-standing asthma. There were no cardiovascular risk factors. The electrocardiogram showed signs of prior anterior infarction. Echocardiography demonstrated severely depressed left ventricular function (ejection fraction 30%). Multislice cardiac computed tomography revealed a giant coronary aneurysm (Figure 1A and Figure 1B) of the left circumflex coronary (LCX) artery of 4 cm diameter with mural thrombi (Figure 1B) and also aneurysmatic changes of the right coronary artery (RCA) with proximal occlusion (Figure 1 A). Coronary angiography showed aneurysmatic changes of the LCX with collateral filling of distal RCA and mid-segment occlusion of the left anterior descending (LAD) (online Figure 1C and 1D, Moving image 1 - Moving image 3). Single-photon emission tomography confirmed an ischaemic cardiomyopathy with irreversible defects. Treatment was carried out medically, and an internal cardioverter-defibrillator was implanted.
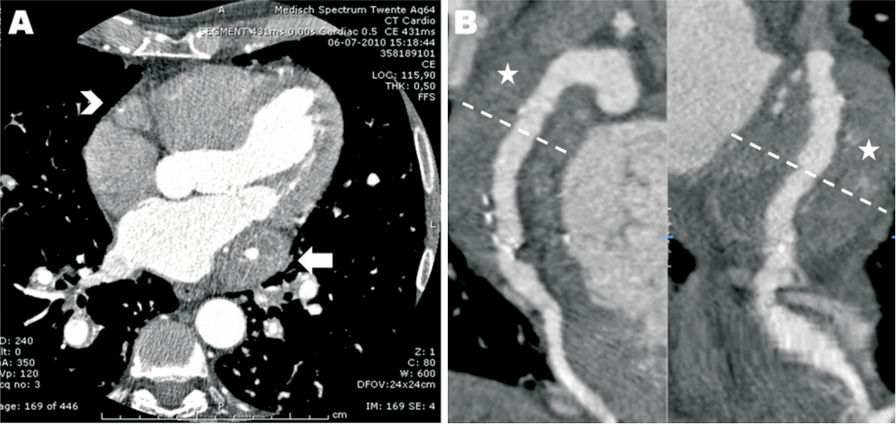
Figure 1. Multislice cardiac computed tomography imaging (A, B) showed a giant coronary aneurysm of the LCX artery (arrow in A) with a diameter of 4 cm and mural thrombi (asterisk in B) and aneurysmatic changes of the RCA with proximal occlusion (arrowhead in A).
Coronary aneurysms are uncommon; they are usually due to atherosclerotic disease and only in a minority of cases are they the result of an autoimmune vasculitis1. CSS is a rare small-vessel vasculitis with asthma and eosinophilia2,3. There are only a few reports with CSS and involvement of major coronary vessels with aneurysmatic changes1-3. The toxic effects of eosinophils on the coronary wall may result in aneurysmatic enlargement1-3. This case describes extensive coronary involvement leading to an ischaemic cardiomyopathy, probably due to thrombotic occlusions and distal coronary embolisations1.
Conflict of interest statement
The authors have no conflict of interest to declare.
Online data supplement
Figure 1 C and Figure 1 D. Coronary angiography (with CLS guiding catheter) also showed extensive aneurysmatic changes of the LCX artery (arrow in C, D) with collateral filling of distal RCA which is proximally occluded (arrowhead in C, D). The LAD showed mid-segment occlusion with minor collateral filling of the distal part (asterisk in C, D).
Moving image 1. Coronary angiogram RCA.
Moving image 2. Coronary angiogram LCA#1.
Moving image 3. Coronary angiogram LCA#2.
